
Abstract
Our case demonstrates the rare presentation of sinonasal sarcoidosis causing severe nasal obstruction. While the patient had a remote history of pulmonary sarcoidosis, she was in remission and had no prior history of sinonasal involvement. Sarcoidosis should be considered in a patient with nasal obstruction especially when there is a history of systemic sarcoid disease.
A 64-year-old African American female with a remote history of pulmonary sarcoidosis presented for evaluation of severe nasal congestion. Her pulmonary sarcoidosis was inactive and she had not required medication for several years. The patient first noticed right-sided nasal congestion and difficulty breathing 6 months earlier, unimproved with daily topical nasal steroid. On examination, there was an approximately 1 cm firm, submucosal lesion on the anterior aspect of the right nasal septum extending from the nasal cavity floor to the nasal valve and head of the inferior turbinate causing complete right-sided obstruction. The overlying mucosa was hypervascular, nonfluctuant, and nontender to palpation. There was bilateral inferior turbinate hypertrophy, greater on the left, as well. The posterior nasal septum was incompletely visualized on the right side due to the obstructing septal lesion and turbinate hypertrophy.
Given the patient’s severe nasal congestion and failure to respond to topical nasal steroids, she elected to forgo an in-office biopsy and instead pursued septoplasty and turbinate reduction with biopsy of the submucosal septal lesion (Figure 1). A right-sided submucoperichondrial flap was elevated, and once the anterior submucosal lesion was largely excised down to the intact cartilage, the remainder of the septum posterior to the lesion appeared straight and, therefore, the septoplasty was not performed. During endoscopic turbinate reduction, the left inferior turbinate submucosa appeared rubbery and friable, similar to the contralateral septal mucosa, and was biopsied as well. Submucosal turbinate reduction was performed on