
Abstract
The treatment of complete subglottic stenosis (SGS) remains a challenge due to anatomic and technological limitations. Placement of the Montgomery T-tube is an effective treatment option. For complete SGS patient combined with lower trachea collapse, the ventilation management during the T-tube insertion process is more complicated. Here, we report a case with complete SGS combined with severe lower trachea collapse, which was successfully managed with T-tube insertion under extracorporeal membrane oxygenation.
Introduction
The treatment of complete subglottic stenosis (SGS) remains a challenge due to anatomic and technological limitations. Placement of the Montgomery T-tube is an effective treatment option. 1 During the process of T-tube insertion, the airway must be shared by a respiratory interventional physician and anesthesiologist, and this provides a challenge to ventilation management. 2 For complete SGS patient combined with lower trachea collapse, the ventilation management is more complicated. Here, we report a case with complete SGS combined with severe lower trachea collapse, which was successfully managed with T-tube insertion under extracorporeal membrane oxygenation. As far as we know, similar cases have not been reported yet.
Case Report
A 32-year-old female with a tracheostomy tube for 7 months was admitted to our hospital in October 2018. She experienced glottic edema due to severe drug allergy 7 months ago, for which tracheostomy was performed. The patient remained with the tracheostomy for the next 7 months during which time several attempts at decannulation failed. Then, she was transferred to our hospital. Chest computed tomography showed complete SGS located 1 cm below the glottis for a length of 2 cm. Bronchoscopy revealed complete SGS (Figure 1A) and granulation hyperplasia at the distal end of the tracheostomy cannula (Figure 1B). The patient occurred respiratory distress during bronchoscopy; therefore, emergency tracheal intubation was performed through the tracheostomy stoma. Further bronchoscopy revealed severe collapse of the lower trachea extending to the level above carina (Figure 1C).
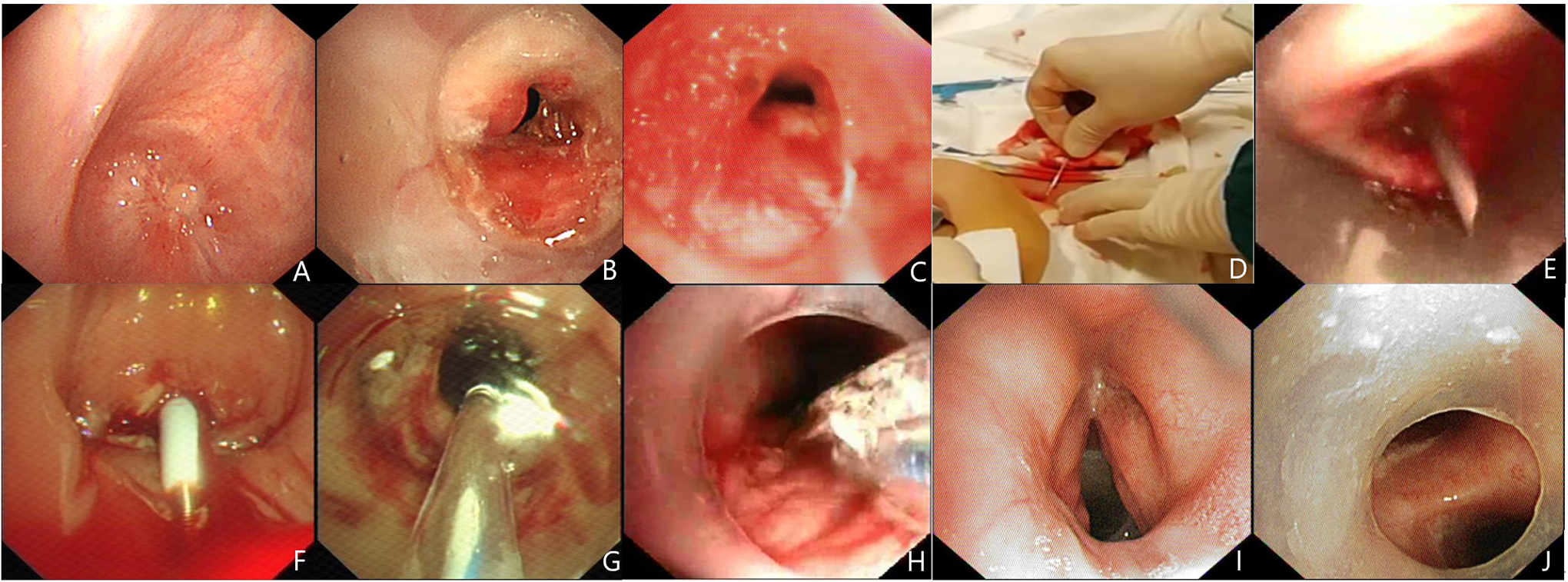
The manifestation on bronchoscopy. A, Bronchoscopy showed complete subglottic stenosis. B, Granulation hyperplasia at the distal end of the tracheostomy cannula. C, Bronchoscopy showed collapse of lower trachea. D, Reverse puncture using an introducer needle through the tracheostomy stoma. E, Introducer needle tip pierced through the occlusion tracheal segment. F, A guidewire and a tissue dilator were inserted to create a pinhole opening. G, Subglottic stenosis was dilated by balloon sequentially. H, The lower limb of T-tube was pushed forward with balloon expansion assistance. I, The proximal end of the T-tube was 0.5 cm below glottis. J, The distal end of T-tube was near the carina.
