
Abstract
Prostate cancer is the third most leading cause of cancer in men in the United States. Although expected metastatic spread to bone, liver, and lymph nodes are often monitored, there are other rare presentations that can occur. This case report demonstrates a rare presentation of prostate cancer spreading to the paranasal sinuses and orbit. Not only did this case have an atypical presentation mimicking infection, the diagnosis was also only achieved through pathological evaluation after an endoscopic examination and biopsy. This case demonstrates the importance of a low threshold for endoscopic examinations in uncertain sinonasal presentations, and consistent biopsies when performing endoscopic examinations.
Introduction
Prostate cancer is the third most common cause of cancer-related death in men in the United States. 1 The usual pattern of the spread of metastatic prostate cancer is to the bone (84%), distant lymph nodes (10.6%), liver (10.2%), and thorax (9.1%), with 19.4% of these patients having metastatic spread to multiple locations. 1 There are also many noted atypical locations of prostatic spread, which include the lungs, and adrenal glands. 2 In general, solid organ metastases to the sinonasal cavities are rare and research is limited to case reports. 3 -5 There have been reports of metastatic cancer to the paranasal sinuses from the lung, 3 breast, 4 kidney, 6,7 liver, 8 and prostate. 5,9 -11
Individual case studies have reported prostate metastases to the sphenoid, 8,9 maxillary, 6 -10 and ethmoid 11 sinuses. Although prostate cancer metastases are common, metastases to the sinonasal cavities are not a frequently noted occurrence of even atypical presentations of prostate cancer. 1,2 In this article, we present a rare case of a patient with prostatic metastasis to the sphenoid sinus and mandible, which remains a rare and infrequently studied occurrence.
Case Report
A 58-year-old male with a history of adenocarcinoma of the prostate, chronic obstructive pulmonary disease, dialysis-dependent stage V chronic kidney disease, and insulin-dependent diabetes mellitus presented to our tertiary care center after an episode of presyncope with worsening confusion, left eye pain with discharge, and headaches. Most notably, the patient had locoregional recurrence of his adenocarcinoma of the prostate that was treated with adjuvant chemotherapy and was currently undergoing palliative radiation at the time of presentation. Upon initial emergency department workup, he was found to be hypotensive, hypoglycemic, and hypothermic with an elevated white blood cell count, meeting sepsis criteria.
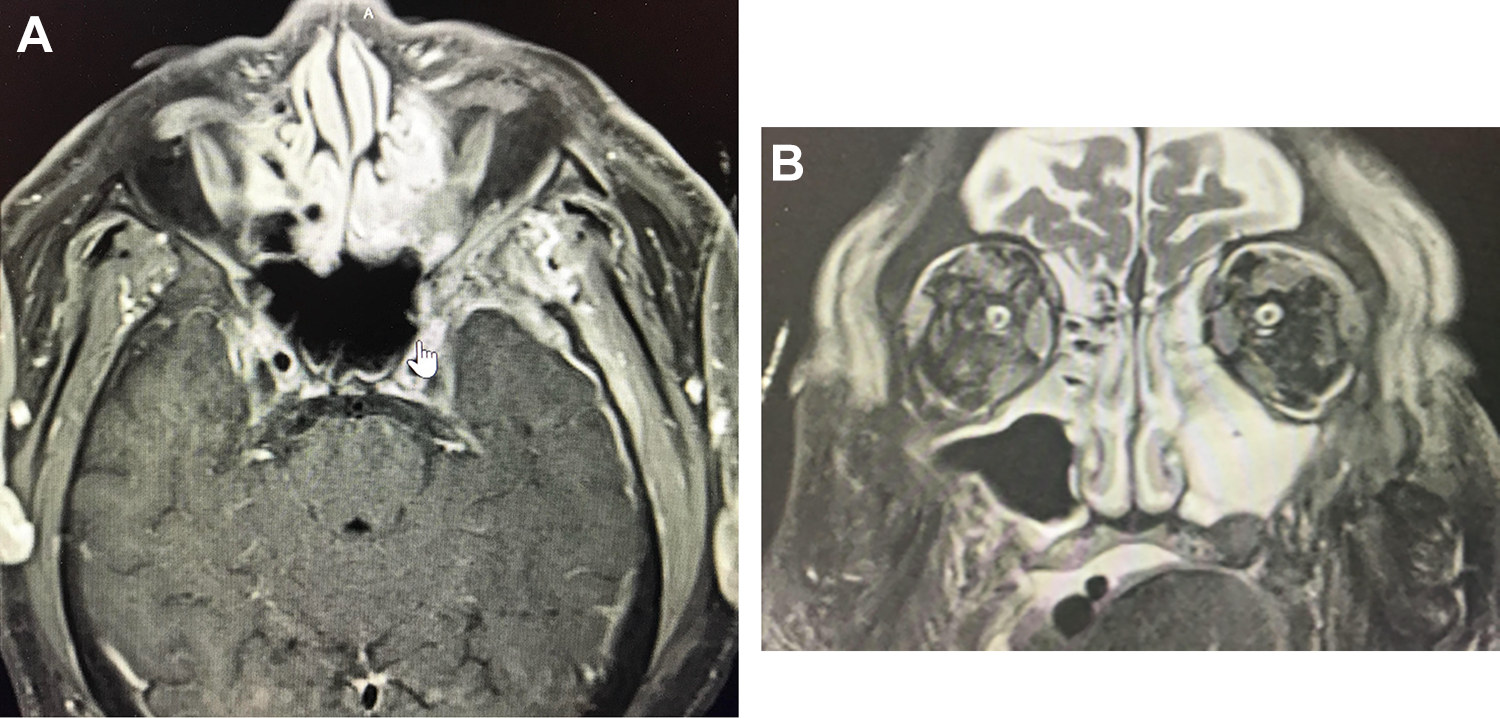
Computed tomography (CT) scan of the facial bones obtained at an outside hospital prior to transfer were suggestive of an infectious/inflammatory process with postseptal orbital and intracranial extension with osteomyelitis of the left lateral orbital wall, left sphenoid wing, squamous portion of the left temporal bone, and left superior orbital roof. Soft tissue thickening was also noted in the left ethmoid and sphenoid sinus, with demineralization of the left lamina papyracea and left sphenoid sinus wall