
Abstract
Objectives:
To prevent aesthetic and functional deformities, precisely closed reduction is crucial in the management of nasal fractures. Plain film radiography (PF), ultrasonography (USG), and computed tomography can help confirm the diagnosis and classification of fractures and assist in performing closed reduction. However, no study in the literature reports on precisely closed reduction assisted with PF measurements under the picture archiving and communication system (PACS).
Methods:
We retrospectively evaluated 153 patients with nasal bone fracture between January 2013 and December 2017. Surgeons conducted precisely closed reduction assisted with PF measurement of the distance between the fracture site and nasal tip under PACS on 34 patients (group A). Another group on 119 patients were reduced under surgeon’s experience (group B).
Results:
No significant differences in age, gender, Arbeitsgemeinschaft fur Osteosynthesefragen (AO) classification, and reduction outcome were observed between group A and group B (P > .05). The operative time of the group A was significantly lower (12.50 ± 4.64 minutes) compared to group B (23.78 ± 11.20 minutes; P < .001). After adjusted age, gender, and AO classification, patients in group A scored 10.46 minutes less on the operative time than those in group B (P < .001). In addition, the severity of nasal bone fracture (AO classification, β = 3.37, P = .002) was positive associated with the operative time.
Conclusions:
In this study, closed reduction in nasal bone fracture assisted with PF measurements under PACS was performed precisely, thereby effectively decreasing operative time and the occurrence of complications. This procedure requires neither the use of new instruments or C-arm nor USG or navigation experience. Moreover, reduction can be easily performed using this method, and it requires short operative time, helps achieve great reduction, less radiation exposures, and is cost-effective.
Introduction
Nasal bone fracture is the most common type of facial fracture. However, it is commonly misdiagnosed, and appropriate treatment timings are hard to be determined due to nasal swelling. In Taiwan, individuals have easy access to health care services, and most patients who sustain traumas will immediately seek medical assistance. With thoroughly history taking and cautious physical examinations are adequate for the diagnosing of nasal fractures. Plain film radiography (PF), computed ultrasonography (USG), and computed tomography (CT) can help confirm the diagnosis, help classifying the fracture types, and assist in fracture reduction. Appropriate surgical interventions are the key in the management of nasal fractures, preventing aesthetic and functional deformities. In our patient series, the fracture position was precisely measured on PF under the picture archiving and communication system (PACS), and closed reduction of nasal bone fracture was easily and accurately performed. After a review of literatures, we found that this method has not been reported before. Thus, this report indicates our method, which can facilitate precise fracture reduction, decreasing the occurrence of tissue trauma and related swelling, and lower the rates of complications, such as undercorrection, overcorrection, and deviation.
Materials and Methods
Nasal Bone Classification
Several classification systems are available for the classification of nasal fractures, including Stranc and Robertson, 1 Murray et al, 2 and Rohrich and Adams. 3 The Arbeitsgemeinschaft fur Osteosynthesefragen (AO) foundation has provided a simple classification system for clinical findings in 2009 (Figure 1). We used this system to evaluate the types of bone fracture in our patients; the treatments were based on our nasal bone fracture algorithm (Figure 2 ).
