
Abstract
Objective:
To investigate the anatomical status of the round window niche and hearing outcome of cochlear implantation (CI) after explorative tympanotomy (ExT) with sealing of the round window membrane in patients with sudden sensorineural hearing loss at a tertiary referral medical center.
Methods:
Between January 1, 2007, and July 30, 2020, 1602 patients underwent CI at our department. Out of these, all patients previously treated by ExT with sealing of the round window membrane because of unilateral sudden hearing loss were included in the study. A retrospective chart review was conducted concerning method of round window membrane sealing, intraoperative findings during CI, postoperative imaging, and hearing results.
Results:
Twenty one patients (9 females; 8 right ears; 54.3 years [± 12.9 years]) underwent ExT with sealing of the round window membrane with subsequent CI after 26.6 months (± 32.9 mo) on average. During CI, in 76% of cases (n = 16), the round window niche was blocked by connective tissue due to the previous intervention but could be removed completely in all cases. The connective tissue itself and its removal had no detrimental effects on the round window membrane. Postoperative computed tomography scan showed no electrode dislocation. Mean postoperative word recognition score after 3 months was 57.4% (± 17.2%) and improved significantly to 73.1% (± 16.4%, P = .005) after 2 years.
Conclusion:
Performing CI after preceding ExT, connective tissue has to be expected blocking the round window niche. Remaining tissue can be removed safely and does not alter the round window membrane allowing for a proper electrode insertion. Short- and long-term hearing results are satisfactory. Consequently, ExT with sealing of the round window membrane in patients with sudden sensorineural hearing loss does not impede subsequent CI that can still be performed safely.
Keywords
Introduction
In patients with severe sudden sensorineural hearing loss (SSNHL), explorative tympanotomy (ExT) with the sealing of the round window membrane may be offered to patients after failure of conservative treatment. Intraoperatively, the round window niche and oval window niche are inspected for a perilymph fistula that has been reported to occur in up to 35% of the cases. 1 Sealing of the round window membrane has been described with temporal connective tissue or a fat filling in combination with fibrin glue or topical cortisone.1-4 Even in view of the potentially high rate of spontaneous recovery of SSNHL, patients with severe initial hearing loss have a poor prognosis. Despite the treatment with ExT, around one-third of patients show no hearing improvement over time.5,6 In patients with residual moderate-to-severe hearing impairment and poor speech perception, cochlear implantation (CI) is an effective treatment option when hearing rehabilitation with a conventional hearing aid remains unsatisfactory. 7 In this regard, successful CI after ExT has been described in a case report by Kleinjung et al. 8 Nevertheless, no knowledge exists about if and how previous sealing of the round window influences subsequent CI. Thus, the primary objective of the present study is to determine the accessibility of the round window membrane for electrode insertion during CI in patients previously treated with ExT. Secondary objectives include postoperative electrode position and hearing results.
Patients and Methods
This retrospective study was conducted at a tertiary referral medical center (Department of Otorhinolaryngology and Head and Neck Surgery, Friedrich-Alexander-Universität Erlangen-Nürnberg [FAU], Erlangen, Germany) and was approved by the local ethics committee (application number: 424_20 Bc).
Patients provided with a cochlear implant between January 01, 2007, and July 30, 2020, were eligible for the study. Inclusion criteria were as follows: history of sudden hearing loss treated with ExT, subsequent CI of the same ear. Exclusion criteria were age under 18 years at the time of ExT, incomplete medical records. Prior to any surgical intervention, pure tone audiometry allowed the calculation of the mean four-frequency pure-tone average (4FPTA), that is, 0.5, 1, 2, and 4 kHz.
