
Abstract
Nodular fasciitis is a rare, benign lesion characterized by the pseudosarcomatous proliferation of fibroblasts and myofibroblasts. Accurate diagnosis presents a unique challenge for otolaryngologists, as nodular fasciitis frequently mimics malignancy clinically; however, it can be distinguished from malignancy by subtle findings on pathology. A diagnosis of nodular fasciitis should be considered for any irregular or rapidly growing lesion of the head and neck area, as accurate diagnosis is particularly important to avoid overtreatment in cosmetically sensitive regions.
A 49-year-old male with no relevant medical history presented to otolaryngology clinic with a 2 × 1.5 cm mass centered on the left conchal bowl that had been growing rapidly over the previous 4 months. The lesion was noted to be irregular and firm, but nontender with no associated erythema (Figure 1). Multiple punch biopsies were performed in the office, but the pathologic findings were nondiagnostic. The patient subsequently underwent excision of the mass under general anesthesia for definitive diagnosis and management of the rapidly growing mass. At the time of excision, the perichondrium was mostly able to be preserved, although in certain portions it appeared that the lesion involved the underlying conchal cartilage, necessitating removal. Local reconstruction was performed with a full-thickness skin graft from the postauricular area.

The patient presented with an irregular, firm 2 × 1.5 cm lesion centered on the left Conchal bowl that had been growing over the past 4 months.
The lesion histologically demonstrated bland foci of spindle cells scattered within large tangles of keloid-like collagen bundles (Figure 2). The spindle cell areas had a loose tissue culture-like appearance with extravasated red cells, characteristic of nodular fasciitis. Although the histologic differential diagnosis included both nodular fasciitis and keloid, immunoperoxidase stains positive for smooth muscle actin and negative for β-catenin supported the former. At last follow-up, the patient appeared to be healing well with no evidence of local recurrence.
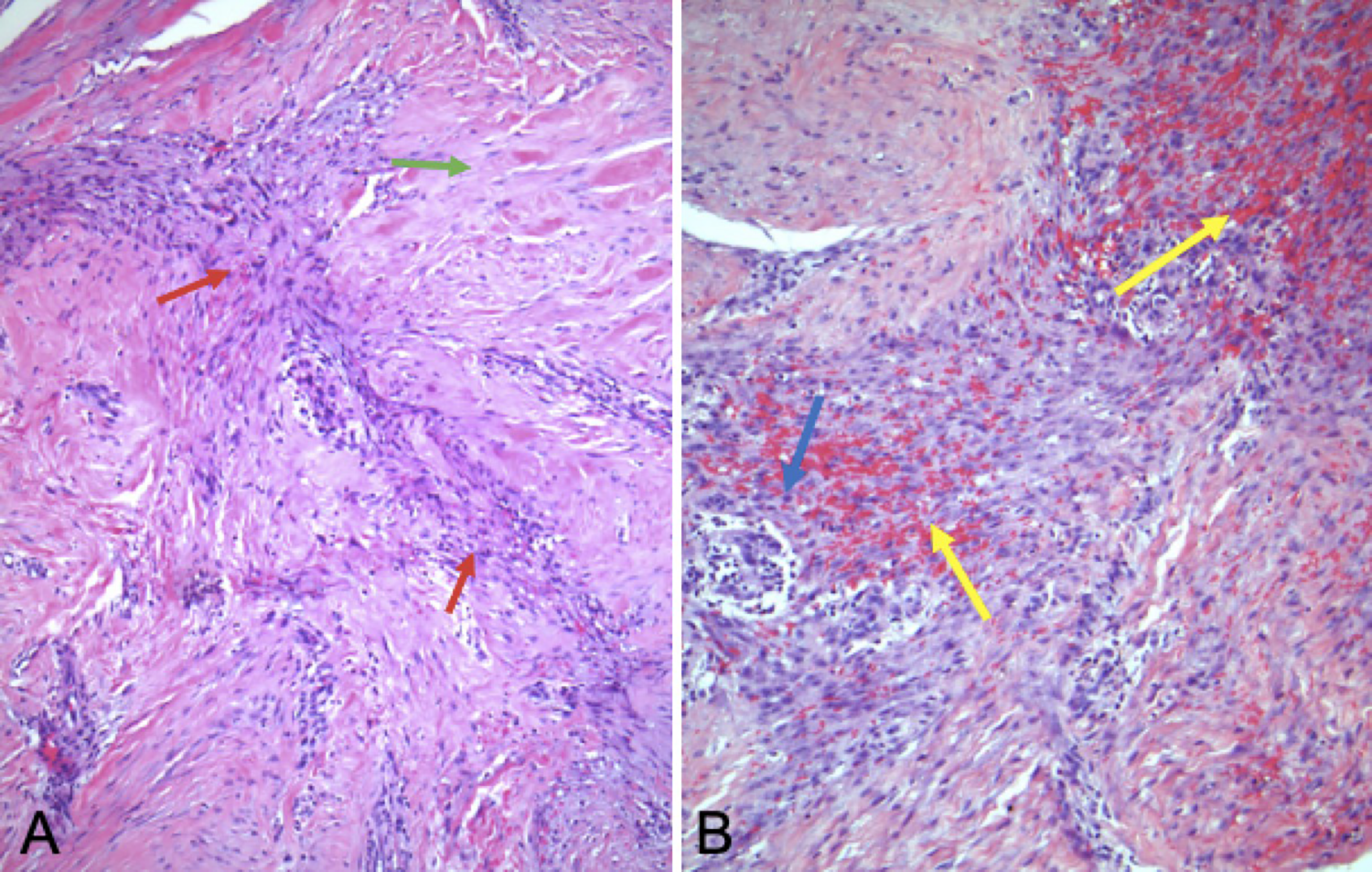
A, Histology from the lesion demonstrating foci of loosely associated spindle cells (red arrow) scattered within large tangles of collagen bundles (green arrow). B, Higher magnification image demonstrating extravasated erythrocytes and inflammatory cells (yellow arrow) against a myxoid stromal background, with stromal “tears” (blue arrow) a common finding in nodular fasciitis.
Nodular fasciitis is characterized by a benign, pseudosarcomatous proliferation of fibroblasts and myofibroblasts.1,2 These lesions tend to occur in patients between 20 and 40 years of age, and anecdotally are often associated with a site of previous trauma, although a direct mechanism for this has not been established.1,3 Lesions are generally small, but rapid growth may raise clinical concern for malignancy. On pathology, lesions are characterized by proliferative myofibroblasts with a spindle- to stellate-shaped appearance with oval nucleoli and abundant basophilic cytoplasm. These cells are usually associated with loose, myxoid stroma as well as areas of dense collagen deposition. 