
Abstract
Objectives:
The nasal septal swell body (NSB), also known as the nasal septal turbinate, is located in the anterior part of the nasal septum. This study is a narrative review of the existing knowledge on recent developments in NSB.
Methods:
A literature search was performed using PubMed, Embase, Web of Science, Ovid, and Cochrane Library databases. Google Scholar was used to access more extensive literature. The inclusion criteria were human studies published in English. The exclusion criteria were non-English language and animal studies.
Results:
Of the 345 articles that were initially obtained from 5 databases and Google Scholar, 28 were included in this review. There have been many names for NSBs in the past, which still have no unified terminology recognized by professionals. Pathological investigations revealed that NSB contains a certain amount of sinusoidal blood components. Nasal septal swell body is closely related to the internal nasal valve. Imaging studies have found that the size of NSB is associated with nasal diseases, and NSB hypertrophy can cause anatomic obstruction. In recent years, several procedures for NSB have been reported, and preliminary effectiveness has been achieved. However, the long-term outcomes of volume reduction techniques remain unproven.
Conclusions:
The NSB is a distinct anatomic structure that may contribute to nasal obstruction and may be reduced surgically with unclear long-term results. Although being investigated for over a century, the unique physiological roles of NSB are not yet fully understood. More evidence is needed to elucidate its physiological effects.
Keywords
Introduction
The nasal septal swell body (NSB) is a distinct structure located in the anterior part of the nasal septum (NS), adjacent to the anterior part of the middle turbinate and superior part of the inferior turbinate (IT; Figure 1). 1,2 Structurally, NSB contains bone and cartilage components of the NS and swell tissues involving bones and cartilages. 3 Kölliker and Kohlraush first reported the “swell bodies” in the nasal cavities of humans. 4 Schieferdecker called this structure on the NS a “tuberculum septi.” 4 Previous studies have suggested that NSB is a part of the nasal cavity and plays an essential role in regulating various physiological functions. 5,6 The NSB has been a surgical target of interest and hence surgical procedures have also been attempted to reduce its volume in recent years. 7 -10
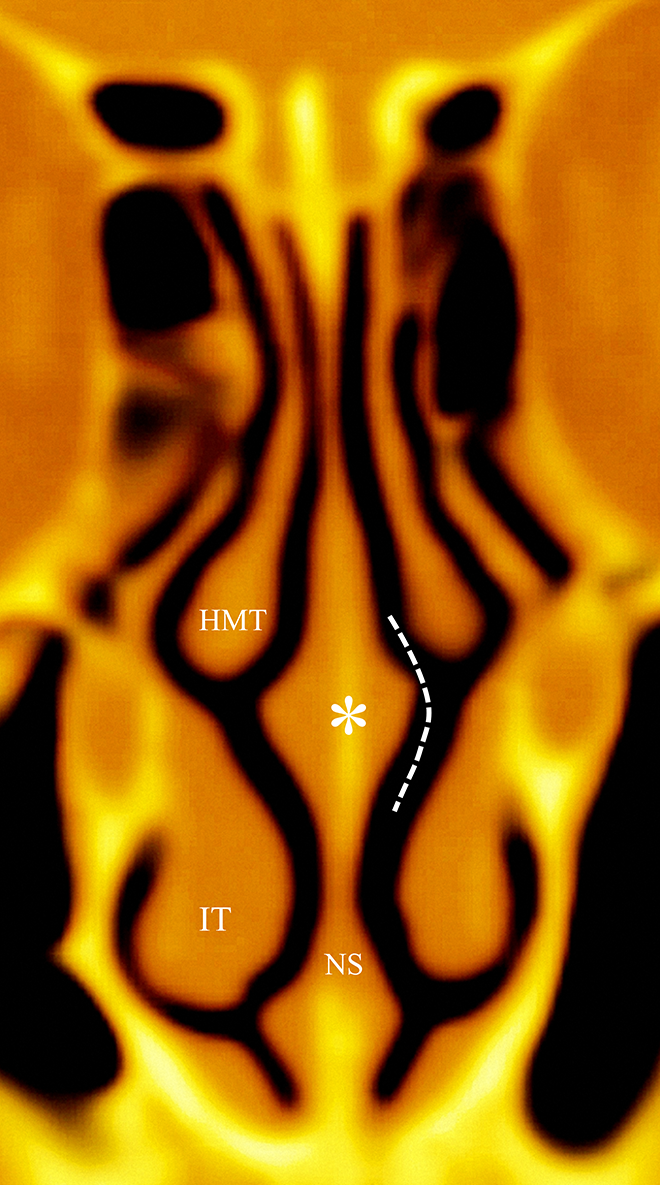
Schematic illustration of the relationship between NSB and the adjacent structures. The white asterisk depicts NSB. The white dashed line shows the internal nasal valve. HMT indicates head of middle turbinate; IT, inferior turbinate; NS, nasal septum; NSB, nasal septal swell body.
