
Abstract
This retrospective evaluation of surgical outcomes for hyomandibular suspension when performed with uvulopalatopharyngoplasty (UPPP) for the treatment of obstructive sleep apnea (OSA). Thirty-nine patients with moderate-to-severe OSA were treated with hyoid myotomy and suspension and uvulopalatopharyngoplasty. Patients underwent hyoid advancement and suspension to the mandible (Encore System) with either staged or concurrent UPPP. The primary outcome was a successful surgical result, defined as an apnea hypopnea index (AHI) lower than 20, and a 50% or greater decline in AHI on postoperative polysomnography. Successful surgical results were achieved in 30 (76.9%) out of 39 patients. The mean preoperative AHI improved 69.2% from 49.9 ± 25.6 to 15.4 ± 14.9 (P < .001) postoperatively. All patients reported clinical improvement of symptoms. There were 4 wound complications and one infection requiring removal of hardware. For patients with multilevel obstructive sleep apnea, hyoid advancement and suspension to the mandible appears efficacious when performed in conjunction with uvulopalatopharyngoplasty.
Introduction
Obstructive sleep apnea (OSA) is a chronic sleep disorder where partial or complete collapse of the upper airway occurs. 1 The prevalence of OSA associated with accompanying daytime sleepiness is approximately 3% to 7% for adult men and 2% to 5% for adult women in the general population. 2
Continuous positive airway pressure (CPAP) is considered first-line treatment for OSA. However, long-term compliance with CPAP is estimated to be only 60% and significant sequelae for untreated patients with moderate to severe sleep apnea is well documented.3-6 Symptomatic OSA patients who fail CPAP therapy are excellent candidates for an upper airway surgery treatment option.
Uvulopalatopharyngoplasty (UPPP) is the most commonly performed OSA surgery; however, UPPP alone has been shown to achieve an apnea hypopnea index (AHI) reduction of only 33%. 7 Standalone UPPP addresses only velopharyngeal airway collapse while moderate to severe OSA is widely accepted as a multilevel airway disease. Due, to its limited efficacy and longer term complication profile it is no longer the most commonly utilized technique for OSA surgery; however, it remains a widely employed modality on which we hope to elaborate further. The decreased level of efficacy when UPPP is performed alone on patients with moderate and severe OSA is not unexpected. Recent evidence reviews of OSA surgery demonstrated that the addition of less invasive hypopharyngeal procedures to UPPP improves the surgical success over UPPP alone and may achieve AHI reductions similar to those observed for the most compliant CPAP users, as reported by Stück et al.8-10
For multilevel airway surgery, the experience of the authors has been that hyomandibular advancement, when added to modified UPPP, is efficacious, easy to perform. Most published hyoid suspension results are confounded by varying technique approaches (hyomandibular vs hyothyroid suspension) and by concomitant tongue base procedures (genioglossal advancement). It has been speculated that hyomandibular suspension has a higher success rate for treating OSA than hyothyroid suspension procedures, particularly in the female population. 11 Outside of a recent study by Gillespie et al, 12 there are no published studies that investigate the safety and efficacy of only hyoid suspension to the mandible with UPPP in the treatment of OSA. Thus, the additive efficacy of combining standalone hyomandibular suspension to UPPP is not well documented.
This study presents the outcomes of a consecutive series of patients who met inclusion criteria treated with hyomandibular suspension using a system with proprietary bone anchors that allow adjustment of the advancement and suspension of the hyoid bone to the mandible (EncoreTM; Siesta Medical). This study’s primary aim is to retrospectively evaluate the surgical success rate, impact on sleep apnea severity, and complications of a less invasive approach to multilevel upper airway surgery where a tissue-sparing modified UPPP is performed along with hyomandibular suspension.
Materials and Methods
Study Design
A multicenter, retrospective chart review of all patients with moderate-to-severe OSA undergoing multilevel hyomandibular and modified UPPP airway surgery was performed. All adult patients (age > 18 years) who underwent hyoid suspension to the mandible using the EncoreTM System (Siesta Medical) with either previous or concomitant UPPP, who had a baseline AHI of 15 or greater, and had a follow-up polysomnography (PSG) or home sleep study (HSS) performed were included in analysis. The EncoreTM System (Siesta Medical) is a widely available surgical platform in the United States with a comparable cost profile to similar products. Data acquired included patient demographics, pre- and post-procedural AHI, and adverse events.
The primary outcome measure was a successful surgical result, 13 defined as a final AHI lower than 20 with a 50% or greater decline in AHI on the postoperative sleep study. An institutional review board exemption was obtained for each institution in this multicenter, retrospective chart review study.
Patient Selection
All patients initially presented with a diagnosis of moderate-to-severe OSA and CPAP failure or intolerance. Patients received a comprehensive airway examination including flexible nasopharyngolaryngoscopy. Patients were selected based on in-office endoscopy findings consistent with hypopharyngeal obstruction. Specific findings included a narrow retroglossal airway, lateral hypopharyngeal wall collapse on Mueller maneuver, and/or contact of the epiglottis to the posterior pharyngeal wall. Finally, larger Friedman tongue positions (III/IV) and smaller or absent tonsils (0-1+) were included as indications for hyomandibular suspension.
Surgical Procedure
Patients who had not had a previous UPPP underwent combined modified UPPP and hyomandibular suspension at the time of surgery. Patients who had previously received a UPPP underwent hyomandibular suspension alone. All baseline PSG or HSS results recorded prior to the initial UPPP procedure.
