
Abstract
Objective:
Investigate the effect of a targeted wellness program on burnout in Otolaryngology residents.
Methods:
Residents and faculty collaboratively developed a program aimed at improving resident wellness. Program implementation began in July of 2018 and after 1 year, residents evaluated the program’s effects on burnout. We used the Maslach Burnout Inventory (MBI) and a Likert scale to evaluate the effects of the program.
Results:
After 1 year of the resident wellness program, the MBI results showed an increase in the number of residents in the “engaged” category and a decrease in those rated as “burnout.” Residents rated favorably initiatives grouped into the following themes: time away from work, faculty engaging with residents outside of the hospital environment, efforts to enhance residents’ self-efficacy, fostering a positive culture among residents, and providing easy access to physical activity. The majority of initiatives were targeted to the “culture of wellness” domain, as defined by the Stanford Well MD framework. Our program targeted to a lesser extent the other 2 domains, “efficiency of practice” and “personal resilience.”
Conclusion:
After 1 year, the wellness program resulted in a trend toward improving burnout. Future efforts should be focused on targeting the multidimensional drivers of burnout as defined by established wellness frameworks. Realizing new stressors brought on by the COVID-19 pandemic will also be an area of active effort and research.
Introduction
Burnout is an epidemic in health care affecting individuals at all levels of care: medical students, residents, nurses, administrators, and practicing clinicians. Burnout is an occupational syndrome defined by an extended response to job stressors and is characterized by emotional exhaustion, depersonalization, and reduced sense of personal accomplishment. In other words, feeling emotionally overextended and exhausted by one’s work, cynical or detached from the job, or lacking satisfaction in one’s work are all telltale signs of burnout. 1
Burnout among physicians has increased in prevalence in recent years. In a study that surveyed physicians using the validated Maslach Burnout Inventory (MBI), 54.4% of physicians reported at least one symptom of burnout in 2014 in comparison to 45.5% in 2011. 2 Research has also demonstrated that burnout leads to increased medical errors, decreased quality of patient care, and higher suicidal thoughts among health care professionals. 3 -6 Without proper intervention, burnout among health care workers will continue to spread, negatively impacting both health care providers and the patients who rely on them.
In the field of Otolaryngology-Head and Neck Surgery, there is evidence that training within our specialty is not immune to this epidemic of burnout. In a nationwide sample from 2007, the majority of Otolaryngology residents reported at least a moderate level of burnout. 7 This study is but one of several that have linked burnout to the problem of excessive work hours. 8 Although a major factor in the development of burnout, overwork is not the only issue linked to decreased resident wellness. Factors such as dissatisfaction with faculty or personal relationship and family stressors also play a major role. 7,9 Certainly, burnout is a multifactorial issue that varies based on an individual’s level of resilience and each program’s focus on a work–life balance. However, given the nature of the problem it follows that potential solutions must also be multidimensional. Focus on resiliency efforts alone is insufficient to solve this growing burnout crisis. 10 Additionally, there is evidence that efforts made on behalf of an organization, rather than individual effort, are more successful at addressing burnout. 11 Specifically, changes in schedules and reduction of workload were effective at reducing burnout, as were efforts to foster a culture of teamwork and increase the level of decision-making among physicians in their own organization. Although individual measures such as physician burnout education, mindfulness training, or cognitive behavioral training are important factors in mitigating burnout, larger departmental and institutional change is likely needed to sufficiently target the lasting effects of physician burnout.
In light of this evidence, we sought to institute a department supported, resident-led wellness program within our department. The initiatives created by the wellness committee were motivated by the evidence that exists regarding the drivers of burnout among our peers, along with the personal insights provided by a member of each post-graduate year (PGY) class within our program. The aim of this study was to investigate the effect of the targeted Resident Wellness Program on overall burnout as measured by a validated burnout survey while also evaluating the reception of each wellness initiative on residents’ subjective feeling of burnout. Determining which wellness program components successfully mitigated the drivers of burnout in these residents could lead to improvements in resident well-being nationally.
Methods
Otolaryngology Resident Wellness Program
Launched in the academic year of 2018-2019, a resident-led, faculty-supported committee developed the resident wellness program. The committee consisted of one resident per PGY class and 2 faculty members. Primarily, the committee developed and implemented department-specific initiatives to promote work–life balance; support physical, psychological, and emotional health; and provide a peer support and advocacy network throughout residency. The committee also curated the institutional and national wellness resources available to residents.