Nevertheless, the structure and function of NSBs are still far less understood. 11,12 Therefore, we endeavored to produce a precise contemporary description to improve our understanding of NSB. This narrative review highlights recent developments related to NSB, including terminology, examination, histology, physiological effects, imaging, operations, and future directions.
Methods
Research Strategy
This review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A literature search was carried out using the PubMed, Embase, Web of Science, Ovid, and Cochrane Library electronic databases. Google Scholar, a search engine, was also used to access more comprehensive literature. The following keywords were used: “nasal septal swell body,” “nasal septal turbinate,” “septal turbinate,” “Kiesselbach’s body,” “septal swell body,” “nasal septal body,” “septal body,” “nasal swell body,” “swell body,” “septal erectile body,” “septal cavernous body,” “anterior septum tuberculum,” and “intumenscentia septi nasi anterior.” The searches were performed independently by 2 authors. The final search was performed on February 20, 2021.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: human studies, type of study (original papers, conference papers, case reports, reviews, and clinical trials), and language (English written studies). No constraints on the year of publication were applied.
We initially screened the titles and abstracts of the retrieved documents for potential relevance. We excluded studies that were not relevant to our study topic. Animal studies, non-English language articles, and abstracts without full text were also excluded. Subsequently, full texts of all relevant articles were obtained and assessed to exclude those that did not meet the inclusion criteria.
Results
The initial database search identified 337 articles: 56 in PubMed, 41 in Embase, 30 in Web of Science, 33 in Ovid, and 177 in Cochrane Library. In addition, 8 articles were obtained through the Google Scholar search engine. Thus, a total of 345 articles were obtained. After removing duplicates, a total of 238 pieces of literature remained. Screening of titles and abstracts excluded 206 studies, and 32 studies were potentially eligible for evaluation. After reading the full text in these studies, another 4 articles were eliminated (nasal vestibular body studies = 2, abstracts without full texts = 1, and animal study = 1), leaving 28 articles for this review. A flowchart of the literature search is presented in Figure 2.
Flowchart showing the process of literature screening.
Terminology
Nasal septal swell body has been described in the literature in various medical languages. These terminologies include nasal septal turbinate, 8,9,13,14 septal turbinate, 3,15 Kiesselbach’s body, 16 septal swell body, 1,12,17 -19 nasal septal body, 11,12,20 septal body, 2,16,21 -24 nasal swell body, 10,25 -28 NSB, 3,7,29 swell body, 30 septal erectile body, 31,32 septal cavernous body, 26 anterior septum tuberculum, 33 and intumenscentia septi nasi anterior. 15,34 These names can now be classified roughly into 2 broad categories: septal turbinate categories and septal body categories. Proponents of the former name argued that the distinct structure is similar to that of lateral turbinates, while those of the latter considered it differently. To date, no universally recognized terminology exists. This situation has led to barriers in scholarly communication. European position paper on anatomical terminology of the internal nose and paranasal sinuses suggested that the English terminology of the structure is “septal tubercle.” 35 However, the term “tubercle” seems inappropriate to describe a particular physiological structure, since it also refers to pathological lesion of the tissues. This leads to a misunderstanding of the structure. Wexler et al suggested that “nasal septal swell body” is a suitable term for expansile tissues based on coronal computed tomography (CT) scans, and it implies no constitutional or physiological information. 3 Hence, we agree with this term. Given the limitations of current recognition, the naming principles should be considered neutral according to the regulations of anatomical locations and morphological structure.