The modified UPPP technique performed focused on providing muscular support and sparing tissue (Figure 1A-D). First, the tonsils are removed. The tonsillar fossa are then closed with suture running through the posterior and anterior pillars and out to the anterior and lateral palatal musculature. The uvula is trimmed conservatively, leaving a remnant of at least 5 mm. The postoperative result has the soft palate lifted off the posterior wall of the pharynx, improved soft palate tension, and stability with the uvula biased anteriorly.
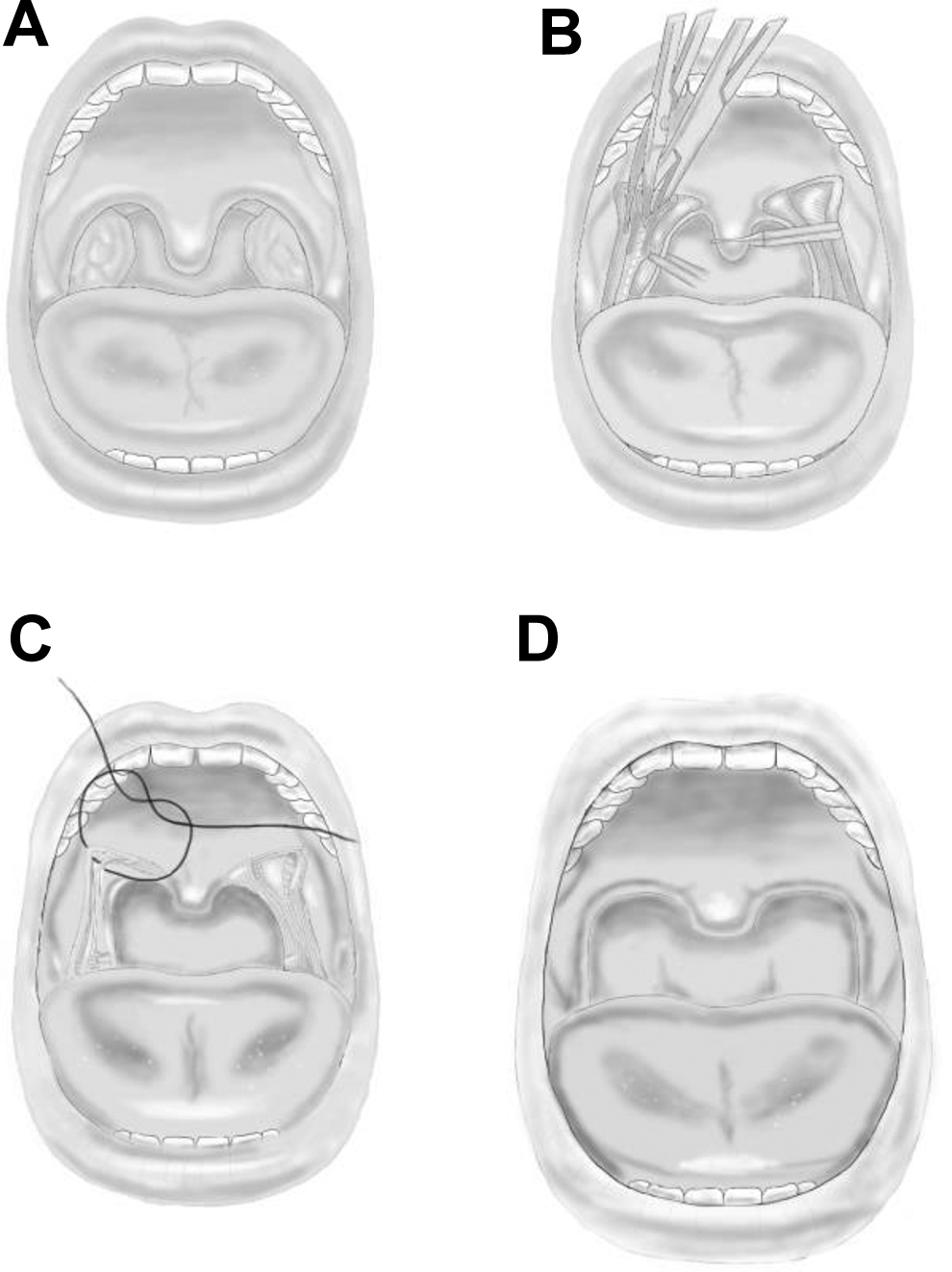
Modified UPPP technique: (A) preoperative, (B) tonsils removed and engaging pillars along with uvula trim, (C) closure and lateralization stiches, (D) postoperative. UPPP indicate uvulopalatopharyngoplasty.
The hyomandibular suspension technique described below has previously been described by Gillespie et al 12 and was performed in a similar stepwise fashion to ensure consistency across the performing surgeons (Figure 2). It was performed using either a single submental incision or 2 incisions, 1 submental, and the other anterior to the hyoid bone. The single incision technique was similar to the “minimally-invasive” technique of Gillespie. 12 For the single incision technique, a 2- to 3-cm submental incision was used to narrowly dissect to the hyoid bone. Minimal midline muscular release from the inferior attachments to the hyoid bone was made during the dissection. The hyoid bone was then grasped with an Allis clamp or tracheostomy hook and pulled anteriorly to provide improved access to the hyoid bones posterior surface. A curved helical needle (Revolution™ Suture Passer, Siesta Medical) was passed around the hyoid bone and used to place 2 suspension sutures around the body of the hyoid bone. The suspension sutures were then secured to hyoid bone with a girth hitch. Bone anchors were screwed into 1.5 mm diameter pilot holes drilled bilaterally approximately 5 mm from the midline of the mandible just within the inferior, posterior border. The hyoid suspension sutures were then threaded through the eyelets of the bone anchors, tensioned to anteriorly displace the hyoid bone 1 to 2 cm, typically to the point where the musculature attached to the hyoid began to provide significantly increased resistance to movement, and then locked in place using the internal locking screw on the bone anchors. The 2-incision approach was similar except instead of a narrow dissection to the hyoid bone, a second incision anterior to the hyoid bone was used to dissect to the hyoid bone. Suspension sutures were tunneled in a subplatysmal plane to the submental incision and then threaded into the bone anchors. The 2-incision approach simplifies hyoid bone access and suture passing and minimizes the amount of dissection necessary. Before closing, the incision(s) were generously irrigated with a saline and anti-biotic solution. No postoperative drains were placed.