The wellness program and the level of burnout of our residents were evaluated annually using the gold-standard measurement in burnout research, the MBI. Additionally, we sought feedback of program initiatives using a Likert scale in an effort to refine the program from year-to-year.
The Maslach Burnout Inventory-Human Services Survey is a validated instrument to measure occupational burnout in individuals in the health care industry. This psychological inventory consists of 22 items assessing levels of burnout in 3 traditional categories: (1) Emotional Exhaustion, (2) Depersonalization (Cynicism), and (3) Personal accomplishment (Inefficacy). First introduced in 1981, the MBI has been used by countless groups of researchers spanning numerous industries. Recently, the traditional scoring mechanism of assigning low, moderate, and high levels of burnout within each category has come into question. 12 For this reason, we followed the latest recommendation from the survey’s cocreators regarding interpretation of the survey data. In brief, the mean score and standard deviation within each category was used to calculate a critical high value against which all individuals were compared. 13 Each individual was then labeled among 5 established profiles based on their combination of high scores: (1) Engagement (low on all dimensions), (2) Ineffective (high on inefficacy only), (3) Overextended (high on exhaustion only), (4) Disengaged (high on cynicism only), and (5) Burnout (high on all 3 dimensions). The 5 profiles are considered a continuum of worsening burnout from Engaged (least burnout) followed by Ineffective, Overextended, Disengaged, and Burnout (most burnout).
The Likert scale from −2 to +2 (corresponding to markedly worsened burnout, mildly worsened burnout, neutral, mildly improved burnout, and markedly improved burnout). The Likert scale asked residents to rate wellness initiatives with higher numbers representing a more favorable impression. All interventions and resources comprising the wellness program are found in Table 1.