Tracheal resection and reconstruction could not be performed due to multiple segmental tracheal stenosis. Bronchoscopic intervention was considered. However, the complex tracheal condition provided a large challenge to patient’s ventilation management during operation. After discussion, we decided to use ECOM support during the operation.
Extracorporeal membrane oxygenation was deployed in a veno-venous configuration, then the tracheal tube was removed. The patient was general anesthetized and a 14-mm rigid bronchoscope (Karl Storz) was inserted through the oral cavity. The complete SGS was reverse punctured with the introducer needle of a central venous catheterization set through the tracheostomy stoma (Figure 1D). Under the direct observation of rigid bronchoscope, the introducer needle tip pierced through the occlusion tracheal segment after several attempts (Figure 1E). Subsequently, a guidewire and a tissue dilator were inserted using the Seldinger technique to create a pinhole opening (Figure 1F). A needle-shaped electrical knife was applied carefully along the guidewire to make an incision in the stenotic area followed by balloon dilatation (Boston Scientific) according a 12-13.5-15mm sequence (Figure 1G). Then, the rigid bronchoscope was gradually passed through the stenosed trachea to the upper level of tracheostomy stoma.
Next, a flexible bronchoscope was passed through the horizontal and lower limbs of the T-tube (12-mm internal diameter, 29-mm upper limb, 72-mm lower limb, Boston Medical Products Inc) and was inserted into lower trachea through the tracheostomy stoma. A balloon catheter was inserted through the bronchoscope biopsy channel to dilate the collapsed lower trachea, and the lower limb of the T-tube was gradually pushed forward, which eventually traversed the collapsed segment successfully (Figure 1H).
The upper limb of T-tube was inserted into subglottic trachea with the assistance of rigid forceps and the whole T-tube was placed successfully. The proximal edge of the T-tube was 0.5 cm below the glottis (Figure 1I), and the distal edge was near the carina (Figure 1J).
The patient developed glottic edema after operation which was subsided 8 hours later. Then, ECOM support was withdrawn. Patient had no complaints of discomfort after the procedure and was discharged 1 week later. Follow-up bronchoscopy was performed 4 months after the procedure, and there was no sign of granulation tissues proliferation on both edges of T-tube. No obvious sputum retention was found in the T-tube. She was encouraged to do saline atomization daily and self-expectorate. As of last contact, 2 years post-operation, she was doing well with no breathing issues.