Diagrammatic and written outline of the surgical technique outlined above for hyomandibular suspension. (Adapted from Siesta Medical.)
Follow-Up
Routine follow-up in the postoperative period to monitor surgical healing and manage any complications was performed. Polysomnography or a HSS was performed 3 to 9 months after surgery.
Statistical Methods
All data were collected and analyzed using Microsoft Excel software (Microsoft, Inc.). Categorical variables are presented as frequencies and percentages (%), with continuous variables presented as mean ± standard deviation values. Pre- and posttreatment outcome measures were analyzed using paired Student t test for continuous variables. A P value of less than .05 was considered indicative of statistical significance.
Results
Thirty-nine consecutive patients (27 males and 12 females) with moderate-to-severe OSA with an average age of 57 ± 11.9 years underwent concurrent or prior UPPP and adjustable hyomandibular suspension with the EncoreTM System (Siesta Medical). Eighty-two percent of treated patients had severe sleep apnea and most had a significant level of obesity (Table 1). PSG or HSS follow-up evaluations were performed an average of (7.0 ± 8.1) months after hyoid suspension.
Baseline Patient Demographics.
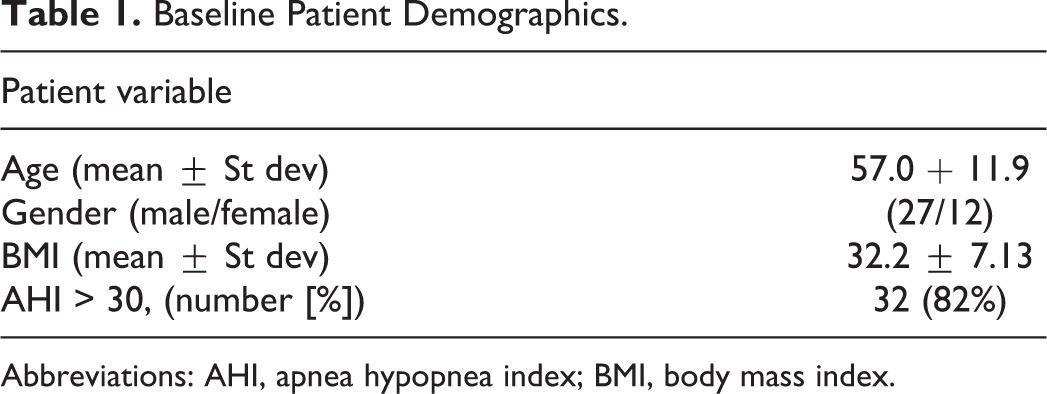
Abbreviations: AHI, apnea hypopnea index; BMI, body mass index.
The individual outcomes from this study are detailed in Tables 2 and 3, and further illustrated as a reduction in pre- and post-procedural AHI in Figure 3. A successful surgical result was achieved in 30 (76.9%) patients with the median AHI reduced from 42.0 to 10.8. The mean AHI improved significantly postoperatively by 69.2% (49.9 ± 25.6 to 15.4 ± 14.9) across all patients. Twenty nine (74.4%) of the patients achieved a final AHI of less than 15.0, with 17 (43.6%) patients experiencing a final AHI of less than 10.0. Figure 4 compares % AHI reduction with patient BMI, and demonstrates a lack of correlation between the 2 factors with a correlation coefficient of 0.0235.
Surgical Outcomes by Patient.