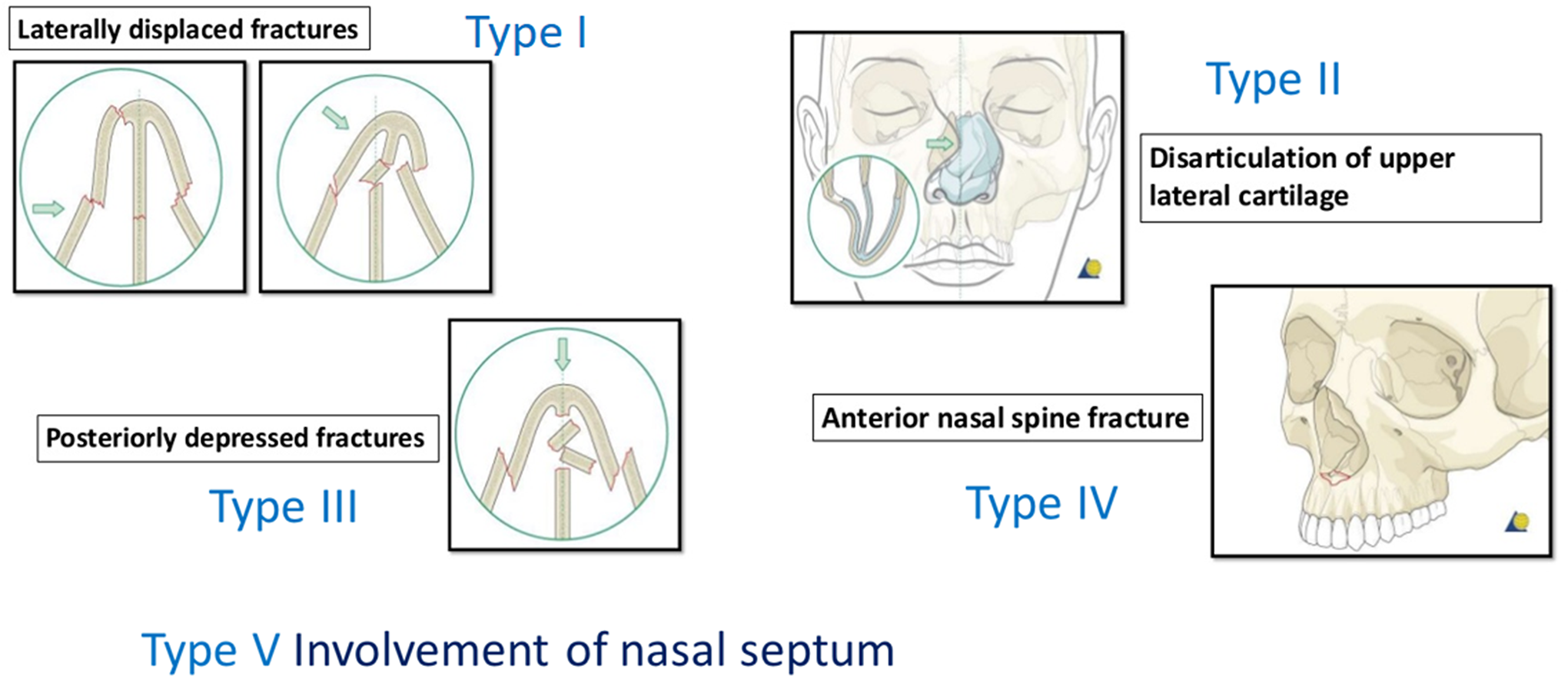
AO (Arbeitsgemeinschaft fur Osteosynthesefragen) surgery provides a simple classification system based on clinical findings (2009). (1) Laterally displaced; (2) Posteriorly depressed fractures; (3) Disarticulation of upper lateral cartilage; (4) Anterior nasal spine fracture; and (5) Involvement of nasal septum.
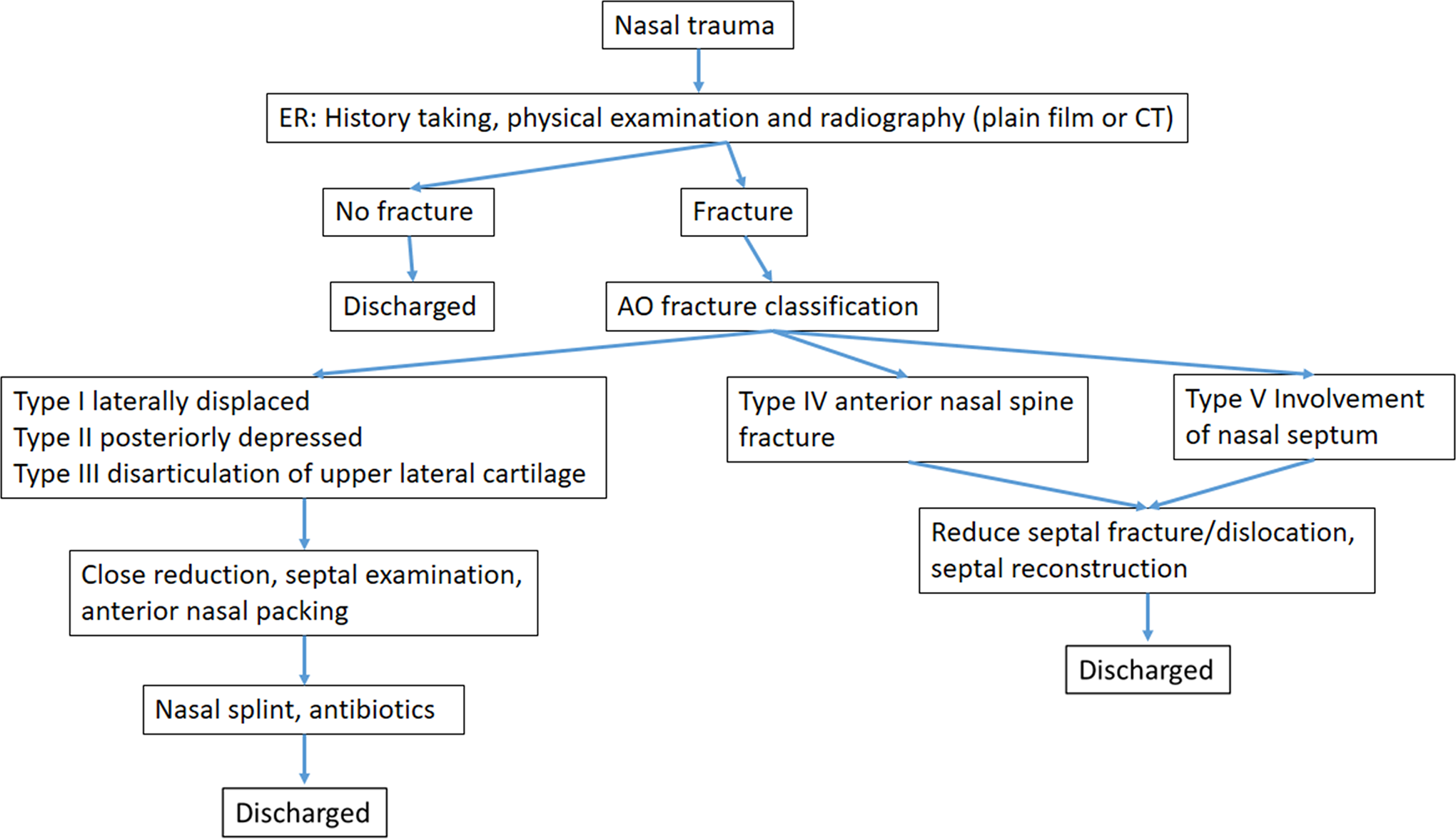
Nasal bone fracture algorithm.
Patients
We retrospectively assessed 153 patients admitted to the Ditmanson Medical Foundation Chia-Yi Christian Hospital for nasal bone fracture between January 2013 and December 2017. Nasal bone fracture was diagnosed by obtaining medical history and performing a physical examination and imaging studies, such as cephalolateral, anteroposterior radiography, or CT. Surgeons have conducted precise closed reduction (group A) on 34 patients who were diagnosed with nasal bone fractures. Another group of 119 patients with their nasal bone fractures reduced under surgeon’s experience (group B).
Surgical Procedures
All patients underwent surgical procedures under general anesthesia. In group A, all fracture positions and the distance between the fracture site and nasal tip were precisely measured on PF before surgery (Figure 3A), and precisely closed reduction was performed using either Walsham or Asch’s forceps (Figure 3B and C). In group B, closed reduction was performed using either Walsham or Asch’s forceps under surgeon’s experience. Anterior nasal packing and aluminum nasal splinting were placed after the closed reductions. As a prophylactic treatment, 1000 mg of cefazolin was administered intravenously every 6 hours until the removal of nasal packing on postoperative day 3, and the patients were then discharged from our hospital. Aluminum splinting was removed 1 to 2 weeks after surgery.