Discussion
The case reported here had complete SGS accompanied with lower trachea collapse, which was an extremely complicated airway disease. Tracheal intubation or extended tracheostomy cannula could be used to pass through the collapsed lower trachea to maintain breath; however, the patient would have to endure poor quality of life and loss of phonation. Therefore, Montgomery T-tube, which could maintain airway patency and phonation, was the preferred treatment. 3
There were several challenges during the insertion process of T-tube for this patient. The first one was respiratory management. During the process of SGS recanalization or T-tube insertion, the tracheostomy cannula had to be removed sometimes, thus causing short-term interruption of ventilation. For patient with a normal lower trachea, the tracheostomy cannula could be reinserted if oxygenation declines obviously. Unfortunately, due to the severe collapse of lower trachea, this method would not work for this patient who might be at risk for asphyxia if the tracheostomy cannula was removed. Therefore, ECOM support instead of conventional ventilation was used and oxygenation during T-tube insertion was well maintained.
The second challenge was the recanalization of complete SGS. Complete tracheal stenosis is an uncommon, extreme form of postintubation or post-tracheostomy tracheal stenosis with only a few reported cases. Different teams have reported different recanalized methods.4-6 In fact, the top-down recanalization method is extremely risky due to the inability to accurately assess the distal airway. In this report, we used the introducer needle of a central venous catheterization set to perform reverse puncture through the tracheostomy stoma. Under the direct observation of rigid bronchoscope, the tip of puncture needle could be observed when it pierced through the occlusion tracheal segment. This method has been proved safe and effective in our center.
The third challenge was the insertion process of T-tube. In the conventional T-tube insertion process, the lower limb of T-tube was inserted with the help of a hemostat. 1 However, this method could not work for this patient due to the collapse of lower trachea. Therefore, we inserted the lower limb of T-tube with the help of a balloon. The lower limb of the T-tube was gradually pushed forward with balloon expansion assistance and eventually passed through the collapsed tracheal successfully.
In conclusion, this is an uncommon, extreme case of complex airway stenosis. The treatment process of this patient may provide guidance for respiratory interventional physicians during the management of similar cases.
Supplemental Material
Supplemental Material, sj-docx-1-ear-10.1177_01455613211006010 - Montgomery T-Tube Insertion Under ECMO in a Patient With Complete Subglottic Stenosis and Severe Lower Tracheal Collapse
Supplemental Material, sj-docx-1-ear-10.1177_01455613211006010 for Montgomery T-Tube Insertion Under ECMO in a Patient With Complete Subglottic Stenosis and Severe Lower Tracheal Collapse by Beibei Jin, Ting Wang, Yuling Wang and Jie Zhang in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material, sj-docx-2-ear-10.1177_01455613211006010 - Montgomery T-Tube Insertion Under ECMO in a Patient With Complete Subglottic Stenosis and Severe Lower Tracheal Collapse
Supplemental Material, sj-docx-2-ear-10.1177_01455613211006010 for Montgomery T-Tube Insertion Under ECMO in a Patient With Complete Subglottic Stenosis and Severe Lower Tracheal Collapse by Beibei Jin, Ting Wang, Yuling Wang and Jie Zhang in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
B.J. and T.W. are contributed equally to this work. Ethical approval to report this case was obtained from the Institutional Review Board of Beijing Tian Tan Hospital (approval ID: KY 2020-042-02). All procedures in this study were conducted in accordance with the institutional review board of Beijing Tian Tan Hospital (approval ID: KY 2020-042-02) approved protocols. Written informed consent was obtained from the patient for her anonymized information to be published in this article.
Acknowledgments
The author would like to thank Dr. Xiaoping Wang, and members of the ECMO team of China-Japan Friendship Hospital for their assistance during the operation process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grant from Beijing Municipal Administration of Hospitals Incubating Program (PX2021022).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.