The indication for ExT was unilateral acute severe to profound hearing loss, that is, hearing loss ≥ 60 dB over at least 4 audiometric frequencies and missing response to conservative treatment. In general, 250 mg intravenous prednisolone for 3 following days once daily and at least one dose of intratympanic dexamethasone (4 mg) was applied before recommending ExT after 3 days of treatment without hearing improvement. In brief, the surgical procedure was performed in local or general anesthesia, depending on the patient’s preference. Following the endaural auxiliary incision, a tympanomeatal flap was raised and the tympanic membrane was released from its frame. The round window niche and the oval window niche were inspected and controlled microscopically for perilymph fistula. Pressure transmission from the oval to the round window was controlled by careful movement of the stapes. According to Maier et al, patients were classified into 3 groups retrospectively: perilymph fistula, absence of perilymph fistula, and doubtful fistula. 1 In general, connective tissue was harvested from the area of the endaural incision. Based on the surgeon’s discretion, it was soaked with cortisone for about 30 seconds (1 ml of triamcinolone 40 mg/ml or 1 ml of dexamethasone 4 mg/ml) and applied at the round window niche. Thereafter, the tympanic membrane and the tympanomeatal flap were laid back and the auditory canal was filled with GELITA-SPON® STANDARD (Gelita Medical) that was removed 1 week later. At the end of the procedure, a soft ointment patch and a pressure bandage were applied at the auricle. The first follow-up examination for audiometric testing was scheduled 2 weeks after surgery. Three months after ExT, the patient was counseled about options of hearing rehabilitation depending on the current audiometric results. In general, a contralateral routing of signals (CROS) or bilateral microphones with contralateral routing of signals (BiCROS) hearing aid was tested. If indicated, CI was recommended to the patient according to the applicable guidelines. 9 During CI surgery, the middle ear was entered via a posterior tympanotomy and the round window niche was checked for connective tissue and scar tissue remaining from the previous sealing during ExT. Tissue impeding access to the round window was carefully removed with a small hook. If necessary, the subiculum was drilled for better visualization of the round window. Electrode application was performed via the unaltered round window, an enlarged round window or a cochleostomy. In general, the round window approach was primarily targeted. If the round window anatomy was not favorable, an enlarged round window approach was performed. For that, the round window was carefully extended anterior-inferiorly by approximately 1 to 2 mm with a 1 mm diamond burr to reveal the membranous scala tympani that was opened with a 0.5 mm needle following slow and careful atraumatic electrode insertion. Finally, when individual anatomy required, a cochleostomy was performed anterior-inferior to the round window. The type of approach was based on the surgeon’s discretion. The position of the implanted electrode was confirmed by Dyna-CT-scan (Siemens AXIOM Artis, Siemens Healthineers AG) with a slice thickness of maximum 1 mm and a resolution of 512 × 512 ppi on the first postoperative day.
For word recognition score (WRS), the Freiburg monosyllable test was used. Before CI, the maximum recognition score for phonemically balanced monosyllabic words (WRSmax) was measured using headphones. 10 Postoperative WRS with cochlear implant was measured in free field with a presentation level of 65 dB sound pressure level in an anechoic booth. Appropriate masking of the contralateral ear was assured. WRS was measured 3 months (WRS3m), 6 months (WRS6m), 1 year (WRS1y), and 2 years (WRS2y) after CI. Statistical analyses were performed using SPSS (IBM SPSS Statistics version 22.0; IBM). Metric variables are presented as values ± standard deviation and range (minimum [min], maximum [max]). Wilcoxon signed-rank test was used to evaluate hearing improvement after ExT and after CI. A repeated measures analysis of variance (ANOVA) with the main effect “time” (WRSmax, WRS3m, WRS6m, WRS1y, and WRS2y) was calculated to compare word recognition scores over time. In case of a significant main effect, follow-up tests were performed with dependent t tests (WRSmax vs WRS3m; WRS3m vs WRS2y; and WRS3m vs WRS6m vs WRS1y vs WRS2y). Correction for multiple testing was performed using family-wise error correction resulting in a critical P value of .01 for the WRS.
For each significant post hoc test, the effect size r was calculated, with r = 0.1 displaying a small effect, r = 0.3 representing a medium, and r = 0.5 representing a strong effect.