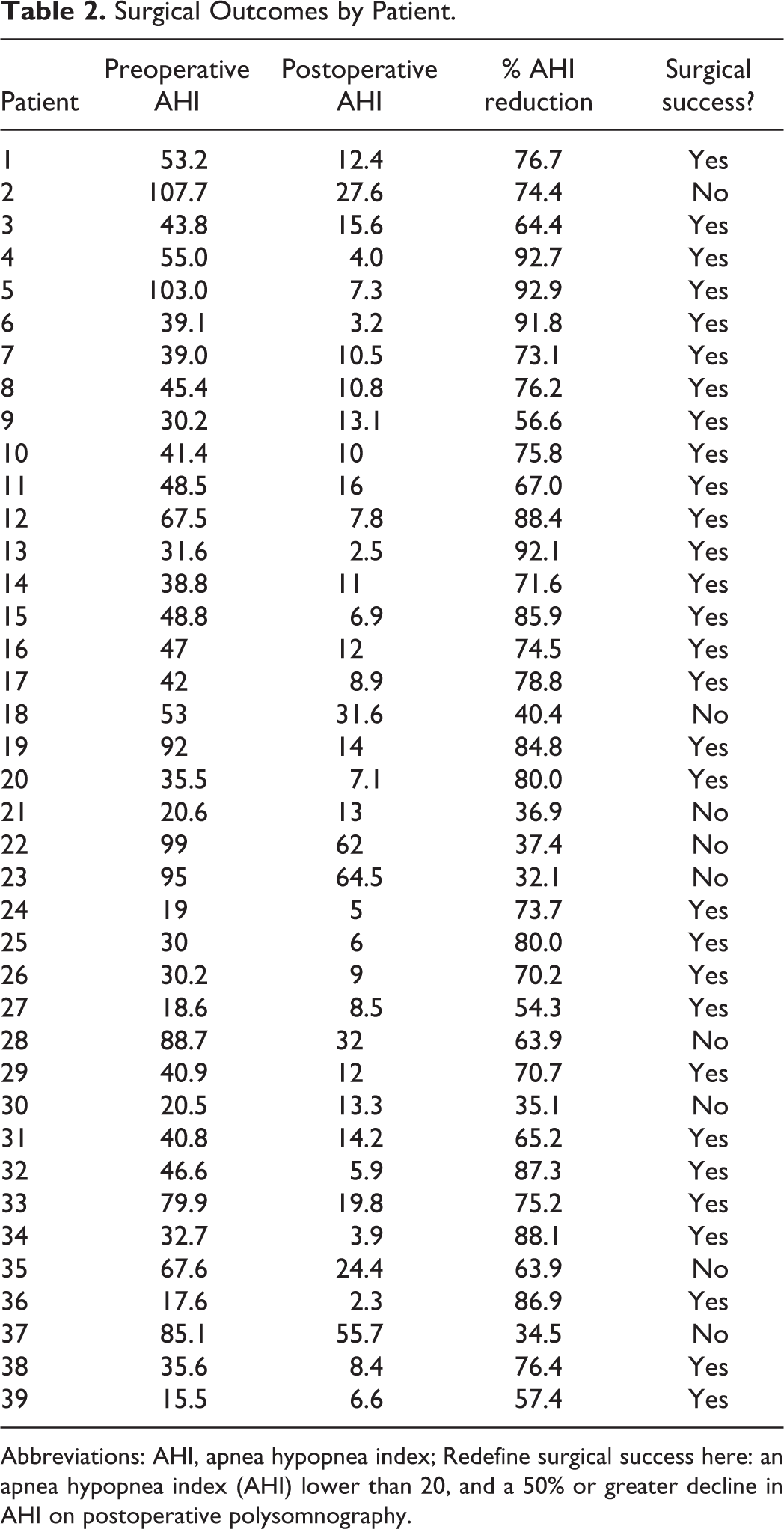
Abbreviations: AHI, apnea hypopnea index; Redefine surgical success here: an apnea hypopnea index (AHI) lower than 20, and a 50% or greater decline in AHI on postoperative polysomnography.
Pre- and Postoperative AHI Results Resulting From Hyomandibular Suspension With UPPP.a
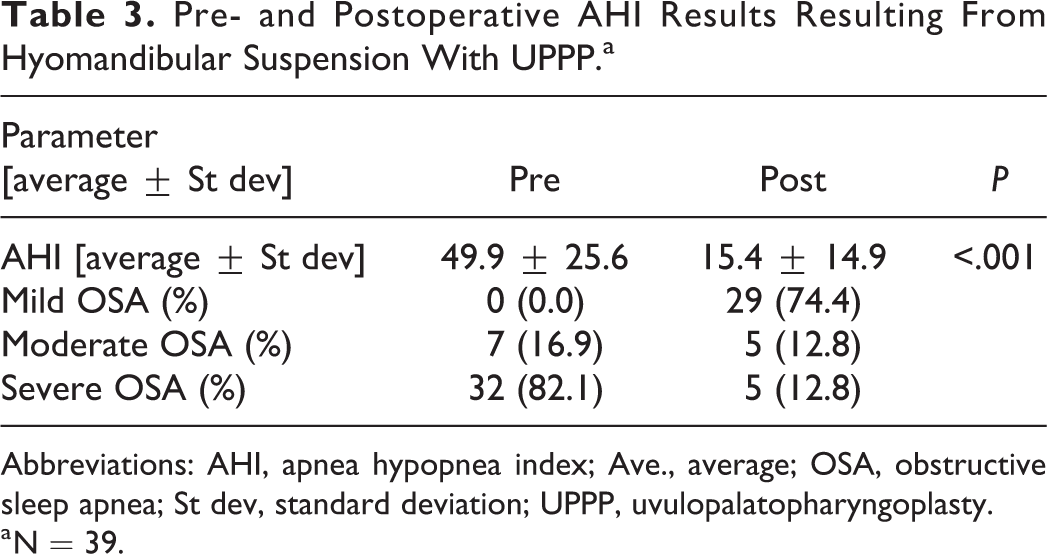
Abbreviations: AHI, apnea hypopnea index; Ave., average; OSA, obstructive sleep apnea; St dev, standard deviation; UPPP, uvulopalatopharyngoplasty.
a N = 39.