Correlation With Internal Nasal Valve
The nasal valve, the narrowest portion of the nasal airway, is subdivided into external nasal valve and internal nasal valve (INV). 36 Historically, INV was noted as distal as 1.3 cm from the nares and bounded by the upper lateral cartilages, septum, IT, and nasal floor. 37,38 However, recent evidence suggests that it is a complicated 3-dimensional (3D) structure, comprising various morphological characteristics rather than a simple planar structure. 30 However, the detailed 3D features of INV have rarely been described. 39
The relationship between NSB and INV has sparked controversy. There are 2 main viewpoints on this issue. Some experts proposed that NSB is located adjacent to the distal part of INV, and NSB hypertrophy can encroach INV, resulting in anatomic obstruction. 1,9 However, others have argued that NSB is a part of the medially bound INV. 12 Cole considered NSB as one of the vulnerable pathological obstruction sites. 31 The degree of congestion of the erectile mucosa of NSB controls the cross-sectional area’s size and resistance to airflow. There is a mutual understanding of the 2 perspectives in that NSB is closely linked to INV.
Nasal Examination
Under typical conditions, NSB can be readily visualized using anterior rhinoscopy or rigid endoscopy (Figure 3). If the patient has nasal diseases such as IT hypertrophy, it is necessary to use nasal decongestants before nasal examination. The expansile structure is also easily ignored by otolaryngologists. Nasal septal swell body may be misdiagnosed clinically as a high septal deviation (SD), as pointed out in the previous literature. 3,16,25,34 Topical application of decongestants in the nasal cavity is a useful method to diagnose NSB. It can also be differentially diagnosed based on CT imaging findings.
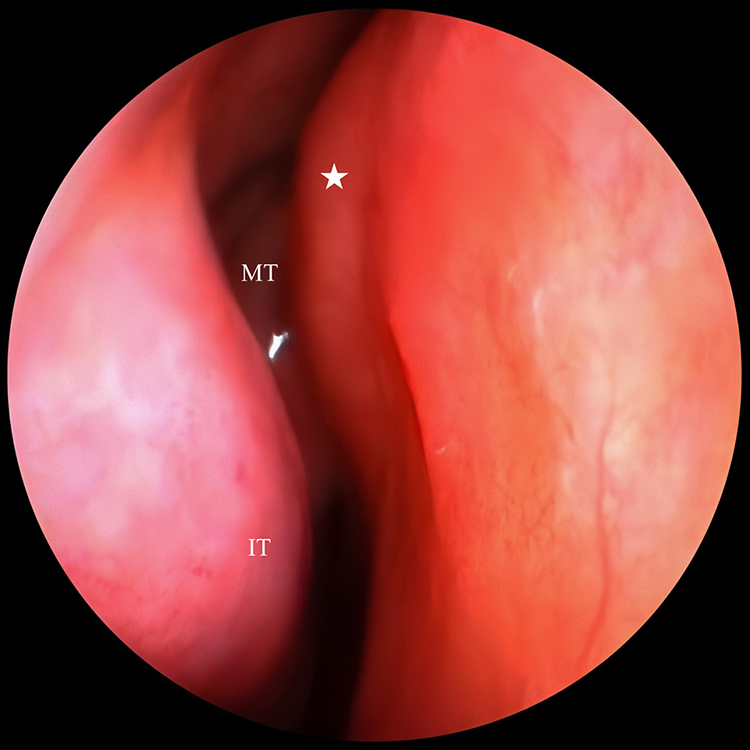
A 0° rigid endoscopic view showing the nasal septal swell body (right nasal cavity), depicted by a white asterisk. MT indicates middle turbinate; IT, inferior turbinate.
To date, there have been no uniform criteria regarding the size of an NSB in healthy individuals and definition of NSB hypertrophy. Recently, Yu et al proposed a definition of NSB hypertrophy based on nasal endoscopic examination: bilateral symmetrical bulging, not ultimately seeing the middle turbinate from limen nasi, and a gap of < 3 mm between the NSB and the lateral nasal wall. 22 However, these criteria have not been verified in a large sample population. Therefore, this definition needs to be validated in multicenter studies. In addition, the influence of the bony septum and septal cartilage should be considered while setting standards.