Results
Explorative Tympanotomy With Sealing of the Round Window Membrane
Out of 1602 CIs at our department between January 01, 2007, and July 30, 2020, a total of 21 patients accounting for 21 ears underwent ExT prior to CI. The included 21 patients (9 females, 8 right ears) averaged 54.3 years (± 12.9 years, min 22.8 years, max 71.7 years) at the time of ExT. Severe sudden sensorineural hearing loss had been diagnosed in all but 1 of the 21 cases. One patient suffered from acute severe combined hearing loss due to traumatic inner ear damage and a perforation of the tympanic membrane with a cotton stick. ExT had been performed at our institution in 17 (81%) of 21 patients and in 4 cases at a different institution. The procedure was performed by 13 different surgeons in general (n = 14) and local anesthesia (n = 7). Mean operating time was 40.2 minutes (±16.7 minutes, min, 16 minutes, max, 70 minutes). Intraoperatively, a doubtful perilymph fistula in the region of the round window was reported in 3 cases (14%), whereas the round window showed no sign of a perilymph fistula in 18 cases (86%). The oval window was unsuspicious in all patients. Connective tissue was used for sealing of the round window membrane in all but 1 patient. The connective tissue was soaked in cortisone in 10 cases and fixated using fibrin glue in 2 cases. One round window was sealed with GELITA-SPON® STANDARD (Gelita Medical) and cortisone only.
Cochlear Implantation
At the time of CI, 3 patients had been implanted at the contralateral ear before. After testing, no patient opted for treatment with CROS or BiCROS hearing aid. Mean time from ExT to CI was 26.6 months (± 32.9 mo, min, 2.8 mo, max, 115 mo) with a median of 11.2 months. Patients averaged 56.5 years (± 12.4 years, min, 30.6 years, max, 74.2 years) at the time of CI. All but 2 CIs were performed by a single experienced surgeon. Mean operation time was 72 minutes (±14.4 minutes, min, 47 minutes, max, 99 minutes). Implants from Cochlear® (Cochlear Limited) with Contour Advance electrodes were used in 13 patients (CI24RE [CA] = 2; CI512 = 10; CI612 = 1), whereas Slim Modiolar electrodes were implanted in 3 additional patients (CI532 = 2; CI632 = 1). Five patients received implants from MED-EL® (MED-EL) using lateral wall electrodes (Concerto Flex 28 = 1; Synchrony Flex 28 = 4).