adjacent to the orbital apex (Figure 1A). Additional findings in the head and neck included heterogeneity of the left mandibular ramus and condyle, asymmetric enlargement of the left masticator muscles, and asymmetric enlargement of the left parotid gland (Figure 1B). Chest x-ray showed a consolidative opacity in the left lung base which was also thought to be a possible etiology of the patient’s overall sepsis presentation. Interestingly, CT abdomen obtained at the outside hospital also demonstrated several new subcentimeter low attenuation lesions throughout the liver concerning for metastatic disease.

A, Computed tomography (CT) sinus, axial view demonstrating soft tissue thickening at the left lateral ethmoid and sphenoid. Sinus, with demineralization of the left lamina papyracea and left sphenoid sinus wall adjacent to the orbital apex. B, CT sinus, axial view, depicts erosion of the left mandibular ramus inner cortex, heterogeneity of the left mandibular ramus and condyle, asymmetric enlargement of the left masticator muscles, and asymmetric enlargement of the left parotid gland.
The patient was admitted to inpatient care for treatment of his pneumonia and sepsis with broad spectrum antibiotics and Otolaryngology and Ophthalmology teams were consulted. A magnetic resonance imaging (MRI) of the orbit and brain with contrast was obtained to better examine the suggested areas of intracranial extension. The MRI demonstrated an infectious/inflammatory process centered in the greater wing of the left sphenoid bone with osteomyelitis and involvement of the walls of the left orbit and left squamosal temporal bone (Figure 2A). Furthermore, the MRI also showed direct intracranial extension into the anterior left middle cranial fossa with an enhancing collection of purulent material and pathologic dural enhancement along the floor and lateral left middle cranial fossa (Figure 2B).
A, Magnetic resonance imaging (MRI) brain with contrast, axial view enhancement involving the left orbital floor and lamina papyracea, abnormal signal involving the left greater wing of the sphenoid. There is a confluent zone of enhancing material with mild restricted diffusion posterior to the orbit and lateral to the greater wing of the left sphenoid bone. Evidence of intraorbital extension where there is pathologic extraconal enhancement. Laterally, superiorly and inferiorly with fluid and slight abnormal enhancement involving the left lateral rectus muscle suggesting some myositis. B, MRI brain, coronal view extensive membrane thickening and fluid in the paranasal sinuses with opacification of the left ethmoid and maxillary sinuses. Enhancement involving the lateral orbital wall as well as the left orbital floor.
The patient was taken to the operating room by the ENT team for management of the sinuses. Left endoscopic sinus surgery with left maxillary antrostomy, left total ethmoidectomy, and sphenoidotomy was performed. Left medial orbital decompression was also performed, and tissue samples were taken for pathology and culture, including fungal culture. Interestingly, no purulence was found on endoscopic exam despite imaging highly suggestive of an infectious process.