Morphologic and Histological Characteristics
Two previous studies directly measured the size of NSB. 16,29 Elwany et al described the structure as ellipsoidal, with a mean horizontal diameter of 2.0 ± 0.15 cm and a mean vertical diameter of 1.5 ± 0.11 cm. 16 Costa et al described it as having a fusiform shape, with a mean length of 2.84 ± 0.35 cm, width of 1.24 ± 0.19 cm, and height of 1.96 ± 0.32 cm. 29
Nasal septal swell body is covered by a thick, pseudostratified, ciliated epithelium with goblet cells. 16 Although examining samples harvested from cadavers, Saunders et al found that NSB is a highly glandular tissue. 33 Wexler et al examined mucosal biopsies of NSB and found that it mainly consisted of seromucinous glands (49.9%), with moderate venous sinusoids (10.0%). 3 Elwany et al reported a conclusion slightly different from the study mentioned earlier, with glandular acini (69.5%) and dilated blood sinusoids (21.2%). 16 These rich glandular tissues seem well adapted to the drying effects caused by a high airstream impact. 3 The existence of a certain number of blood sinusoids confirms that NSB is part of the expansile vascular tissues in the nasal cavity. 3,16 A study by Yigit et al evaluated the histopathology of NSB in patients with allergic rhinitis and those with nonallergic rhinitis and found no significant difference between them. 28
Physiological Effects
The above-mentioned histopathological features suggest that NSB is a unique structure that can play a vital role in regulating nasal airflow and adjusting the temperature and humidity of the inhaled air stream. 3,16 Nasal septal swell body changes the nasal airflow direction, splitting the inhaled airflow into 2 directions: 1 toward the nasal meatus and the other toward the ostiomeatal complex, which increases the contact area of the nasal mucosa and thus better serves as a warming and humidifying structure. 14 Common respiratory viruses can replicate rapidly in a cooler upper airway environment of 32 °C, but the replication is restricted at a body temperature of 37 °C. 40 When infected with respiratory viruses, the human body can limit the replication of respiratory viruses by regulating the nasal cycle to increase the nasal mucosal temperature to 37 °C through nasal congestion and nasal obstruction. 40 Nasal septal swell body is similar to IT and participates in the nasal cycle. Therefore, we speculate that NSB also has a protective effect against respiratory viral infections.
Imaging Findings
Although NSB is sometimes not noticeable during nasal examination, it can be well visualized by imaging techniques (Figure 4). Scholars have studied these nasal structures using imaging methods for nearly 4 decades. 5,6 However, early research is only preliminary. In 1983, Cole et al conducted a CT study on the distribution of erectile mucosa in healthy adult nasal cavities. 5 This study showed that the anterior septal region, such as the middle turbinate and IT, also consists the erectile mucosa. Later, Ng et al obtained a similar conclusion in a magnetic resonance imaging investigation. 6
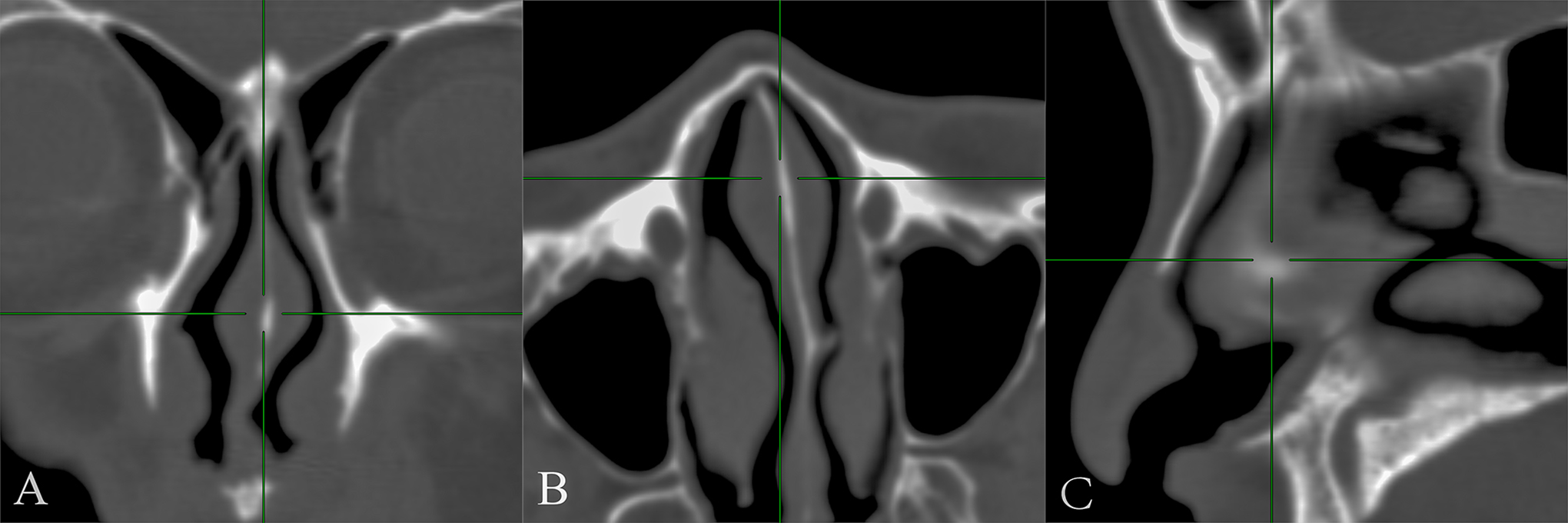
Computed tomography (CT) scan of the paranasal sinus showing the nasal septal swell body, depicted by green crossed lines. A, coronal CT scan, (B) axial CT scan, and (C) sagittal CT scan.
It is still debatable whether the structure is an anatomical variation or a universal existence. Arslan et al investigated the paranasal sinus CT scans of 595 patients and found that the structure existed in 332 patients (55.79%); hence, they considered it to be a typical anatomical variation in the nasal cavity. 34 A recent study showed that the structure was detected in 25.1% of individuals (149/594). 27 Moreover, the structure may also present with pneumatization, similar to concha bullosa. 15 The results of Setlur and Goyal’s survey differed from those mentioned above in that the structure was detected in all 100 individuals, 21 indicating that the structure is a common feature in healthy individuals.