Intraoperatively, connective tissue was found covering the round window in 16 out of 21 patients (76%). In all 16 cases, connective tissue could be removed completely with a small hook. The round window membrane itself did not appear to be altered in any case. Figure 1 shows intraoperative findings before and after tissue removal at the round window niche.
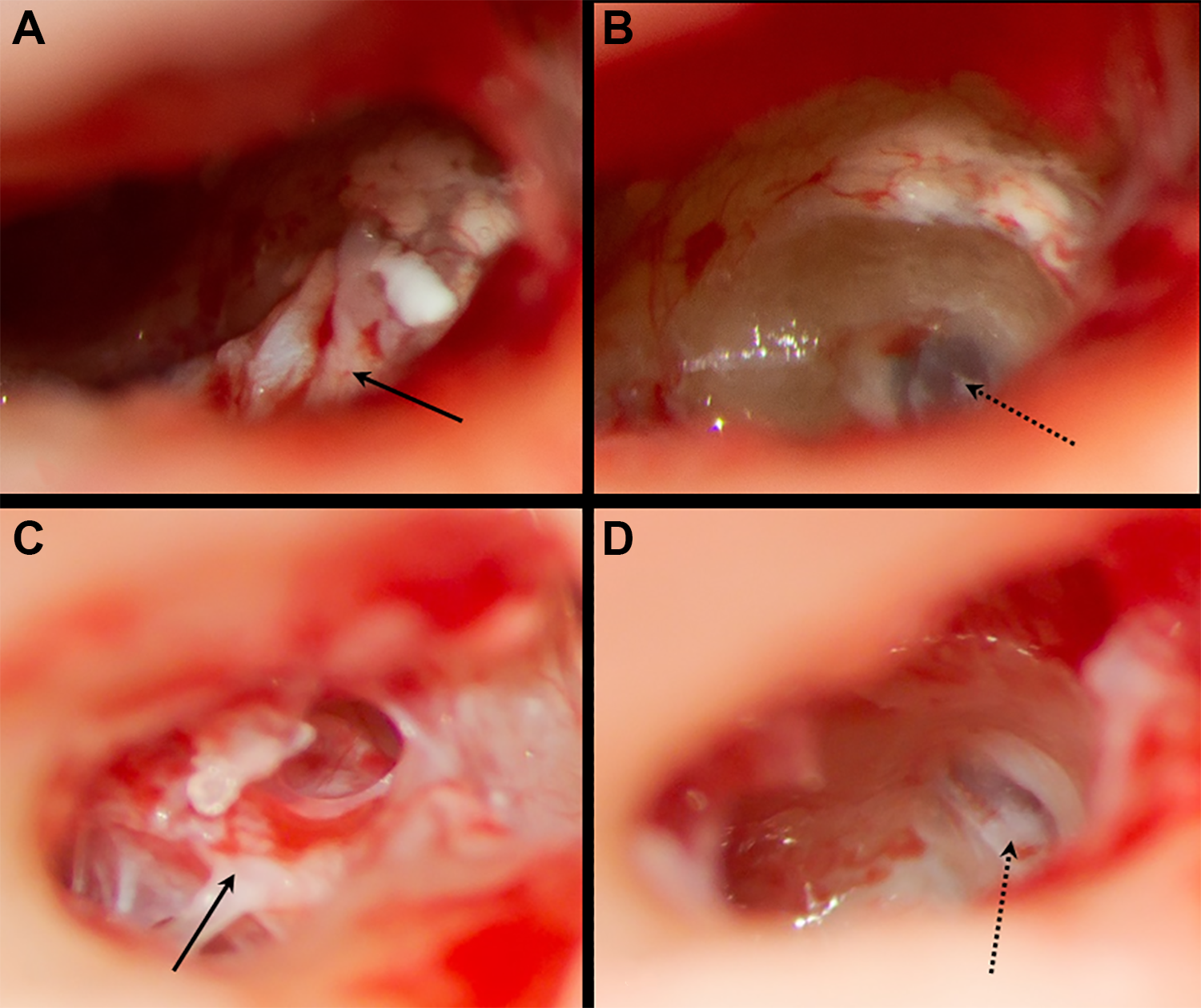
Intraoperative findings during cochlear implantation before (A, C) and after (B, D) tissue removing at the round window niche. Black arrows indicate tissue in the round window niche, dotted arrows point on the round window membrane. A, Patient No. 20 showing tissue in the round window niche impeding access to the round window. B, Patient No. 20 after tissue removing and drilling of the subiculum, the round window membrane can be clearly visualized. C, Patient No. 21 with tissue blocking the round window niche. D, Patient No. 21 with good view on the round window membrane after tissue removing and drilling of the subiculum.
The type of approach for electrode insertion was not influenced by remaining connective tissue and was based on the individual patients’ anatomy. Insertion of the electrodes was performed via the unaltered round window in 7 (33%) cases, whereas the round window was enlarged in 10 (48%) patients. A cochleostomy was performed in 4 (19%) patients. All electrodes were completely inserted. Postoperative computed tomography (CT)-scan of the temporal bone for position control of the electrode was performed in all but 1 patient who underwent transorbital X-ray examination confirming correct electrode position (Patient No. 1; CI24RE [CA]). CT imaging showed a complete scala tympani position of the electrode in 16 patients but revealed an electrode translocation from scala tympani to scala vestibuli in 4 patients all implanted with a Contour Advance electrode (Pat. No. 6, 11, 12, 14). No adverse effects due to extracochlear stimulation were observed. Consequently, no electrodes had to be switched off. In no case, a tip-fold over was detected. Patients’ characteristics are given in Table 1.