1 Lesions are generally well circumscribed, although limited peripheral soft tissue infiltration may be observed. Immunohistochemistry is not necessary for diagnosis, but lesions will demonstrate staining for vimentin, smooth muscle actin, muscle-specific actin, and CD68 (KP-1). 1 Recent reports have identified a potential MYH9-USP6 fusion gene that may trigger clonal neoplastic origin. 2 Treatment is generally via surgical excision, although if diagnosed definitively on FNA, expectant management for 4 to 8 weeks may lead to spontaneous regression. 4 When treated with surgical excision, recurrence rates are reported to be 1% to 2%. 5
The diagnosis of nodular fasciitis is relatively uncommon, representing approximately 0.025% of all pathologic diagnoses. 4 Although most commonly found in the extremities, these lesions can occur anywhere in the body and the head and neck region represents 7% to 20% of all cases.4,6 Although the head and neck is a relatively common location, particularly in children, involvement of the ear is less common. Reported cases of nodular fasciitis involving the external ear include a 2001 series of 50 cases of nodular fasciitis involving the external ear region by Thompson et al, and an additional series published in 2016 of 20 cases involving the external auditory canal by Ahn et al.1,2
Accurate diagnosis presents a unique challenge, as these lesions frequently mimic malignancy clinically and pathologically. Nodular fasciitis often presents as an irregular-appearing lesion, characterized by rapid growth and sometimes infiltrative of the surrounding soft tissues. On imaging, these lesions demonstrate irregular and infiltrative borders similar to sarcomas and have also been reported to be FDG-avid on positron emission tomography–computed tomography.3,4 FNA is rarely diagnostic but can demonstrate frequent mitoses, spindle cells, and low-grade atypia. 3 On pathology, these lesions have been confused with dermatofibrosarcoma protuberans, fibrosarcoma, leiomyosarcoma, malignant fibrous histiocytoma, proliferative fasciitis, inflammatory pseudotumor, fibromatosis, fibrous histiocytoma, and benign peripheral nerve sheath tumors. 1 However, nodular fasciitis can be differentiated from malignant lesions by a lack of significant nuclear atypia, hypercellularity, cellular necrosis, or atypical mitotic activity on cellular staining. 2
Although nodular fasciitis of the external ear is rare, a diagnosis of nodular fasciitis should be considered on the differential whenever one encounters an irregular or rapid-growing lesion of the head and neck area. Particularly in cosmetically sensitive regions, an accurate diagnosis is particularly important in order to avoid aggressive overresection or overtreatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.