Recently, Wong et al studied the correlation between the sizes of NSB and IT. 17 This study revealed a statistically significant correlation between the change in the width of NSB and the total width of IT, while the height of NSB did not show a statistically significant association with that of IT. 17
Several researchers have investigated both age and gender differences related to the size of the structure. 20,34 Arslan et al identified that NSB was more common in males and young individuals. 34 San et al found that the areas of NSB were smaller in females than in males, in either the right or left nasal cavity. 20
Correlation With Nasal Diseases
Previous studies have revealed a higher association between NSB and nasal diseases. 2,11,21,23 Setlur and Goyal measured the relationship between NSB size and laterality of SD. 21 Their research showed that the NSB size of the contralateral SD was more significant than that of the ipsilateral SD. Another survey by Demirci et al reached a similar conclusion. 23 The study also indicated that there was a negative correlation between the sizes of NSB and the middle and ITs in patients with SD. 23 Aki et al investigated the correlation between NSB and quality of life using the Sino-Nasal Outcome Test questionnaire. 24 The study found that SD and ipsilateral NSB size were significantly associated with a diminished quality of life. 24 Yu et al found that NSB hypertrophy is likely to be related to IT hypertrophy and hence clinicians should scrutinize NSB in patients with IT hypertrophy. 2 Moreover, allergic rhinitis can enhance the positive effect. 11
Surgical Attempts
In the past 2 decades, many scholars have proposed surgical interventions for NSB and tried it using various operating techniques. In 2000, Cole first introduced the concept of surgical reduction of erectile tissues and presumed that surgical intervention might improve the results of septoplasty. 32 Cole mentioned this idea again in a study 3 years later. 31 In 2010, Costa investigated the radiological and anatomical features of NSB and raised a question whether the tissues should be surgically treated in symptomatic patients. 29 However, no new procedures have been described in the literature for NSB for over a decade. Recent years have seen a rebirth of interest in operating the peculiar structure, and various therapeutic approaches have been presented. 7,22 Yu et al introduced a microdebrider-assisted procedure for NSB hypertrophy. 22 A prospective randomized controlled study revealed that a combination of volume reduction of NSB and turbinoplasty is superior to turbinoplasty alone for patients with IT and NSB hypertrophy. However, this study has certain limitations; it included only 26 patients, and the follow-up period was too short. Kim et al performed a coblation technique for patients with abnormally thickened NSB. 7 The retrospective clinical series consisted of 8 patients, 6 of whom were delighted with the treatment effect after 1 year of follow-up. The preliminary study showed that coblation is an effective treatment option for NSB hypertrophy. 7 Catalano et al treated 60 patients with prominent NSB by radiofrequency ablation and performed nose obstruction symptom evaluation score and NSB size score on the patients at 3 and 6 months after surgery. 18 Although these patients achieved satisfactory results and improved nasal congestion symptoms, 1 patient developed a complication of septal perforation (SP), which deserves attention. 18 A recent retrospective study found that repairing SPs with bilateral mucosal flaps may cause persistent postoperative nasal congestion due to NSB and that nasal congestion in these patients may be relieved by the surgical reduction of NSB without reperforation. 10