Patients’ Characteristics.
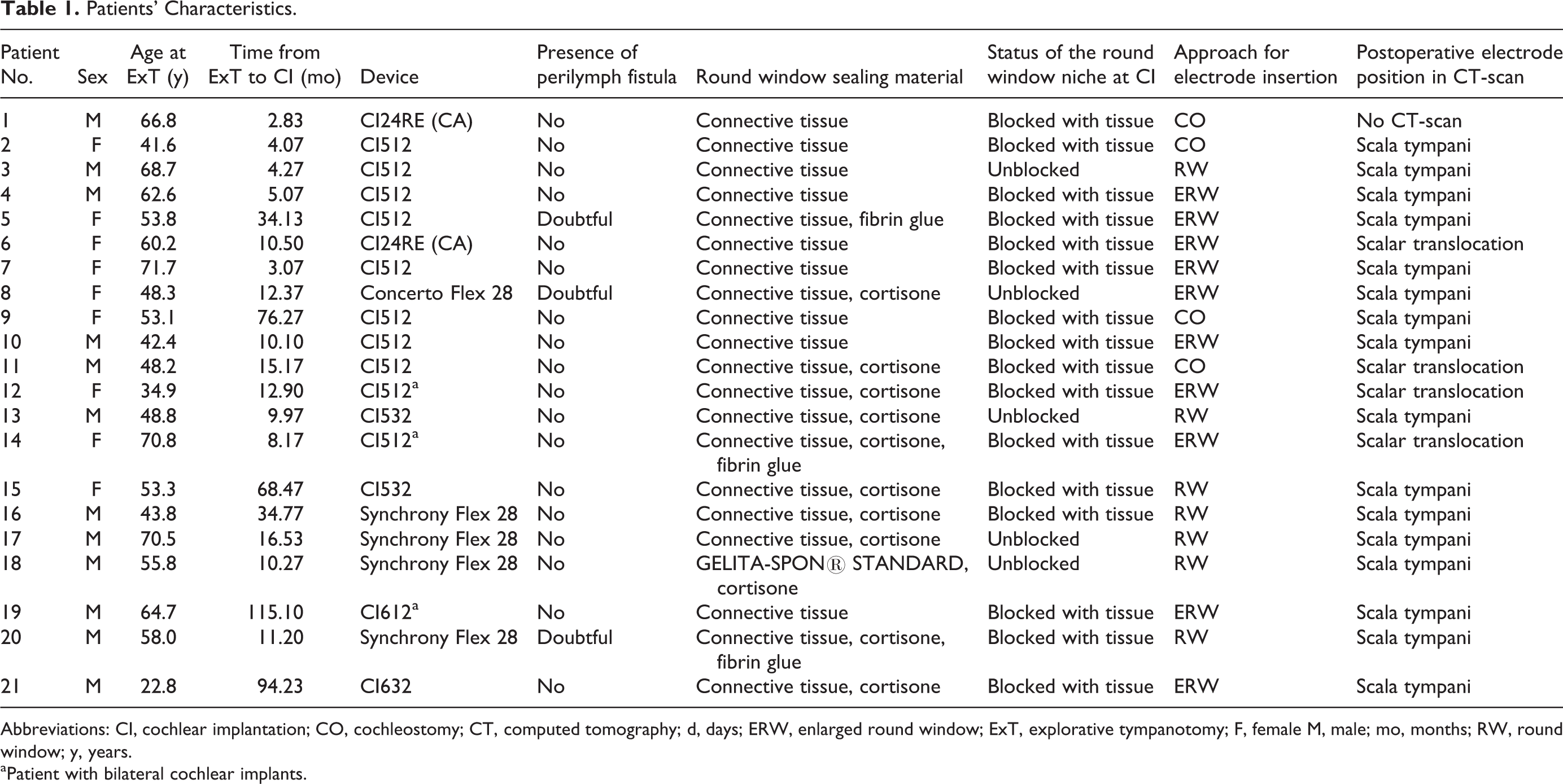
Abbreviations: CI, cochlear implantation; CO, cochleostomy; CT, computed tomography; d, days; ERW, enlarged round window; ExT, explorative tympanotomy; F, female M, male; mo, months; RW, round window; y, years.
a Patient with bilateral cochlear implants.