both inferior turbinates using a coblator turbinate wand. Intraoperative nasal endoscopy revealed otherwise normal mucosa and clear middle meatus with no edema, drainage, or other evidence of sinusitis. Tissue pathology from the right septum and left inferior turbinate revealed nonnecrotizing granulomas, consistent with sarcoidosis (Figure 2).
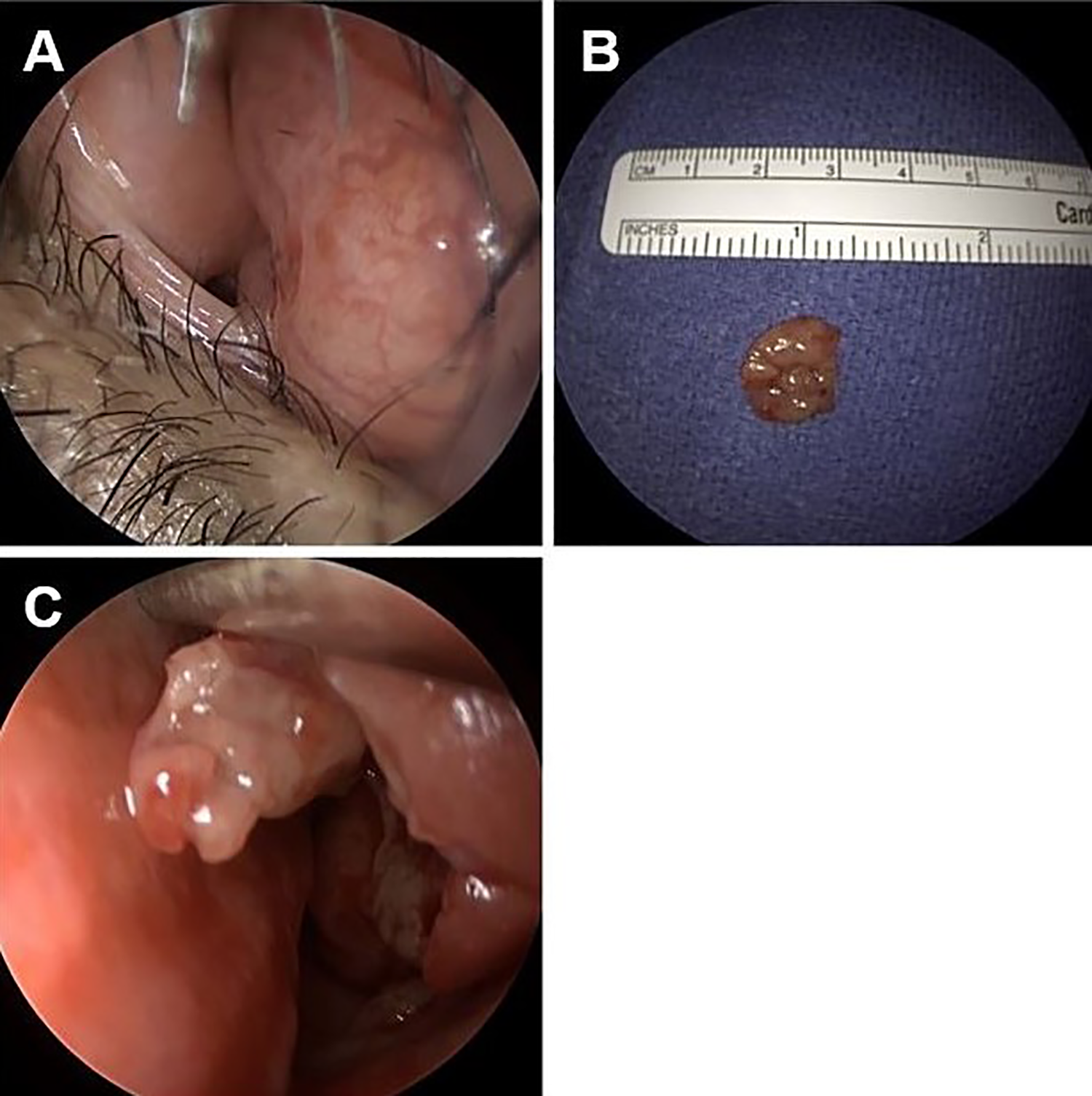
Intraoperative photographs showing a hypervascular submucosal lesion on the right anterior septum causing complete obstruction (A), a representative sample of the excised tissue (B), and appearance of the biopsied rubbery, granulomatous left inferior turbinate (C).
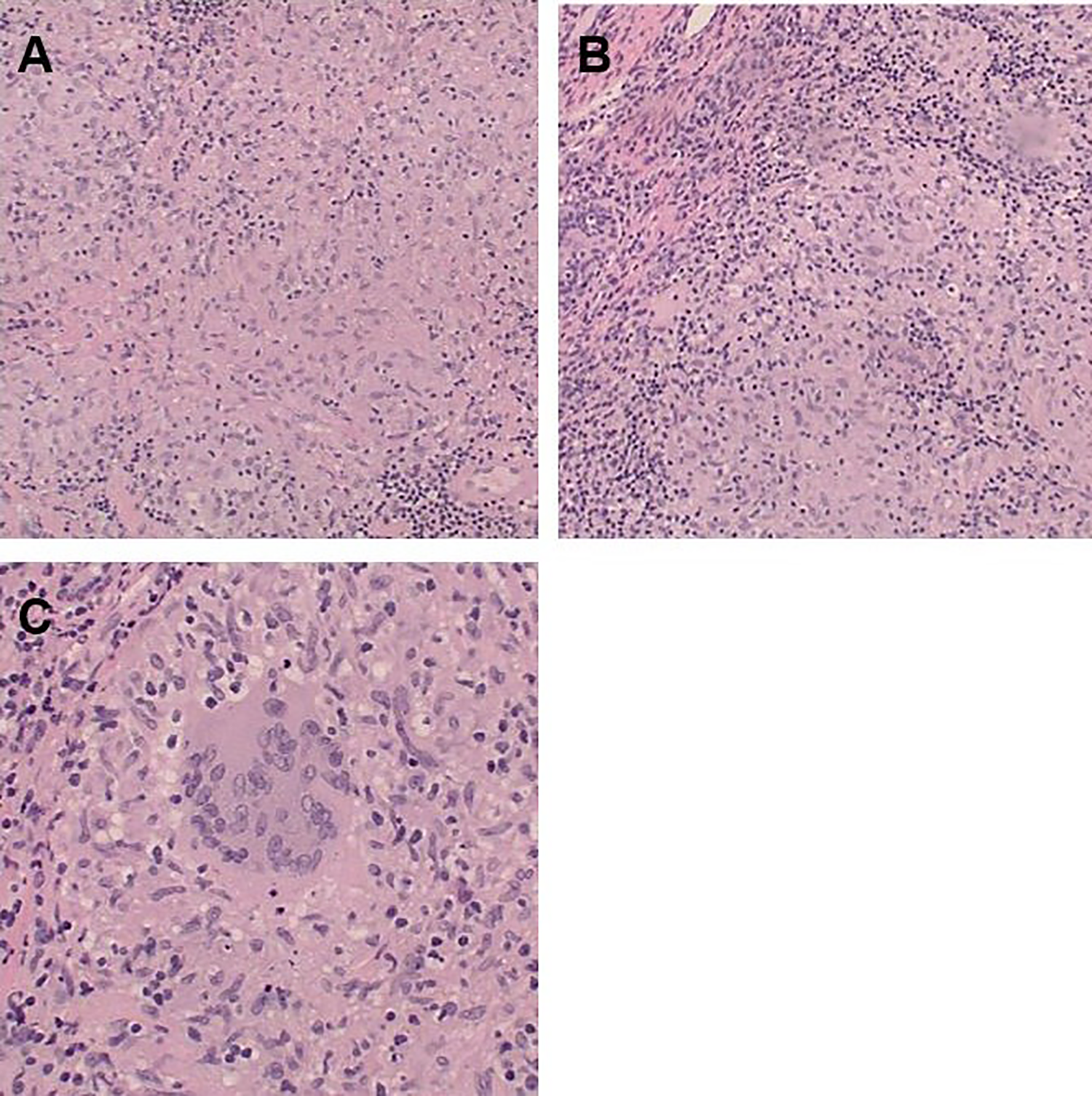
Right nasal septal biopsy showing confluent nonnecrotizing granulomata (H&E, ×100) (A, B). Right nasal septal biopsy showing granuloma, demonstrating classic multinucleated histiocyte among other mononuclear activated macrophages (H&E, ×200) (C).
Postoperatively, the patient reported significant improvement in nasal congestion. She was placed on a 4-week oral steroid taper starting at 40 mg with dramatic improvement in her intranasal edema. Six months following surgery, she has a normal nasal exam and is symptom free while remaining on prophylactic topical nasal steroids only.
Sarcoidosis is a multiorgan disease characterized by noncaseating granulomas. The most common areas involved include the lungs and mediastinum; however, patients often have involvement of the eyes, skin, liver, bone marrow, or extrapulmonary lymph nodes. 1 Only approximately 1% of patients with sarcoidosis have been reported as having sinonasal manifestations.2,3 Patients may complain of nasal obstruction, rhinorrhea, crusting, anosmia, or epistaxis; however many are asymptomatic and remain undiagnosed.3-5 Sinonasal sarcoid may also cause chronic sinusitis.3,6-8 The characteristic granulomas are most often located on the inferior turbinates and nasal septum, appearing as friable mucosa or yellow, submucosal nodules on exam, as seen in our patient. 2