Application of isolated topical decongestants in NSB can determine whether surgery is needed and help predict nasal patency after surgery. 41 A silastic sheet was cut into the shape and size of the anterior nasal cavity. A rectangular cotton sheet impregnated with decongestant was attached on one side, with the cotton sheet facing the NSB so that the decongestant did not involve the IT. 41 When performing NSB reduction in conjunction with other rhinological procedures, NSB reduction should come first. 19 Topical nasal decongestants or local anesthetic injections should be avoided during NSB procedures in order to present the native NSB prominence, which helps to identify the surgical target accurately. 19
It is still unclear whether surgical intervention of NSB can improve the long-term therapeutic effect of nasal obstruction. In addition, minimally invasive surgery techniques are recommended to avoid injuring the critical surrounding structures and causing postoperative complications such as SP. 20 To minimize SP risk, we suggest that NSB operation should not be performed simultaneously with septoplasty. Patients who have already undergone septoplasty should wait at least 3 months before undergoing NSB. 18 Performing surgery on both sides of the NSB can also increase the risk of SP.
Recently, Moss et al pointed out that NSB is an overlooked surgical target based on preliminary evidence. 9 Nevertheless, some scholars hold different opinions on the surgical intervention of NSB, arguing that the operation in this particular region may lead to postoperative nasal dryness and nasal infections. 14
Future Directions
Nasal septal swell body is a structure that remains to be recognized, and further investigations are needed to unveil its physiological effects. First, NSB is a 3D structure, not a bidimensional one. 30 Previous studies measured the data of various planes and attempted to present its 3D feature. 16,29 Nasal septal swell body includes a part of the bone and cartilage of the NS rather than an expansile soft tissue alone. However, present studies do not involve them. Thus, with 3D reconstruction, the NSB could be measured precisely. Second, NSB is a dynamic structure that may change its size and shape with the nasal cycle. 24 However, this hypothesis needs to be confirmed by in vivo or imaging assessments. Third, no study has been conducted to measure the size of NSB before and after decongestion. 21 Such a research design is worth considering. Fourth, computational fluid dynamics, a scientific tool, has been widely used in the assessment of nasal diseases. 26,42 Similarly, modern technology can also be used for NSBs to accurately assess temperature changes, pressure, and wall shear stress. Finally, multicenter study designs, including different races, are needed to determine the treatment effect based on scientific evidence.
Limitations
This review has some limitations. First, it summarizes articles published in English during the past few decades and does not cover the relevant studies published in languages other than English. It also does not include age-old literature. Second, despite the best efforts, there are still omissions in the essence of the predecessors’ thoughts. As a result, there may be some bias in the understanding of this unique structure.
Conclusion
The nasal septal swell body was first discovered over a century ago and has since been explored by multigenerational researchers. Researchers tend to have different interests at different times. In recent decades, research has tended to focus on imaging investigations and surgical exploration. Currently, there is much interest in the surgical reduction of NSB. However, a clear understanding of this particular structure is far from complete. Further evidence is needed to clarify its physiological effects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.