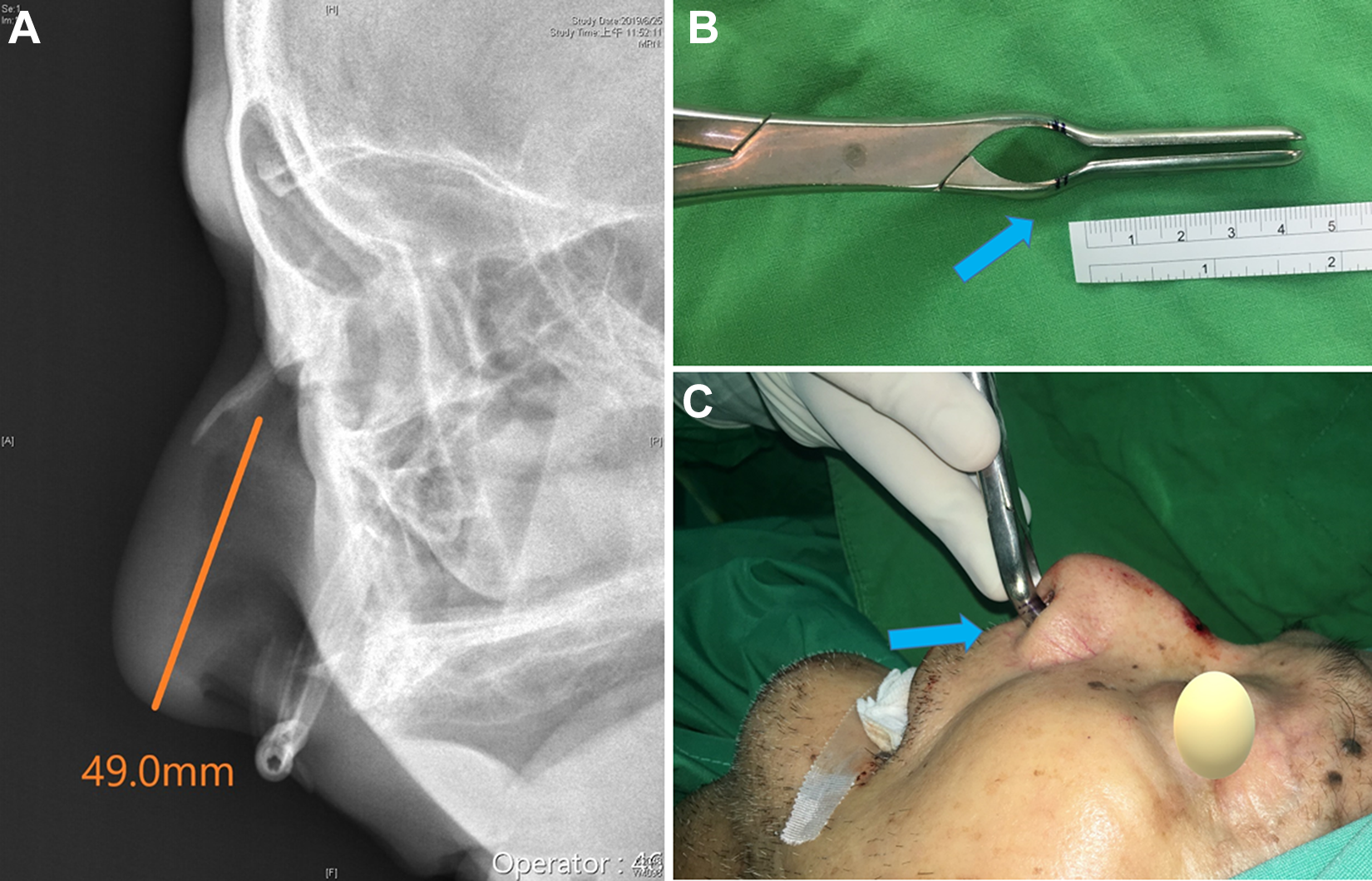
(A) The precise distance (orange color line) between fracture site and nasal tip was precise measured in plain film in picture archiving and communication system (PACS); (B) Marking of the reduction distance (blue arrow, 2 mm shorter the precise distance) in Asch forceps; (C) Close reduction of nasal bone fracture under reduction distance marking (blue arrow).