USC Caruso Department of Otolaryngology Wellness Program Components.
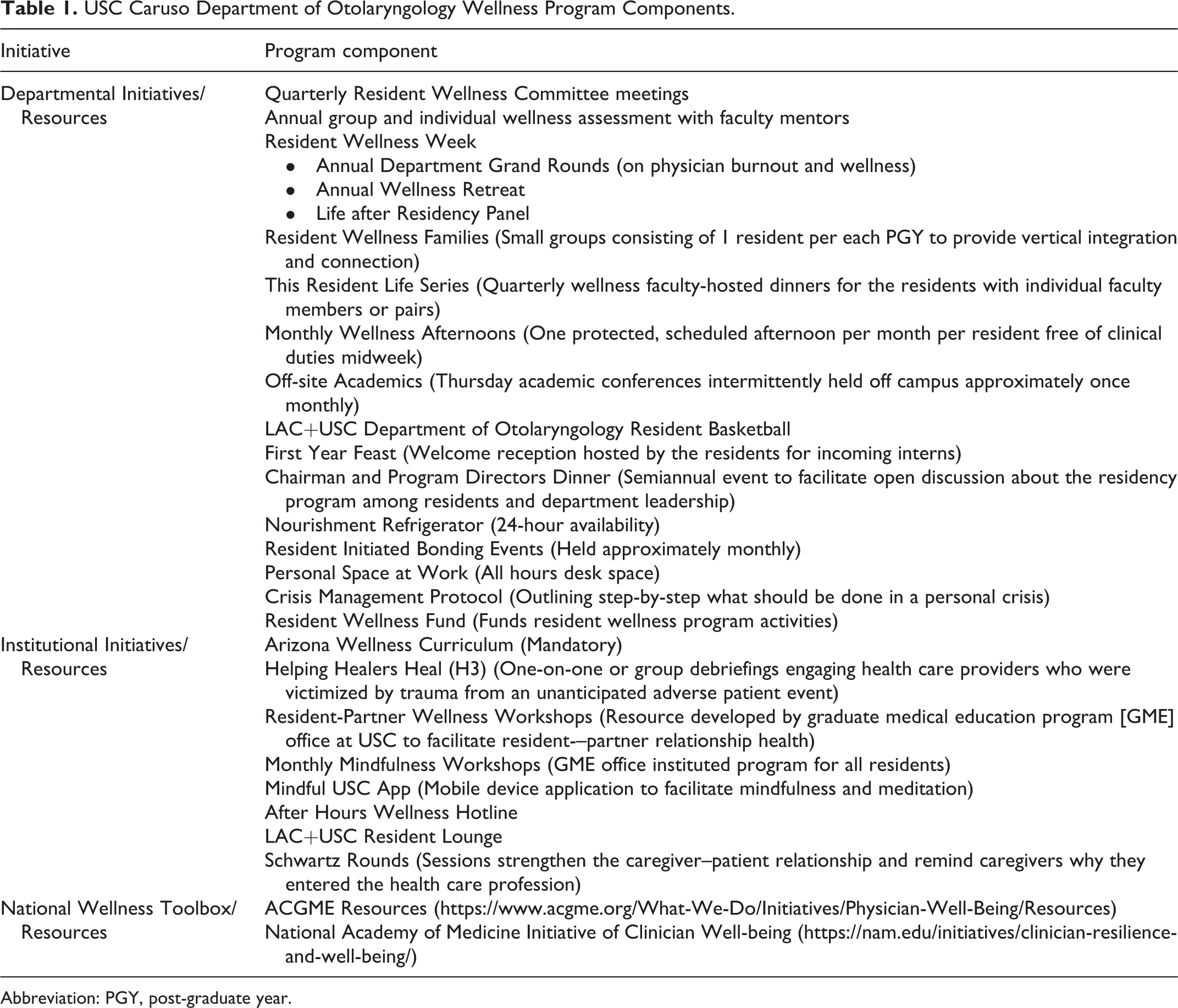
Abbreviation: PGY, post-graduate year.
Study Design and Procedures
Our study proposal was submitted to and approved by the Institutional Review Board at the Keck School of Medicine of USC. Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article. A program coordinator provided the authors with a deidentified codified document containing resident MBI scores from pre- and postimplementation of the first year of the wellness program and Likert scale results from resident evaluation of the various wellness initiatives. Wellness initiatives were both generated by the wellness committee (departmental) and provided by larger institutions (USC, GME). There was an option to mark not applicable if a resident did not utilize a component.
The MBI results and percentage of residents who fell into each of the 5 profiles were calculated for 2018 and 2019 (pre- and postimplementation). The Likert scale scores of each program component were averaged and reported from high to low. Positive average scores indicated a majority sense that the initiative improved burnout while negative average scores worsened burnout. Scores rated as 0 were considered neutral.
Results
Maslach Burnout Inventory-Human Services Study
Burnout was assessed in 20 residents across all PGY levels pre- and postimplementation of the wellness program using the MBI from 2018 to 2019. The percentages of residents who fell into each of the 5 profiles from least to most burnout were as follows: For 2018, 40% were Engaged (8/20); 20% were Ineffective (4/20); 25% were Overextended (5/20); 5% were Disengaged (1/20); and 10% were Burnout (2/20). For 2019, 50% were Engaged (10/20); 10% were Ineffective (2/20); 30% were Overextended (6/20); 5% were Disengaged (1/20); and 5% were Burnout (1/20) (Figure 1).
