
Abstract
When fitting hearing aids, patients are required to make an earmold impression material for device fixation. It usually causes no problems, although in rare cases, the earmold passes through the middle ear through tympanic membrane perforations. 1 – 3 Foreign bodies may cause a delayed inflammatory reaction and deterioration of aeration, especially in the Eustachian tube. Herein, we report a rare case of earmold impression material as a foreign body in the middle ear that required surgical removal.
Case Presentation
A 77-year-old woman was referred to a tertiary referral hospital for suspicion of a foreign body in the middle ear. The patient had a history of chronic otitis media with a long-standing hearing disturbance. A hearing aid was prescribed, and an impression molding procedure was performed at a local hearing aid shop. She complained of otalgia ever since the molding material entered her ear canal. On endoscopic examination, the patient showed tympanic membrane perforation with erythema of the canal wall and a visible middle ear foreign body (Figure 1A). Mixed hearing loss was assessed using pure tone audiometry (Figure 1B). A high-resolution temporal bone computed tomography (TBCT) scan was performed, which revealed silicone filling the middle ear, intercrural areas of the stapes, and extending to the Eustachian tube (Figure 2A). After antibiotic treatment, the otalgia did not improve. The patient underwent an intact canal wall mastoidectomy with facial recess approach to remove the foreign body. A retroauricular incision was made, after which mastoidectomy was performed. After granulation tissue was removed, we observed earmold impression material filling the middle ear both through the perforated tympanic membrane and epitympanum. We confirmed that the foreign material was not fixed in the middle ear cavity and ossicles although the stapes was encased with the material via a combined transcanal-facial recess approach. With meticulous dissection, the foreign material was successfully removed en bloc via a combined transcanal–transmastoid approach, preserving the ossicles and chorda tympani nerve. After removing the foreign body, we confirmed through an otoendoscope that there was no foreign body remaining in the middle ear cavity including hypotympanum and the Eustachian tube. The material had the same shape as the middle ear cavity and was completely removed (Figure 2B). We confirmed that the foreign body did not extended into the mastoid antrum. There was inflammation and granulation tissue in the middle ear and mastoid antrum; however, the ossicles were not damaged. Surgery was performed without any other complications. The patient did not complain of postoperative dizziness or facial nerve palsy, and the otalgia gradually improved.
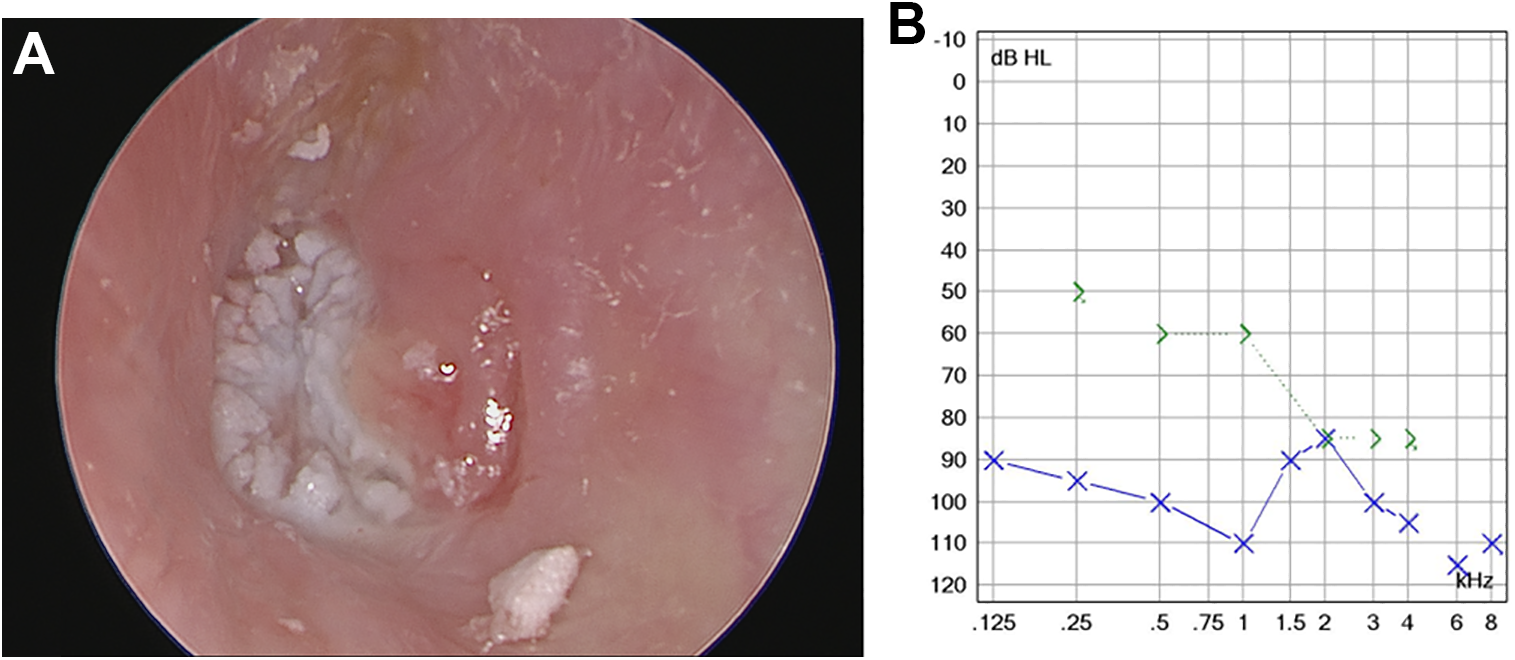
A, An endoscopic view of the left ear canal during the initial visit. Earmold impression material filling the middle ear can be observed through the perforated tympanic membrane. (B) Preoperative pure tone audiometry of the patient. Mixed type hearing loss was found in the left ear.