Hearing Results
Prior to ExT, the mean 4FPTA of all patients averaged 106.0 dB (±15.6 dB, min, 68 dB, max, 120 dB) and improved significantly by 10.0 dB until CI to 96.0 dB (±19.1 dB, min, 66 dB, max, 120 dB, Z = 2.48, P = .013, r = 0.54). The 4FPTA of the contralateral ear before CI was 43.0 dB (±41.2 dB, min, 2 dB, max, 120 dB). Pure-tone average thresholds are shown in Figure 2.
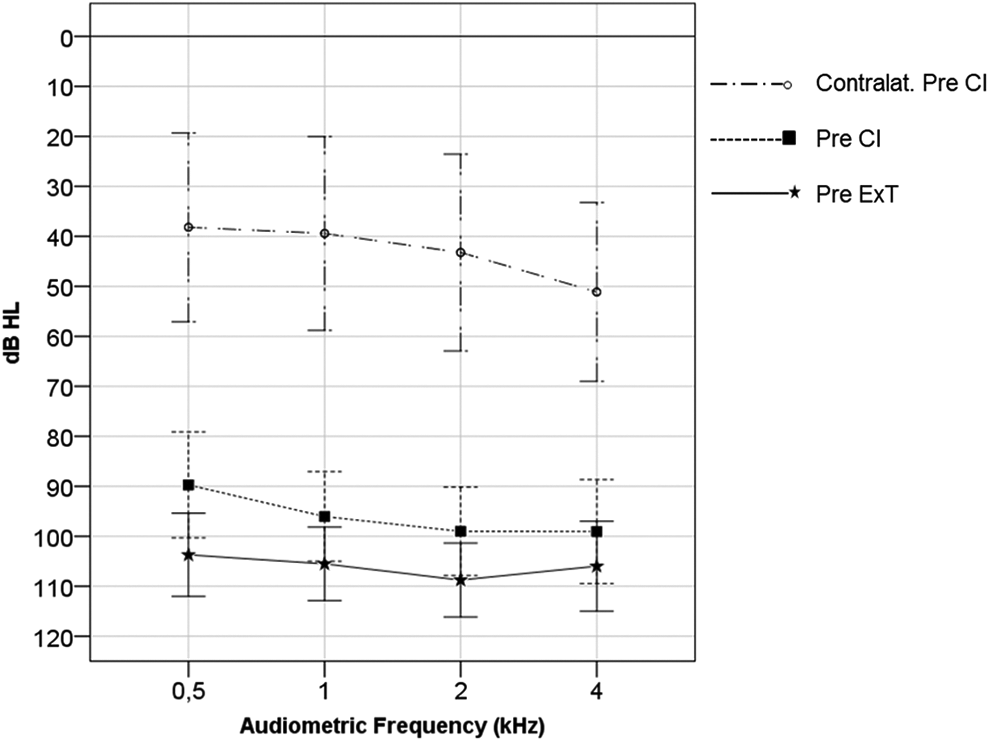
A 4FPTA before explorative tympanotomy (Pre ExT) and before cochlear implantation (Pre CI) as well as 4FPTA of the contralateral ear before CI (contralat. Pre CI); error bars indicating 95% confidence interval of the mean. dB HL indicates decibel hearing loss; 4FPTA, four-frequency pure-tone average; kHz, kilohertz.
Prior to CI, 12 patients had a maximum preoperative monosyllabic score (WRSmax) of 0%. Mean WRSmax for all 21 patients was 12.1% (±17.4%, minimum 0%, maximum 50%) with a median of 0%.