The patient was medically managed on vancomycin and meropenem. Sinus tissue culture returned with rare and unexpected Staphylococcus epidermidis, Staphylococcus lugdunensis, and no fungal growth. Pathology results followed and showed tumor cells characterized by enlarged, hyperchromatic cells with irregular nuclear membranes infiltrating the sinuses (Figure 3A and B). These tumor cells were positive for immunohistochemical stains NKX3.1 and prostate specific antigen (PSA) (Figure 4A and B), consistent with metastatic prostate adenocarcinoma involving bone. Adenocarcinoma was found to be present as scattered individual cells and cell clusters admixed with blood and within the bone fragments. The respiratory mucosa was noted to be relatively normal appearing, without significant inflammation.
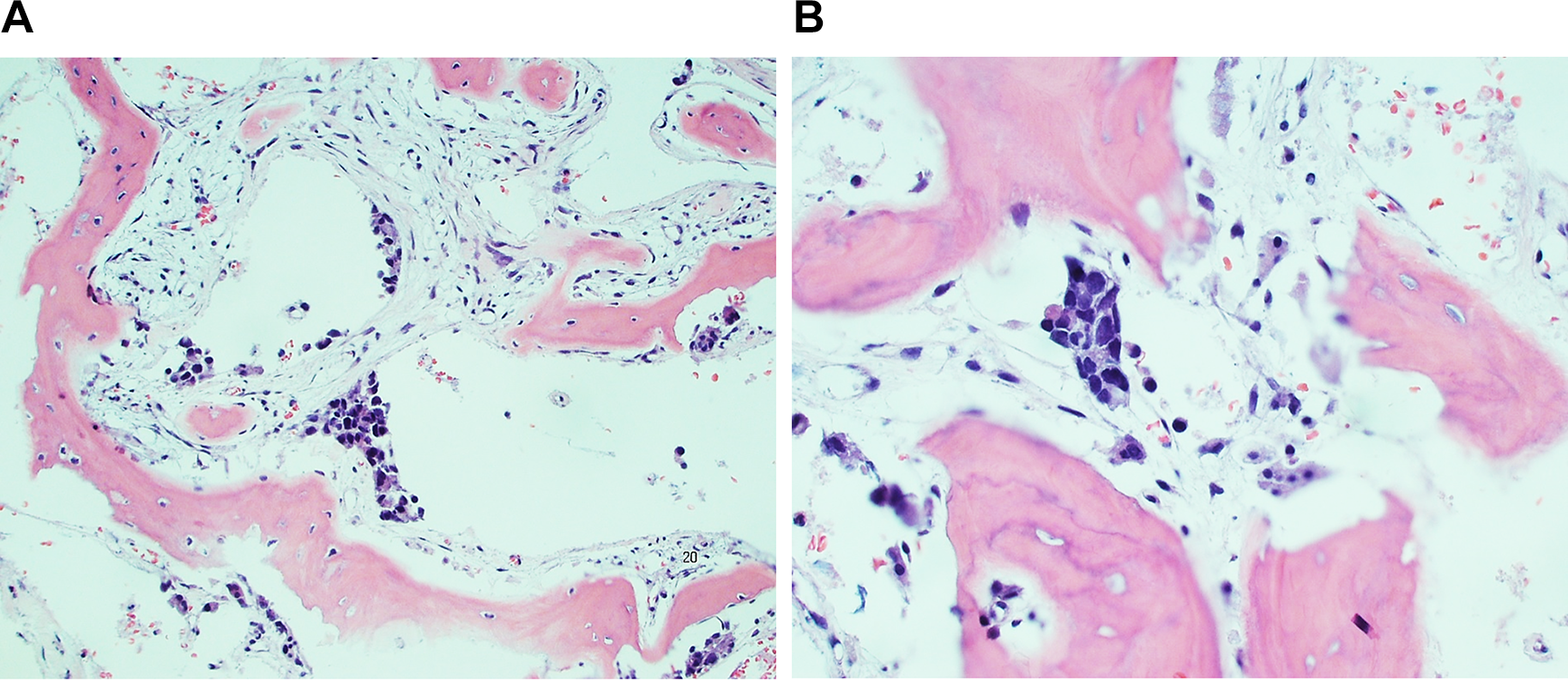
A, Histopathologic findings. A and B, Photomicrographs showing enlarged, hyperchromatic cells with irregular nuclear membranes infiltrating bone (B) Histopathologic findings (A and B) photomicrographs showing enlarged, hyperchromatic cells with irregular nuclear membranes infiltrating bone.