While spontaneous remission of sarcoidosis is not uncommon and has been reported in up to 60% to 70% of cases, many patients require treatment.9,10 Treatment of isolated sinonasal sarcoidosis primarily consists of topical, oral, or injected intranasal steroids. 11 For patients with significant nasal obstruction, like our patient, and failure to improve on corticosteroids, nasal surgery may be considered. Surgery reduces nasal cavity obstruction and provides an opportunity for biopsy-confirmed diagnosis. Postoperatively, patients have shown increased response to topical steroids, perhaps due to lack of obstruction preventing steroid delivery. 12 Despite our patient’s remote history of sarcoidosis, this diagnosis was not on our initial radar and she was not offered systemic corticosteroids after failing topical steroid therapy and prior to offering surgery. It is certainly possible that she may have responded to systemic corticosteroid therapy.
Our patient demonstrated the unique presentation of nasal sarcoidosis causing near complete nasal obstruction after several years without symptoms or requirement of systemic steroids. In fact, she never had a history of nasal problems even when her pulmonary sarcoid was active. While the frequency of nasal involvement in patients with concurrent pulmonary sarcoidosis is well-reported, the frequency in patients with inactive disease is unknown. 10
Although most cases of nasal sarcoidosis are medically managed, the severity of this patient’s disease and obstruction warranted surgical intervention. To date, there is conflicting evidence regarding the long-term success of surgical excision. Case reports have shown recurrence of symptoms within as little as 6 months, whereas others demonstrated absence of symptoms up to 12 years following surgery.5,6,12 Otolaryngologists should have a high index of suspicion for nasal manifestations of sarcoidosis in any patient with a history of active or remote sarcoidosis even in the absence of pulmonary symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.