For WRS, the repeated measures ANOVA revealed a significant main effect “time” (F4,44 = 67.96, P < .001). Three months after CI, each of the 21 patients had a measurable WRS3m with a mean of 57.4% (±17.2%, min, 15, max, 90) that was significantly better compared to WRSmax (t(20) = 9.02, P < .01, r = 0.90) before CI. Additional 3 months later, the mean WRS6m (n = 16) was 66.9% (±18.8%; min, 15%, max, 90%) with a median of 70%. One and 2 years after implantation, mean WRS1a (n = 16) was 68.8% (±20.7%; min, 30%, max, 100%) with a median of 75% and WRS2a (n = 13) was 73.1% (±16.4%; min, 40%, max, 90%) with a median of 80%. Accordingly, 2 years after CI, the mean WRS2y was significantly increased (t(20) = 3.42, P = .005, r = 0.69) compared to WRS3m at 3 months postoperatively. In between times, improvements of the WRS were insignificant (WRS3m vs WRS6m vs WRS1y vs WRS2y, t ≤ 1.51, P ≥ .85). Hearing results for the 4 patients showing scalar translocation were not inferior to the group without translocation. Word recognition scores are visualized in a boxplot diagram in Figure 3.
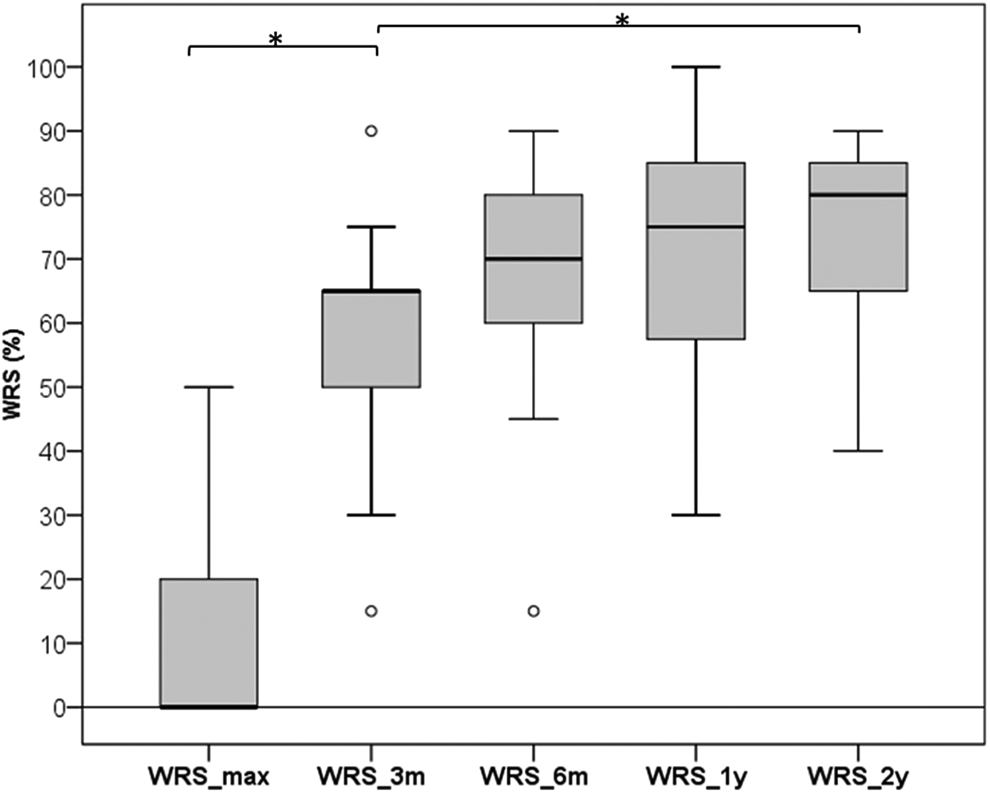
Boxplot diagram of pre- and postoperative word recognition scores. WRSmax = maximum preimplantation word recognition score for phonemically balanced monosyllabic words; WRS3m, WRS6m, WRS1y, WRS2y = word recognition score with cochlear implant 3 months, 6 months, 1, and 2 years after implantation. Star indicates a statistically significant difference.