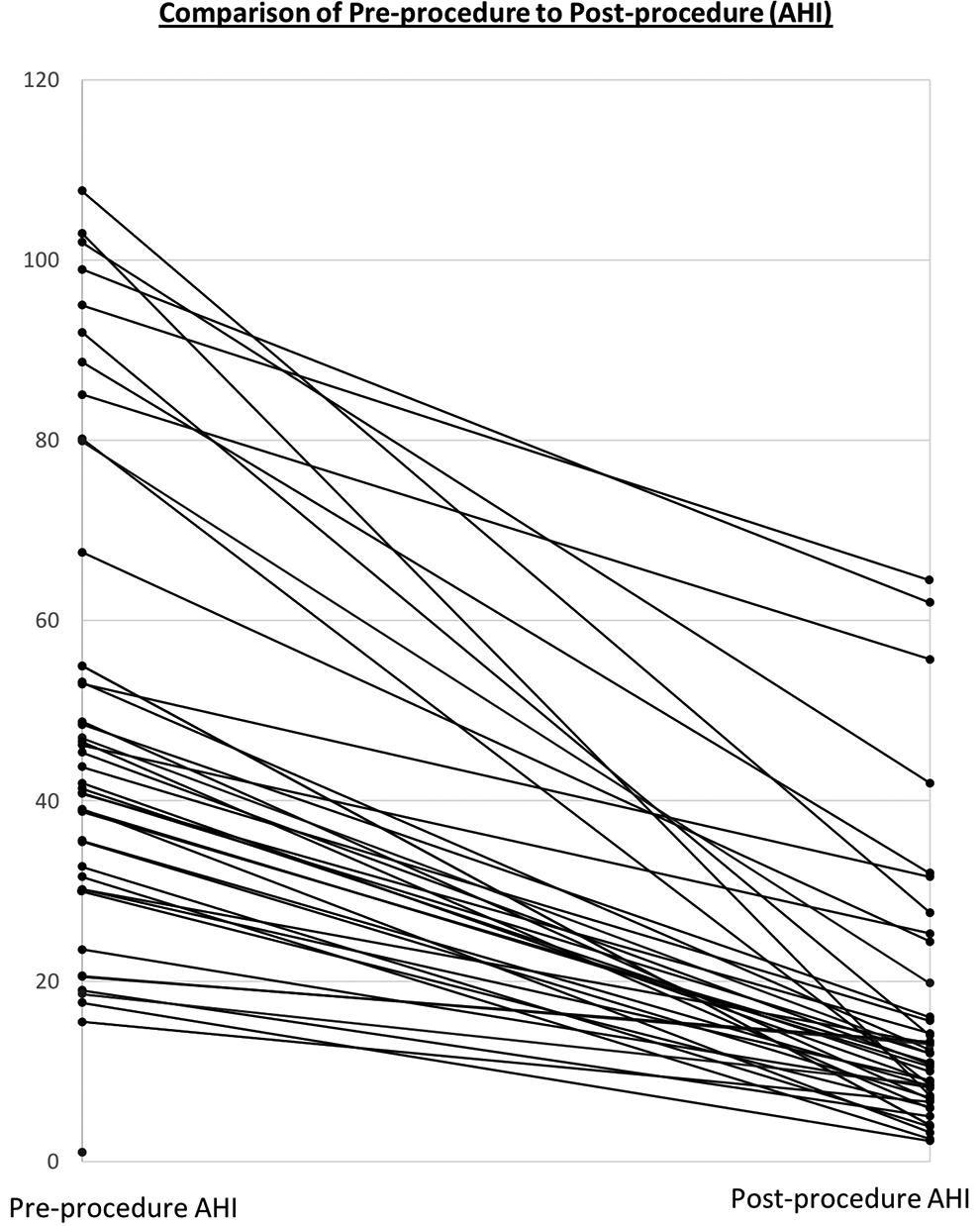
Individual preoperative and postoperative AHI outcomes (AHI = apnea hypopnea index, events/hour).
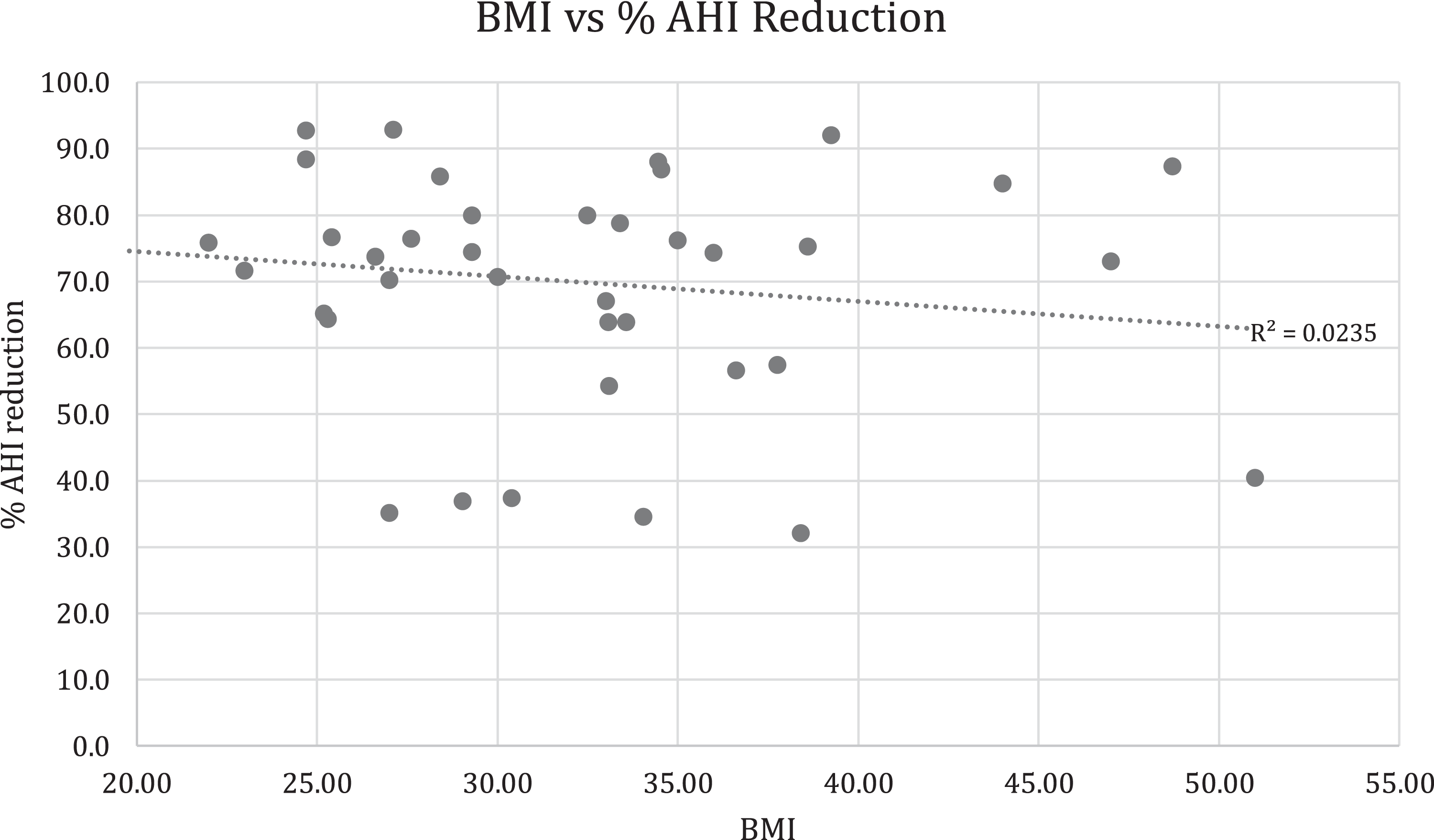
Graphical comparison of %AHI reduction as compared to individual BMI.
Five patients experienced procedure-related complications. These included a tonsillar bleed (N = 1), UPPP related case of bleeding managed with cautery (N = 1), submental seromas at the submental incision site that were managed by aspiration (N = 2), and an infection requiring removal of the implanted hyoid suspension system (N = 1). In the patient requiring removal of the suspension system, no additional peri-procedural complications were experienced; however, recurrence of the patient’s preoperative sleep apnea occurred. The patient did not wish to undergo additional surgery and resumed use of CPAP. Anecdotally, we did not observe complications related to cosmesis or changes in swallow function; however, these end points were not directly collected in the study.
Discussion
Untreated sleep apnea, specifically untreated severe OSA, has been demonstrated to significantly increase mortality risk.4,6 While various surgical options exist, even limited sleep surgery (eg, UPPP) has been shown to improve these outcomes as-well-as or better than CPAP. 14
While UPPP with tonsillectomy has become established as a commonly employed treatment model for resolving airway obstructions in the velopharynx and oropharynx, a wide variety of interventions targeting the hypopharynx exist. These interventions range from highly invasive operative-based procedures (maxillomandibular advancement) to minimally invasive office-based procedures (radio frequency ablation) to newly developed interventions with more limited indications (hypoglossal nerve stimulation). Despite advances in surgical techniques and technologies, none of these interventions are performed with the regularity of UPPP at this time. 15 As hypopharyngeal obstruction is present in up to 96% of moderate and severe sleep apnea sufferers, 16 this clearly represents an undertreated etiology of upper airway obstruction.
