
Abstract
Differential diagnosis of globus sensation in an otherwise asymptomatic patient should include hypopharyngeal fibrovascular polyp to avoid potentially fatal complications like airway compromise following regurgitation. We present a case of a 74-year-old man with a 13-cm long hypopharyngeal fibrovascular polyp with 9 months history of globus sensation. A narrow stalk of the giant polyp allowed endoscopic removal and complete resection with the CO2 laser. Histopathological examination was conclusive for the fibrovascular polyp.
Fibrovascular polyps originating in the hypopharynx or esophagus are extremely rare, benign, submucosal lesions but can be life-threatening. Hypopharyngeal polyps are less frequent compared to esophageal.1,2 Although histologically benign, they may cause sudden asphyxia and death due to obstruction of the larynx.3,4 Symptoms are often nonspecific, leading to slow growth of the polyp which can remain unrecognized for a long period. Late diagnosis has an impact on potential operative and postoperative complications, as well as on abrupt death.
A 74-year-old man was referred to an Ear Nose, and Throat specialist in our hospital with 9 months history of an unexplained sensation of a foreign body in the throat. He had no problems with voice, breathing, or swallowing food and liquids. Flexible nasolaryngoscopy was completely normal. The patient was referred to flexible upper gastrointestinal (GI) tract endoscopy which revealed a mobile, polypoid formation in the hypopharynx. We performed direct microlaryngoscopy and hypopharyngoscopy under general anesthesia to evaluate the possibility of endoscopic removal of the polyp. Intraoperatively, a giant, pedunculated, smooth, red mass was found in the region of the hypopharynx which originated from the lower part of the anterior hypopharyngeal wall, suggesting a fibrovascular polyp (Figure 1). We concluded that the narrow stalk of the mass allowed endoscopic removal of the polyp; and it was completely removed with a CO2 laser. The length of the polyp was approximately 13 cm (Figure 2). Histopathological examination of the resected tumor revealed stratified squamous epithelium on the surface and subepithelial fibro-adipose stroma with blood vessels and was conclusive for the fibrovascular polyp (Figure 3). Follow-up of 2 years showed no evidence of recurrence and complete resolution of symptoms.

Intraoperative view of the giant fibrovascular polyp.

Giant fibrovascular polyp specimen after excision.
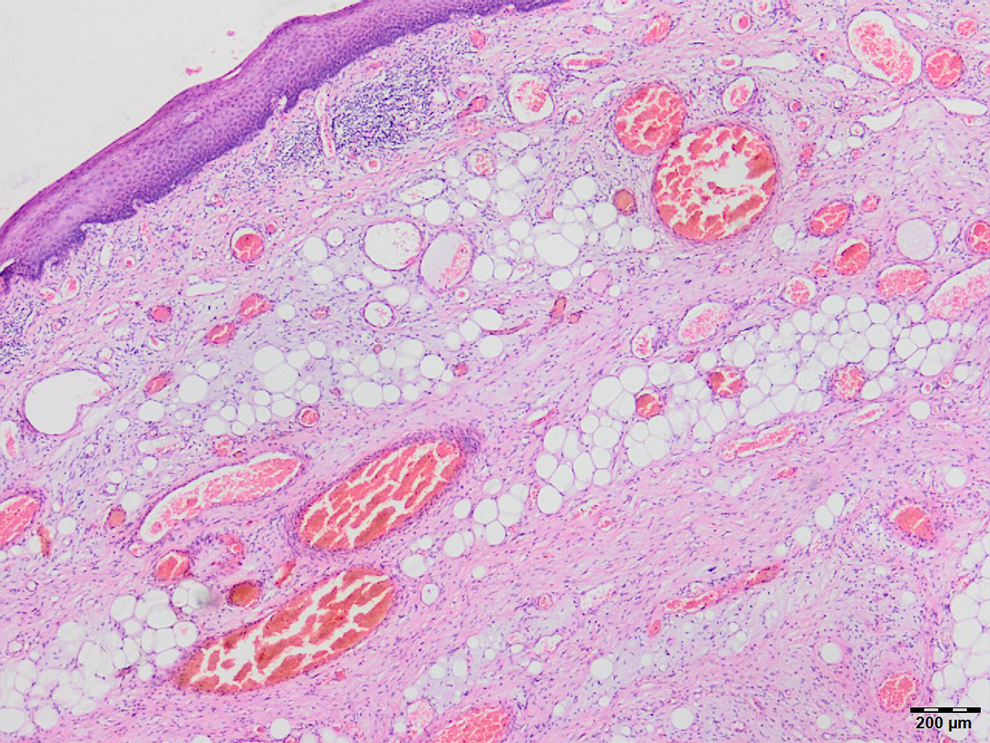
The histopathology of the fibrovascular polyp (Hematoxylin & Eosin; ×40) showing subepithelial fibro-adipose stroma of the polyp with blood vessels, and lined by squamous epithelium.
Globus pharyngeus is a common complaint in ENT practice usually caused by laryngopharyngeal reflux disease, upper aerodigestive malignancy, abnormal upper esophageal sphincter function, nonspecific esophageal motility disorder, psychological factors, stress, pharyngitis, postnasal drip, anticholinergic medication causing xerostomia, salivary hypofunction, tongue base hypertrophy, retroverted epiglottis, thyroid pathology, or supragastric belching.5,6 Due to its slow growth and nonspecific symptoms such as globus sensation, a hypopharyngeal polyp may stay unrecognized for many years.
Diagnostic evaluation of upper GI fibrovascular polyps includes barium swallow test, upper GI tract endoscopy, and direct laryngoscopy with hypopharyngoscopy. However, even on direct laryngoscopy and hypopharyngoscopy, small polyps are easy to miss due to the normal surface mucosa of the polyp. 1
Special considerations influence surgical decisions. In general, large polyps tend to be removed via a transcervical approach and lateral pharyngotomy.7,8 This approach allows adequate visualization but includes more potential postoperative morbidity and sometimes longer postoperative stay compared to endoscopic surgery. The endoscopic approach is usually more suitable for smaller lesions, and adequate visualization is a prerequisite. Transoral robotic surgery, a minimally invasive approach, should represent a valid alternative for large hypopharyngeal polyps, since that technique might provide adequate visualization in patients with lesions too large to visualize well with traditional endoscopy, potentially saving patients from an external approach. Fibrovascular polyps of the upper GI tract tend to recur; hence, endoscopic surveillance and/or barium swallow tests are recommended.
In conclusion, differential diagnosis of globus sensation should include hypopharyngeal fibrovascular polyp to avoid potentially fatal complications like airway compromise. The selection of surgical approach must be influenced by both the chance of complete surgical removal and minimal perioperative morbidity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.