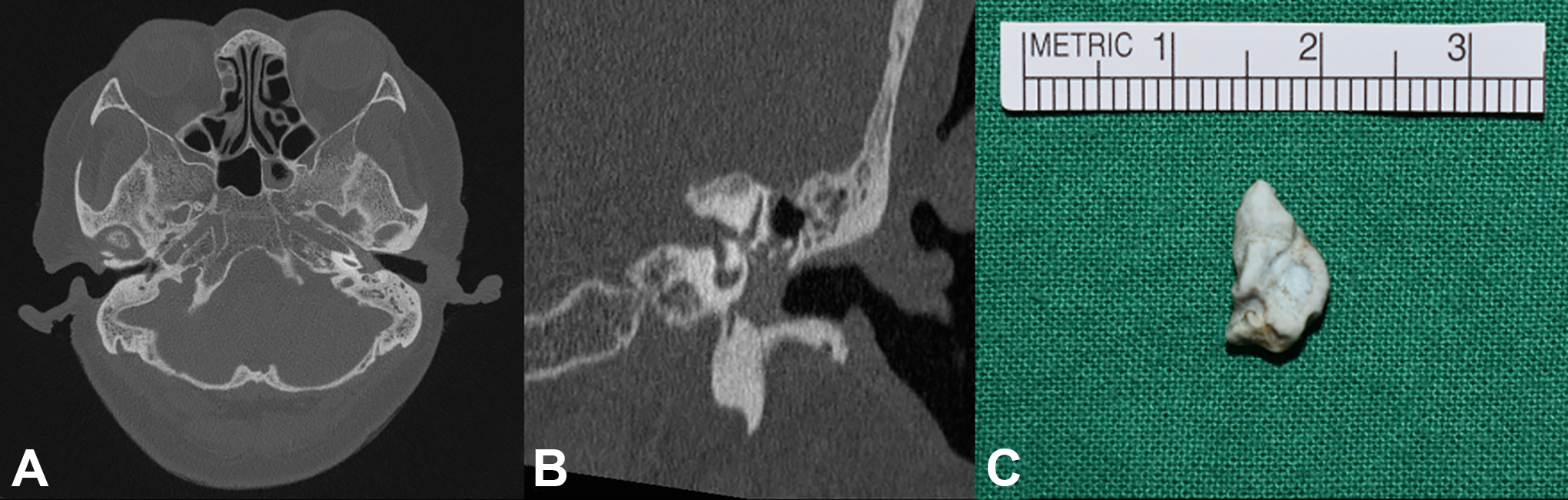
A, Temporal bone computed tomography image of the left temporal bone showing the foreign materials in the left middle ear cavity extended to the Eustachian tube. (B) The foreign material in the left middle ear was in contact with the ossicles on a coronal view computed tomography (CT) image. (C) The foreign material was totally removed en bloc.
Discussion
Hearing aids are widely used rehabilitation methods for hearing loss. 4 According to the Korean Ministry of Health and Welfare statistics annual report for 2020, 13.2% of the population aged 65 years’ experience hearing impairment, and the rate of hearing aid use will increase in the near future. 4 In the Republic of Korea, hearing aids are prescribed either after careful examination by an otology specialist or directly by an audiologist at local hearing aid shop without consulting an otology specialist. Producing a hearing aid mold is not difficult for experienced personnel. However, molding materials may trigger serious complications such as hearing loss and dizziness, and perilymphatic fistula due to the foreign body could occur if there is any history of chronic otitis media or current suspicion of ear infection. According to US regulations, hearing aid providers should check patients’ history of external ear deformities, otorrhea, sudden hearing loss, dizziness, an air–bone gap >15 dB, cerumen impaction, or otalgia. 5 In the case of acute onset of symptoms such as otalgia, tinnitus, dizziness, nausea, and vomiting during the mold-making process, early surgical intervention is essential to prevent cochleovestibular sequelae. 5 During foreign material removal, adequate visualization and careful dissection are mandatory, not a simple “blind” removal. 3 In addition, preoperative TBCT is an essential diagnostic tool to identify the range of the foreign material. In this study, we found that significant complications developed during hearing aid earmold impression taking. Hearing aid-dispensing audiologists should be trained in appropriate educational programs with possible external or middle ear problems by otology specialists. In addition, hearing aid impression material–related complications should be immediately referred to an otology specialist to prevent irreversible complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.