This case series describes a protocol of upper airway surgery that is effective in treating multiple levels of airway collapse in obese patients with moderate-to-severe OSA. Success was noted to be achievable without need for a separate sleep endoscopy based on visual evidence of multilevel upper airway narrowing including in the hypopharynx. Previous studies have shown that sleep endoscopy is most effective in assessing therapeutic response to implanted upper airway stimulation for OSA, but similar efficacy for sleep endoscopy has not been shown across other treatment modalities. 17 The treatment effect on AHI demonstrated in this study is comparable to the most robust OSA treatment options.8,9 Achieving this level of disease severity reduction with multilevel airway surgery in patients who are noncompliant on CPAP is important as compliant CPAP use normalizes the risk of traffic and work accidents, normalizes mortality in severe OSA, reduces the risk of cardiovascular incidents, and improves symptoms of OSA.18,19 This level of success may be due to the greater advancement of the hyoid bone achievable when suspending to the mandible as compared to the thyroid. Genta et al found that lower hyoid position correlates with lower pharyngeal critical closing pressure. From this perspective, the hyomandibular suspension advancement vector is consistent with what one would expect to improve the resistance to pharyngeal collapsibility. 20 In addition, hyomandibular suspension does not restrict the superior mobility of the hyoid bone required for normal swallowing. While a total of 9 patients failed to experience a surgically successful result (eg, AHI < 20 and a 50% or greater decline in AHI on the postoperative PSG), this group continued to demonstrate a meaningful 49% improvement in their average postoperative AHI (from 70.8 down to 36), indicating an ability to achieve worthwhile AHI reductions via surgical management in these individuals. Nonresponders were noted to have a higher baseline AHI but could not be separated based on age or BMI (Table 4).
Surgical Success Comparison.