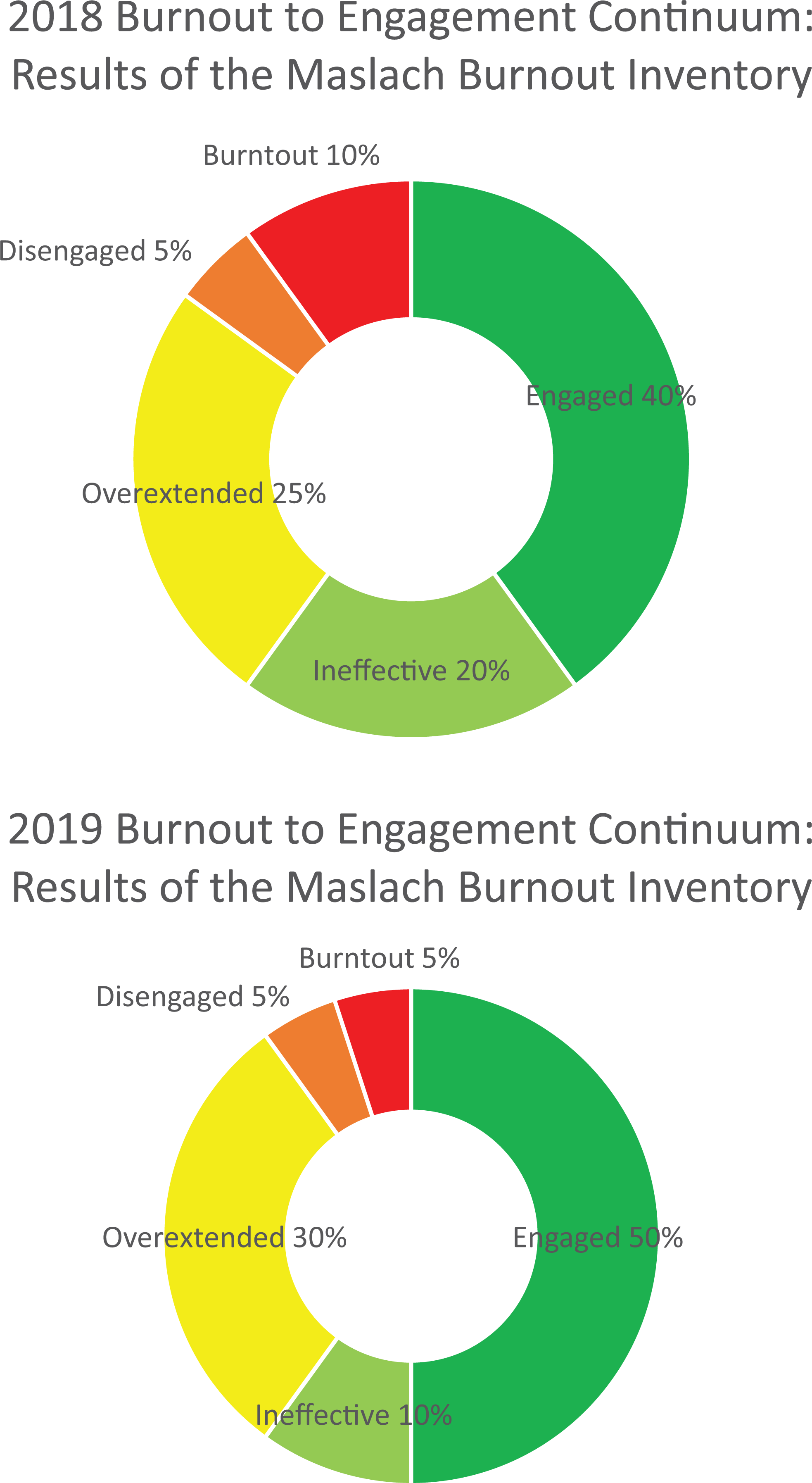
The Malasch-Burnout Inventory. The 5 burnout profiles from least to worst burnout were Engaged, Ineffective, Overextended, Disengaged, and Burnout. The distribution of residents in these profiles are shown for 2018 and 2019.
Program Evaluation Likert Scale
A majority of the departmental wellness committee initiatives scored favorably at the 1-year evaluation. The following program components were rated by residents as improving their overall sense of burnout (positive scores) in order of descending rating value using the Likert scale: Annual Wellness Retreat, Resident Initiated Bonding Events, Monthly Wellness Afternoons, This Resident Life Series, Nourishment Refrigerator, Annual Wellness Grand Rounds, Chairman and Program Directors’ Dinner, Program Review Meetings, First Year Feast, Off-site Academics, Physical Activity Program, Wellness Families Program, and Individual Review Meetings (Supplementary Figure).
The MBI Survey, Crisis Management Protocol, After-Hours Hotline, National Academy of Medicine toolbox, and LAC+USC Resident Lounge were scored as neutral to slightly favorable.
Institutional optional wellness resources and toolboxes scored neutral. Specifically, those program components included Partner Workshops, Mindfulness Workshops, Mindful USC Phone Application, Schwartz Rounds, ACGME Resource Page, and the Keck Wellness Program. Online wellness programs both mandatory and nonmandatory were rated to worsen burnout (negative scores). This includes the Helping Healers Heal programming and the Arizona Wellness Curriculum. In summary, departmental initiatives were scored favorably while the national and institutional wellness resources scored neutral or negatively.