Evaluation
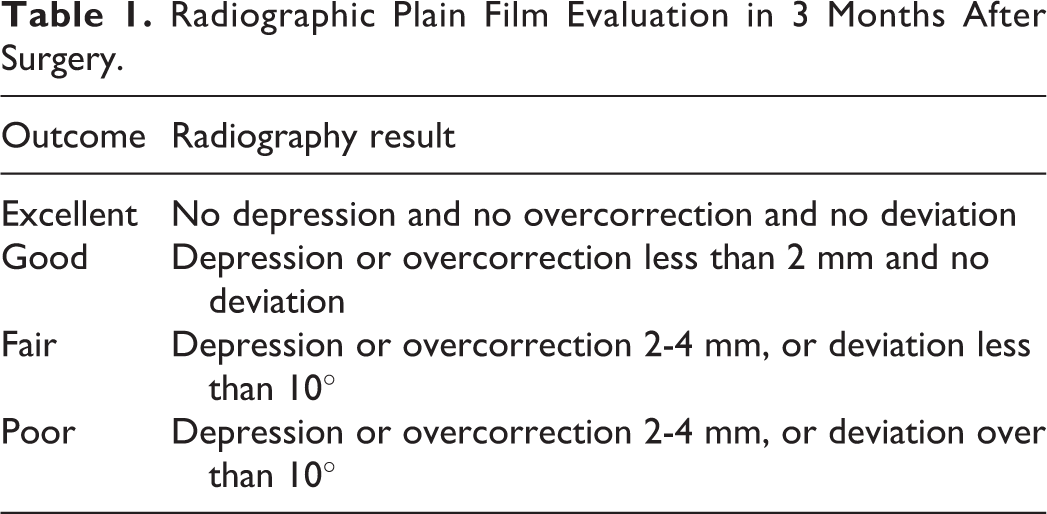
The patients came back to the outpatient clinic for follow-up 2 weeks after surgery, and after 1 and 3 months, the patients underwent evaluation with PF, with a plastic surgeon conducting assessments of the nasal septum to evaluate for functional and aesthetic outcomes. Functional outcome was defined as the presence of complications, such as swelling, nasal obstruction, infection, hematoma, and headache. Meanwhile, aesthetic outcome was defined as the presence of external deformities, such as nose deviation, depression gap, and dorsal hump. A plastic surgeon and a blinded radiologist performed PF evaluation before and 1 and 3 months after surgery, and the reduction outcomes were classified (Table 1).
Radiographic Plain Film Evaluation in 3 Months After Surgery.
Results
Basic Characteristics of the Study Population
The characteristics of the patients are shown in Table 2. No significant differences in age, gender, AO classification, and reduction outcome were observed between group A and group B (P > .05). The operative time of group A was significantly lower (12.50 ± 4.64) compared to group B (23.78 ± 11.20; P < .001).
The Patient Characteristics, Fracture Classification, Operation Time, and Reduction Outcome.a
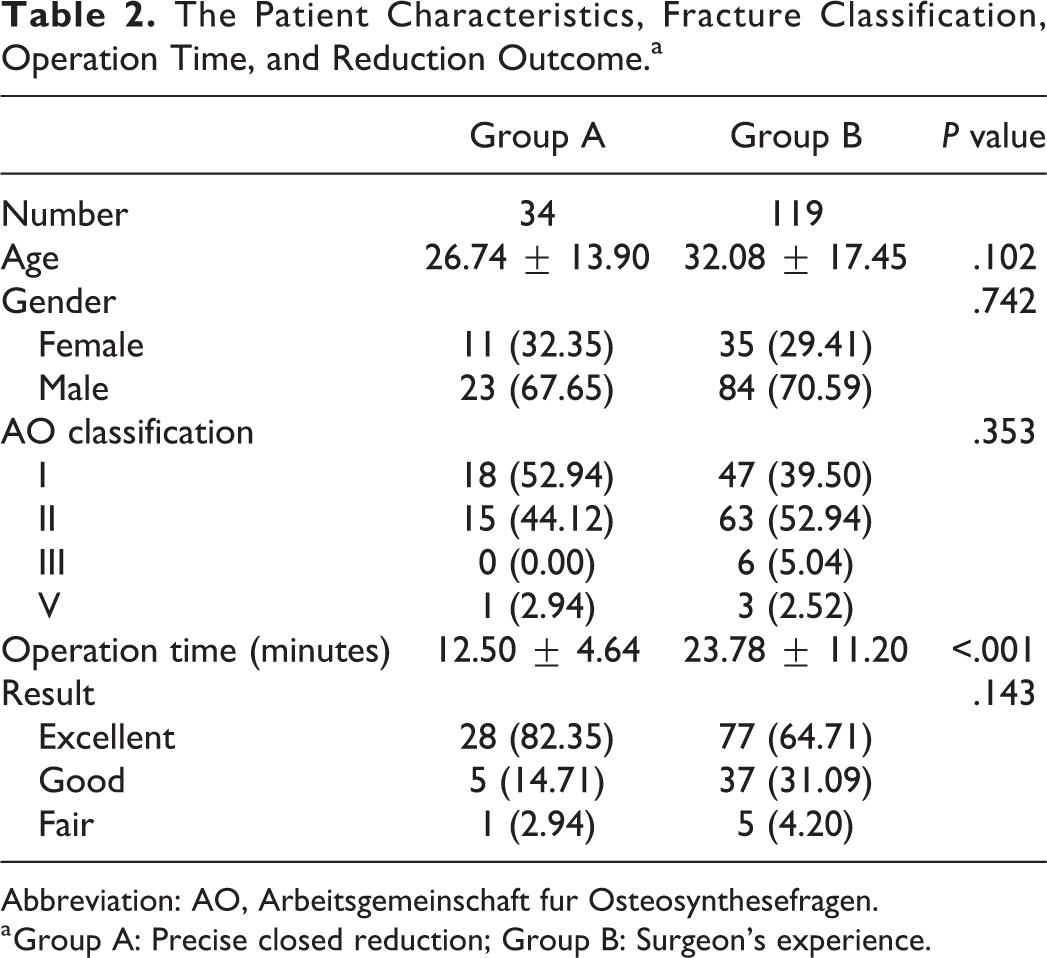
Abbreviation: AO, Arbeitsgemeinschaft fur Osteosynthesefragen.
a Group A: Precise closed reduction; Group B: Surgeon’s experience.