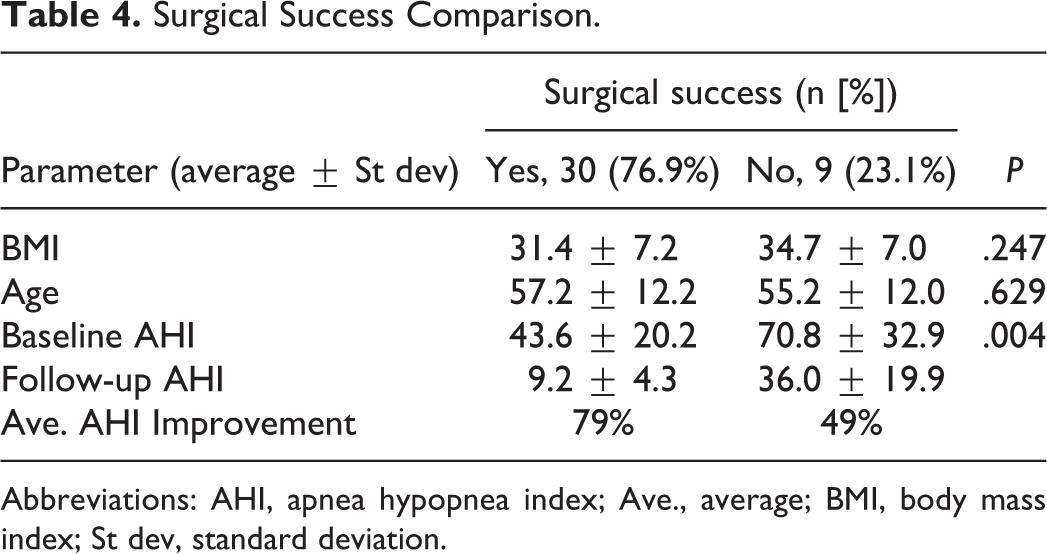
Abbreviations: AHI, apnea hypopnea index; Ave., average; BMI, body mass index; St dev, standard deviation.
There are several advantages of this simplified multilevel surgical approach. First, standard office-based methods for airway evaluation are all that are required in selecting appropriate patients for surgery. Drug induced sleep endoscopy (DISE), used to rule out circumferential collapse of the retro-palatal airway for hypoglossal nerve stimulator placement, is not required. Secondly, hyomandibular suspension combined with modified UPPP does not have the indication limitations that accompany other approaches such as HNS, specifically BMI (<32) and AHI (15-65) limitations. Thirdly, the techniques used for UPPP by the authors in this study minimize long-term consequences characteristic of this surgery. In most study patients the uvula was spared, and no insufficiency was experienced. Cosmetically, patients treated with these methods have a “normal” appearing palate and the single or double external surgical incision can readily be hidden beneath the submental crease.
The hyomandibular suspension technique and system utilized within the current study is associated with several procedural advantages. A significant advantage is the ability to directly appreciate the hyoid suspension suture tension when advancing the hyoid, thus allowing the surgeon to easily set the desired tension and adjust it intraoperatively as needed. In addition, the use of independent suspension lines provides the ability to individually adjust suspension suture tension to ensure balanced tension. Suspension suture tension and the degree of hyoid advancement remain adjustable over the long term, although this was not necessary within our cohort. The implant features that provided for adjustability also allow for uncomplicated system removal as demonstrated by the single patient with an unresolved infection. As opposed to hyothyroid suspension, hyomandibular suspension allows for hyoid excursion during swallowing and this may explain the absence of postoperative dysphagia.
Finally, the helical needle utilized in most patients dramatically improves the efficiency and predictability of passing sutures around the hyoid bone and allows for greater preservation of its muscular attachments.
Gillespie et al reported an average 54.5% AHI reduction for patients who underwent hyomandibular suspension combined with a UPPP. 12 The current study builds on these results with an average AHI reduction of 69.2%. Hyoid musculature remains almost completely undisrupted with this technique, thus maximizing airway stabilization when the hyoid is advanced. This study addresses 2 important sources of potential variability for the effectiveness of hyoid suspension—the relatively limited and variable degree of hyoid advancement achievable with hyothyroid suspension versus the more consistent advancement achievable with hyomandibular suspension, and the ability to reliably titrate the degree of hyoid advancement and suspension perioperatively. To take advantage of this capability, 2 of the authors utilized perioperative endoscopic evaluations to optimize the degree of hyoid advancement. Figure 5A demonstrates the perioperative effect of hyomandibular suspension on the airway in an awake patient while Figure 5B demonstrates similar effects in a sedated patient. There is a marked increase in airway size as the tongue and epiglottis are displaced anteriorly and the lateral hypopharyngeal walls are lateralized. These airway changes for hyomandibular suspension appear to be more significant than what has been reported previously for hyothyroid suspension. In contrast to the findings in the current study, Stuck et al reported that there were no detectable relevant changes in the upper airway anatomy as a result of isolated hyothyroid suspension as evaluated by MRI postoperatively. 21