Discussion
Burnout remains a systemic problem in medicine affecting doctors from early in their careers as medical students through their time as attendings. Although not a new problem, recent evidence suggests that health care professionals suffering from burnout may produce negative outcomes in patient care. Given the negative effects on both providers and patients, efforts to make structural changes to reduce burnout are of critical importance to improve the quality of care for patients and improve the quality of life of health care providers. The resident-driven wellness program was the first in our history to attempt to create initiatives to mitigate factors contributing to burnout. With the support of faculty and administrators, we formally integrated this committee and its initiatives into the Otolaryngology residency program at USC.
Our initial effort to address burnout within our training program proved to be somewhat narrow in scope, as it was focused on the important yet obvious driver of overwork and a lack of work–life balance. Fortunately, this initial attempt at improving our well-being led us to discover the vast body of knowledge and research that exists in the field of occupational burnout. Efforts to prevent burnout and promote well-being have produced the concept of comprehensive wellness frameworks. These models, like the one used by the Substance Abuse and Mental Health Services Administration (SAMHSA), define dimensions of wellness that can be used to explore the drivers of wellness and exact positive changes in individuals suffering from mental or substance abuse disorders. 14 Others are more tailored to the health care community, like Stanford’s Well MD Model, which defines 3 domains that encompass the major factors involved in physician wellness. The “culture of wellness,” “efficiency of practice,” and “personal resilience” domains were identified as key arenas of wellness among physicians and are used to design initiatives at their institution. 15 Through this framework, we can examine our initial effort at a wellness program, where some resemblances exist between the de novo initiatives enacted by our committee and the framework, and in what domains we fell short in creating a comprehensive program.
Initiatives targeting faculty engagement and promotion of a positive department culture were among the highest rated components by our residents. This included the most favorably rated component, the annual wellness retreat, which promoted bonding between residents and engaged faculty members. Undoubtedly, this is what the Well MD model intended by their “culture of wellness” domain. Our results indicate the importance of residents actively building a positive culture with each other and with faculty as part of maintaining a positive and nurturing department culture. Other components that follow this theme which were all rated favorability were the This Resident Life series, the annual department dinner with the Chair and Program Director, and the first-year feast. These interventions cultivated departmental cohesiveness, leadership support, and appreciation which align with residents’ favorable evaluation of these components. The “culture of wellness” domain appears to be the most accurately targeted by our wellness committee and may be the main driver of our modest success. However, this is just one aspect of the framework that should be addressed in future iterations of the program.
The “personal resilience” domain is equally weighted in the Well MD framework and undoubtedly has a major impact on individual well-being. After review of our program, the initiatives that we considered as falling into the “personal resilience” domain included the annual group and individual wellness assessments with faculty mentors, the resident wellness families program (support system), monthly wellness afternoons (self-care, life needs), the 24-hour nourishment refrigerator, and the crisis management protocol. With these initiatives, the burden of fostering resilience is shared among peers and the leadership with whom they work. Although less obvious, the wellness program was targeted to some aspects of personal resilience which were well received by the programs’ trainees.
Admittedly, the “efficiency of practice” domain presented a larger challenge to address and was not the focus of our initial wellness initiatives. Well MD defines this domain as “Workplace systems, processes, and practices that promote safety, quality, effectiveness, positive patient and colleague interactions, and work-life balance.” The fact that our department is but one of dozens of departments within the larger hospital system, which in itself is a small part of the larger US health care environment, makes it difficult to enact sweeping changes in such areas as the electronic medical record, hospital interdepartmental workflow, and patient wait times or appointment availability. These examples, to name a few, could go a long way in optimizing the day-to-day workflow of our residents, but may be out of the scope of this project. Nevertheless, we must attempt to manage the portion of this domain that is within our control. Our creation of personal resident workspace (all hours desk space) and our discussions of day-to-day workflow during our quarterly wellness meetings can be seen as a starting point for future initiatives in this arena. Future attention to this domain would serve the residency program well despite the limitations inherent in broader drivers of systemic burnout.