Observing the postoperative complications 2 weeks after surgery, 8 (28.6%) patients presented with swelling, 5 (17.9%) with nasal obstruction, and 2 (7.1%) with headache, none of the patients presented with hematoma in group A. Forty-two (35.3%) patients presented with swelling, 26 (21.8%) with nasal obstruction, 10 (8.4%) with headache, and 1 (0.8%) with hematoma in group B. One month after surgery, 2 (7.1%) patients presented with swelling and 1 (3.6%) with nasal obstruction in group A; 11 (9.2%) patients presented with swelling and 5 (4.2%) with nasal obstruction in group B. However, 3 (2.5%) patients presented with external deformity in group B. During follow-up, none of the patients presented with infection; thus, antibiotics treatment or debridement was not required. None of the patients required a secondary surgery.
Factors Associated With Operative Time Among Patients With Nasal Bone Fracture by Multiple Linear Regression Models
Multiple linear regressions were used to evaluate the influence of the characteristics, reduction method, and fracture classification on operative time. After adjusting age, gender, and AO classification, patients in group A scored 10.46 minutes less on the operative time than those in group B (P < .001). In addition, the severity of nasal bone fracture (AO classification, β = 3.37, P = .002) was positively associated with operative time. Age and gender did not have a strong linear relationship with operative time. The adjusted R 2 value indicated that 22.1% of the variance in the operative time was explained by these factors (Table 3).
Univariate and Multivariate Regression Analyses of Related Factors for Operation Time.a
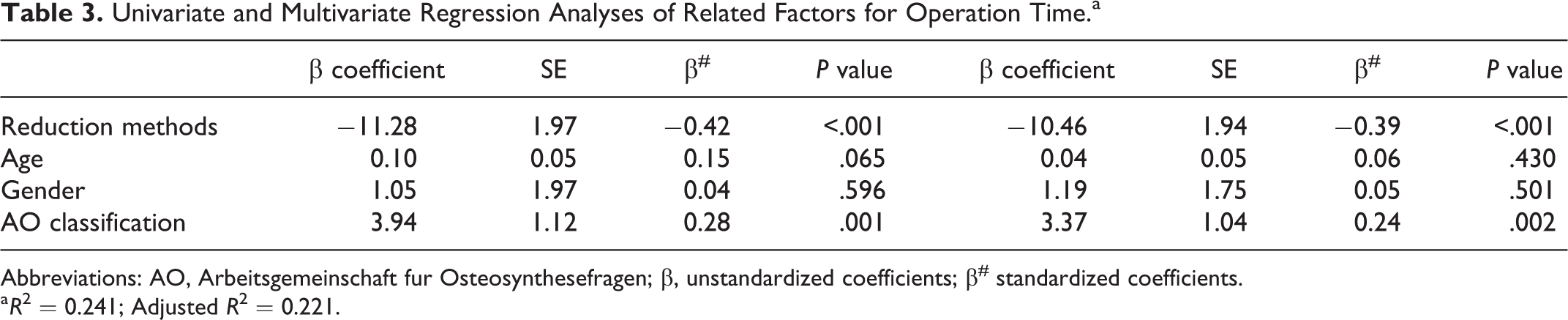
Abbreviations: AO, Arbeitsgemeinschaft fur Osteosynthesefragen; β, unstandardized coefficients; β# standardized coefficients.