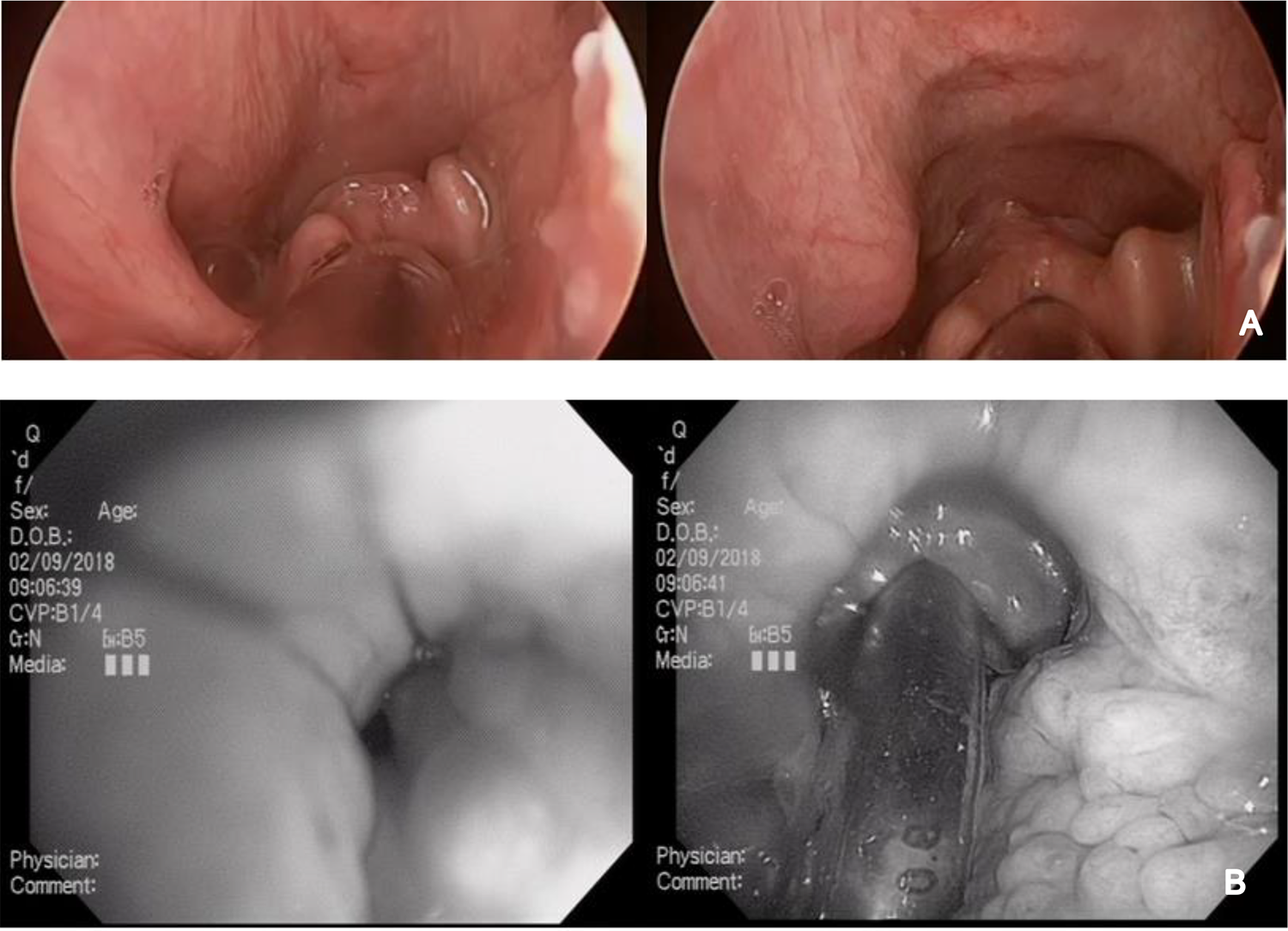
A, Perioperative effect of hyomandibular advancement on airway patency. Before advancement (left) and after advancement (right). B, Intubated and sedated view of airway patency before advancement and after advancement which demonstrates a significant enlargement of airway patency with hyoid suspension.
Patients were considered candidates for hyomandibular suspension if they had evidence of hypopharyngeal narrowing upon office-based examination. In addition, a flat-shaped epiglottis configuration was noted on fiberoptic laryngoscopy in many of the patients treated. This anatomic variant as a likely predictor for hypopharyngeal obstruction may warrant further investigation and the development of a grading system should it prove to be significant.
Results from this study are consistent with methods previously described for reporting on sleep apnea surgical studies. 22 The short duration of this study made an analysis of the change in baseline attributes unnecessary. In addition, no examination of the baseline characteristics correlation to outcomes was performed. This study is limited by the restrictions inherent to a retrospective, nonrandomized study including an inability to compare across additional surgical techniques or collect additional perioperative end points. The addition of patients with previous UPPP that solely underwent hyomandibular suspension may also introduce a level of bias in the results; however, this is felt to be limited as the technique was well established and surgical team was uniform throughout the study. Furthermore, the authors were unable to provide a measure of the relative therapeutic contributions of the modified UPPP versus the hyomandibular suspension intervention on overall outcomes; however, it may reasonably be concluded that the individual contributing effects of these surgeries on outcomes is similar to those previously reported in the literature. 23 Additionally, another inherent shortcoming of our study was a lack of comparative data including Expansion Pharyngoplasty (ESP). The paradigm has shifted in recent years from utilization of UPPP to ESP in treatment algorithms; however, we felt this data still proved critical as UPPP is still a very commonly employed treatment modality and future studies would aim to include this data. Future series may evaluate the relative impact of UPPP versus hyomandibular suspension on this patient population as the adjustability of the system would allow a hyoid suspension to be implanted and later advanced as initial follow-up data are collected. While we didn’t collect long-term complications end points in the current study, future studies would also aim to monitor the safety profile longitudinally and report such results comprehensively.
Conclusion
Adjustable hyomandibular suspension is an effective treatment when combined with modified UPPP to treat moderate-to-severe OSA in patients with clinical evidence of a hypopharyngeal narrowing.
Footnotes
Authors’ Note
Level of Evidence: 4.
Acknowledgments
Siesta Medical, Inc. provided funding for institutional review board review of the study protocol.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Jason Van Tassel, Ryan Nord, Michael R. Abidin, Dustin Platter: Siesta Medical.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Siesta Medical provided funding for IRB review of the study protocol.