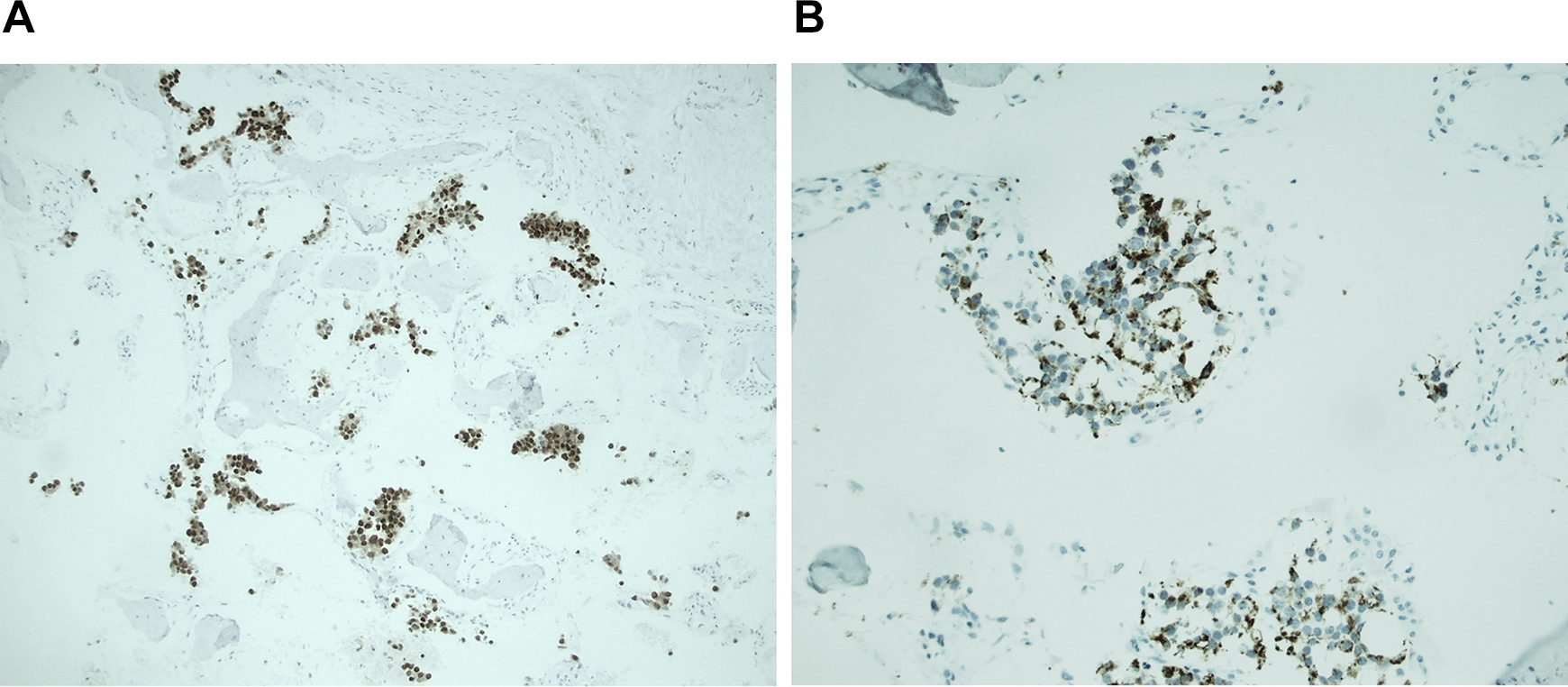
A, Immunohistochemical stains show the tumor cells are positive for NKX3.1. B, Immunohistochemical stains show the tumor cells are positive for prostate specific antigen (B).
After the return of the pathology results, along with elevated prostate-specific antigen, a radionuclide bone scintigraphy study was performed, and further supported the diagnosis of metastatic prostate cancer to the calvarium, left sphenoid, left lateral orbit, and left mandible.
Discussion
Although exceedingly rare, this case illustrates the metastasis of prostate cancer to the paranasal sinuses and orbit. Most notably, the patient presented with a case that mimicked a severe infectious process and highlights the importance of the endoscopic sinonasal examination when there is an uncertain diagnosis. Cultures should always be obtained when performing an endoscopic examination for a suspected infectious process, particularly with orbital and intracranial involvement as seen in the case above. It is also prudent to think beyond the scope of the most likely diagnosis. As shown here, the tissue sampling allowed for a pathologic evaluation that eventually led to the correct diagnosis and ultimately changed the course of the patient’s treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support forthe research, authorship, and/or publication of this article: The authors received funding for publication of this article from the “Lawrence Boies Educational Fund”, Department of Otolaryngology at Regions Hospital, St. Paul, Minnesota.