a R 2 = 0.241; Adjusted R 2 = 0.221.
Discussion
Nasal bone fractures are the most common type of facial fracture owing to its location at the forefront of the face. For adults, the most frequent causes of such fracture type were fights (36.3%), traffic accidents (20.8%), sports (15.3%), and falls (13.4%). For children, the most frequent causes are sports (59.3%), fights (10.8%), traffic accidents (8.3%), collisions (5.0%), and falls (3.3%). 4 A thoroughly history taking and cautious physical examination can accurately diagnose nasal fractures.
Plain film radiography, USG, and CT can help obtain an accurate diagnosis and classification of the fractures types and can facilitate reduction procedure. The accuracy of CT scan (94.4% ± 2.3%) and USG (85.0% ± 3.6%) was significantly higher than that of PF (67.7% ± 4.7%). Computed tomography scan (89.3% ± 3.1%) and USG (87.2% ± 3.3%) were significantly more sensitive than PF. The specificity of CT scan (94.2% ± 2.3%) was significantly higher than that of USG (87.4% ± 3.3%). The specificity of USG was significantly higher than that of PF (67.8% ± 4.7%). Among the PF techniques, combining the lateral view and the Water’s view (71.8% ± 4.5%) had a significantly higher accuracy than the lateral view alone (62.4% ± 4.8%) or the Water’s view alone (61.0% ± 4.9%). In USG, no significant difference was observed in terms of accuracy among the lateral and dorsal views (95.8% ± 2.0%), lateral view alone (84.2% ± 3.7%), and dorsal view alone (84.2% ± 3.6%). 5 Although PF radiography lacks sensitivity and specificity for diagnosing nasal fractures, it can be used for a primary survey after trauma. In this regard, USG may be useful. However, it requires experience, as it is difficult to obtain information about nasal bone symmetry, its interaction with the adjacent tissues, and the nose septal pattern, which can be easily obtained on PF radiography. The use of CT scan is not always practical, due to more radiation exposure and cost-ineffective. However, it can be used for complex fractures or those combined with septum injury. Furthermore, PF is helpful when identifying the distance between the fracture site and nasal tip to help perform a precise reduction, and the distance is not able to be measured by CT or USG.
Closed reduction and splinting are generally recommended in the acute management of nasal fractures. Surgeries do not guarantee reduction, and complications, such as undercorrection, overcorrection, and deviation, may occur. The success rate in reduction is higher in simple fracture cases. 6 Most fractures of the nasal bones are initially reduced by closed reduction, and open reductions are carried out in more severe or complex cases. Verwoerd has summarized the indications of closed and open reductions, which were as follows: (1) unilateral depressed nasal pyramid fractures with a stable dorsum, (2) bilateral fractures with dislocation but without significant loss of septal height, and (3) disruption of an upper lateral cartilage from the septal aperture; and (1) bilateral fractures with significant septal injury, (2) bilateral fractures with buttress dislocation, (3) and fractures or dislocation of the cartilaginous pyramid, 7 respectively. We used the AO classification system to evaluate the types of nasal bone fracture and to provide treatments based on our protocol for nasal bone fractures. Closed reductions were conducted in individuals with AO classification type I, II, and III fractures and open reductions in those with AO classification type IV and V fractures. The complexity of operation depended on the severity of nasal bone fracture, especial in type IV and V, and more time will be needed to manage them. Rhinoseptoplasty for nasal bone fracture is only considered if the initial closed reduction had an unsatisfactory outcome.