Discussion
This study demonstrates that ExT with sealing of the round window membrane due to severe acute hearing loss does not negatively affect subsequent surgery for and rehabilitation with CI. Surgically, the round window niche can be expected to be blocked with connective tissue in the majority of patients, that is, in 76% of the presented cases. However, that tissue can be removed safely thus exposing an unaltered round window membrane. As presented, this allows for proper electrode insertion via standard approaches. Moreover, hearing rehabilitation of these patients is very satisfactory confirmed by short- and long-term follow-up.
Cochlea surgery has proven to be an effective and straight-forward surgical procedure with low complication rates. 11 However, electrode insertion may be impaired or even impossible based on changes of the cochlea in patients after head trauma, acute labyrinthitis, or otosclerosis.12-14 In patients with cholesteatoma or chronic suppurative otitis media, CI can be challenging and, in many cases, requires special operative strategies.15,16
By now, reports on CI in patients treated with ExT and sealing of the round window membrane are scarce. In their case report, Kleinjung et al reported a successful CI following ExT. However, they did not describe the anatomical findings in the middle ear and especially the status of the round window niche intraoperatively. 8 Postoperative X-ray examination revealed a correct electrode position but did not allow for the confirmation of the distinct intracochlear anatomical position of the electrode. Operating these patients, one can expect to free the round window niche from blocking tissue to gain access to the round window membrane itself. As presented, this can be performed successfully and safely leaving the round window membrane undamaged thus allowing the electrode to be inserted via standard approaches. Of note, all 4 electrode translocations occurred with the perimodiolar Contour Advance electrodes only that is consistent with findings by O’Connell et al reporting higher translocation rates for perimodiolar electrodes compared to lateral wall electrodes. 17 Recently, Liebscher et al detected a translocation rate of 32.3% in 99 Contour Advance electrodes which goes in line with our findings of 31%. 18 In this regard, our study collective is not associated with an elevated rate of scalar translocations.
With regard to the hearing results, the presented median improvement of WRS 6 months after CI compared to the maximum preoperative monosyllabic score was 70 percentage points. These results correspond to studies with larger amounts of patients that showed improvements of 65 percentage points and a median postoperative WRS of 65% to 78.9%.10,19-21 So far, there is no evidence that previously performed ExT has any negative effects on hearing rehabilitation in CI.
Patients with acute severe to profound sensorineural hearing loss can benefit from treatment with ExT.3-6,22 However, as it is an invasive procedure, it should be an ultima ratio when patients do not respond to intravenous and intratympanic cortisone treatment. Our study demonstrates that sealing of the round window membrane during ExT does not impede subsequent CI that remains a viable treatment option when hearing does not recover sufficiently over time.
The study’s limitations are due to the retrospective design and the number of patients that should be taken into account when interpreting the results. Furthermore, ExT was performed without standardized protocol by multiple surgeons. In contrast, all but 2 CIs were performed by 1 experienced physician that allowed for consistent intraoperative reports and results. Moreover, no control group was determined as this was beyond the scope of the study and complete follow-up had not taken place in all patients at the time of data analysis. However, the presented cohort is the largest reported so far displaying surgical and audiological outcomes of patients with CI after ExT.
In conclusion, when performing CI after preceding ExT, remaining connective tissue has to be expected blocking the round window niche. Tissue can be removed safely and does not alter the round window membrane allowing for proper electrode insertion via standard approaches. A previously performed ExT does not definitively increase the risk of dislocation or scalar translocation of the electrode during subsequent CI. Short- and long-term hearing results are satisfactory and comparable to the findings of other studies. Consequently, ExT with sealing of the round window membrane in patients with SSNHL does not impede subsequent CI that can still be performed safely.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.