The initial results of the MBI placed 40% of residents in the least troublesome category, “engaged,” and 10% were in the most, “burnout.” The remaining 50% of residents scored above the critical threshold in 1 of the 3 categories and were either labeled “ineffective,” “overextended,” or “disengaged.” After 1 year of the resident wellness program, there were signs of improvement. The number of “engaged” rose to 50% and the number of burnout fell to 5%, leaving just 45% in the remaining 3 categories. Although it is difficult to say whether the outcome is significant due to the small sample size, a trend in the positive direction was considered favorable over the alternative. Furthermore, as the wellness program enters subsequent years, we will start to be able to trend further out and expand our sample size to include new residents to the program.
There are several limitations in our program’s scope and measured outcomes. The most obvious is that the differing responsibilities of residents as they move through residency affects their level of burnout in a way that is immutable to the wellness program. However, with more years of data we will be able to parse out the effects of specific PGY levels with other drivers of burnout. For now, as mentioned, the small sample size and short follow-up time of the study make it difficult to draw any statistically significant conclusions. We also acknowledge that the use of a Likert scale is not a valid measure of burnout. This survey was only meant to provide feedback to the committee on which wellness initiatives were well received and which needed improvement in subsequent years. Additionally, we are hindered in our ability to change larger systemic drivers of burnout, however, the aspects of “efficiency of practice” which are within the reach of the tools disposable to our department should be further explored. Continuous quality improvement projects are already part of the residency curriculum, and perhaps a marrying of these 2 programs can yield positive results in mitigating the factors of burnout. Finally, the inclusion of institutional mandatory activities as part of the wellness program may have created a counterproductive effect that could have diminished the benefits of other wellness program components. This is not to say that these broad wellness tools are not effective when used in earnest, but the feedback elicited from our residents indicated that the engagement with these tools was suboptimal.
Undoubtedly, the COVID-19 pandemic has also presented a new challenge that was not foreseen at the initiation of this program. Namely, a number of our initiatives were focused on team activities which include socializing in and out of the hospital and were essential to maintaining a wellness culture. We have tried to transition as many of these initiatives as we could online, while being wary of overdoing screen time. We have seen some success with This Resident Life series, where attending physicians share stories and offer wisdom gained over the course of their career. Additionally, the wellness committee meetings, assessments with mentors, and the wellness week featuring grand rounds and the life after residency panel have been successfully transitioned online by our residents. Nevertheless, there is no substitute for physical activity and socializing outside of the home and workplace. The working hypothesis of our group is that a focus on personal resilience initiatives may mitigate the isolating effects of the pandemic. We expect that the MBI results from this year will reflect the stress brought on by the COVID-19 pandemic and may reveal a higher prevalence of burnout. However, with comprehensive wellness frameworks as a guide, our committee is actively working to refine and adjust our initiatives to address new stressors brought on by the pandemic. The use of a framework should prove even more important when the drivers of burnout reach uncharted territory like that brought on by a global pandemic.
Conclusion
A targeted resident-wellness program was implemented by our committee of resident and faculty advocates within the Otolaryngology residency program at USC and after the first year of implementation there was a trend toward improving burnout. However, new programs are best served to follow a wellness framework, such as Stanford’s WellMD program, to achieve maximally comprehensive and effective results.
Supplemental Material
Supplemental Material, sj-xls-1-ear-10.1177_01455613211009139 - Targeted Wellness Initiatives Are Most Effective for Reducing Otolaryngology Resident Burnout
Supplemental Material, sj-xls-1-ear-10.1177_01455613211009139 for Targeted Wellness Initiatives Are Most Effective for Reducing Otolaryngology Resident Burnout by Joseph R. Acevedo, Jamie A. Schlacter, Tamara N. Chambers, Lia K. Jacobson, Ronica Yalamanchili, Bhavishya Clark, Dorothy Pan, Niels C. Kokot and Michael M. Johns in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
This work was presented as a poster at the Triological Society Combined Sections meeting, January 25, 2020, and has not been submitted for publication in any journal. This study was approved by the Institutional Review Board at the Keck School of Medicine of USC. All procedures in this study were conducted in accordance with the Institutional Review Board at the Keck School of Medicine of USC. Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Acknowledgments
The authors would like to acknowledge Mostyn S. Fero, BA, for his role in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.