However, as reduction is not conducted via a direct gross observation of the fracture site, it is difficult to obtain a satisfactory result. Some methods can be used to perform closed reduction, which include C-arm guide, 8 USG-assisted visual inspection, 9,10 and surgical navigation for identifying fracture locations and guiding closed reduction. 11 If closed reduction is conducted for nasal bone fractures using C-arm, an accurate result can be obtained by observing the fractured bone indirectly with continuous imaging during surgery. The surgical outcome can be immediately assessed in the operating room, thereby reducing the frequencies of complications and reoperation. 8 Experience is required when performing USG, and it is difficult to carry out reduction at the same time without any complication. Surgical navigation requires the use of more instruments and it is time-consuming and expensive. However, it is recommended for complicated nasal bone fractures or fractures that are not well reduced using the ordinary method.
Our method can easily identify the fracture site and measure the fracture distance on PF under the PACS. The reduction tip of the Asch’s forceps is shorter about 2 mm of the fracture distance, and it can easily and adequately provide support during closed reduction and causes less trauma. This method does not require new instruments, is easy to perform for closed reduction, does not require C-arm and USG or navigation experience, results in shortening the operative time, helps achieving good reductions easily, and is cost-effective. We can use C-arm or USG additionally to ensure satisfactory reduction results using our method.
In Hwang’s meta-analysis study of the complications of nasal bone fractures, the overall deformity rate is 10.4%, and no significant differences were found between closed and open reduction, between local and general anesthesia, or between those who received timely treatment and those who did not. Septal deviation occurred as a sequela of nasal bone fracture in 10.0% of patients. The nasal obstruction rate is 10.5%, and its occurrence was lower on patients who underwent open reduction than in those who underwent closed reduction. 12 In postoperative 2 weeks and 1 month complications, precise closed reduction got less nasal swelling, obstruction, and hematoma. In long-term following up, the nasal deformity rate was 0 in precise closed reduction but 3 (2.5%) patients in surgeon’s experience group. In radiography, precise closed reduction has better result (82%) (excellent) than surgeon’s experience group (65%). No deviation was observed in the clinical and radiologic analysis in precise closed reduction due to less trauma during reduction and precise position of the Asch’s forceps tip to achieve accuracy in reduction.
Post-reduction care included intranasal packing and external nasal splinting, or Kirschner wire (K-wire) splinting. Complaints of nasal obstruction, dry mouth, loss of appetite, and sleep disturbance were significantly lower in the K-wire group. However, aesthetics/postoperative asymmetry did not differ significantly between the groups. No significant difference was observed in terms of the accuracy of reduction and support provided to the reduced nasal bones between the groups. 13 K-wire splinting required longer operative time and more skilled techniques, and there is a higher occurrence of tissue trauma and the risk of complication, such as perforation of the frontal sinus or the cribriform plate of the ethmoid bone, associated with such procedure. Thus, intranasal packing and external nasal splinting were applied for post-reduction care in our series. The packing had several disadvantages, which include blocking the nasal airway and the risk of infection and headache. The optimal duration of the packing from 1 day to 1 week after closed reduction has been a controversial issue. 14 Based on the study of Choi et al, no statistically significant difference was observed between nasal packing in 1, 3, and 5 days of heights, deviations, and nasal bone contours but less discomfort in the 1-day group. 15 We used Merocel nasal packing with airway to decrease nasal blocking discomfort and to support the fractured nasal bone in post-reduction swelling for 3 days.
Conclusion
Precise closed reduction assisted with PF under the PACS has significant clinical efficacy for the treatment of nasal bone fractures. Closed reduction was conducted accurately by directly measuring the distance between the fractured site and nasal tip, thereby effectively reducing the frequencies of complications, such as nasal swelling, deviation, deformity, and reoperation. Our method does not require the use of new instruments and C-arm, USG, or navigation experience and can be easily used in reduction procedure. Moreover, it has a shorter operating time, easier to perform, achieving greater reductions, less radiation exposures, and is cost-effective. In addition, this method can be combined with C-arm, USG, or navigation in the management of complex nasal fractures or evaluation of reduction results. Therefore, for the treatment of nasal bone fractures, more accurate and satisfactory outcomes will likely be obtained with precise closed reduction with PF measurement under the PACS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.