
Abstract
Schwannomas are neurogenic benign tumors originating from the myelin sheath of peripheral nerves, and hypoglossal Schwannomas account for 5% of nonvestibular ones. Extracranial localizations are substantially rare, especially those affecting exclusively the parapharyngeal space; for this reason, the retrostyloid neoformations could initially masquerade as a carotid tumor or deep organized neck abscess. The purpose of this report is to highlight the importance of a multidisciplinary approach in the correct management of differential diagnosis.
Schwannomas are neurogenic benign tumors originating from the myelin sheath of peripheral nerves. It is estimated that almost 25% to 45% of these neoplasms are located in the head and neck region, 1 and hypoglossal Schwannomas account for 5% of nonvestibular ones. 2 Kaye et al proposed a classification system based on the location of the Schwannoma as intracranial (type A), intracranial/extracranial (type B), or extracranial (type C) 3 ; moreover, Nonaka et al proposed a new grading system by differentiating type C into 2 subcategories: the extracranial tumors with or without osseous involvement (type C and D, respectively). 4 Regardless of the various classifications, extracranial localizations are substantially rare, especially those affecting exclusively the parapharyngeal space,5,6 and should be considered in the differential diagnosis of parapharyngeal or neck masses to avoid overtreatment or diagnostic delays.
We report the case of a 41-year-old woman with a 2-month history of right neck painful swelling and progressive dysphagia to solid foods. Due to sudden worsening of symptoms associated with fever, the patient went to the emergency department where she was immediately prescribed blood tests. It was revealed a tough and poorly moveable cervical mass with medialization of the right anterior tonsillar pillar associated with right lateral deviation of the tongue during the protrusion (Figure 1A). Considering the increase in leukocytes, predominantly neutrophils, she was referred for a contrast-enhanced computed tomography scan (Figure 1B) suspecting a peritonsillar abscess. Then, after otolaryngological consultation and correlating the inflammatory state to the recent dental procedure reported by the patient, a contrast-enhanced magnetic resonance imaging (MRI) has been prescribed (Figure 1C and D). The examination showed a space-occupying lesion (3 cm × 4.5 cm × 2.5 cm approximately) with a “salt and pepper” pattern (more evident in T2-weighted sequences) located between the right carotid and parapharyngeal space, just above the bifurcation of the common carotid and extending cranially up to below the petrous rock, posteriorly to the mandible in the retrostyloid area; these images could have been misleading, giving the impression of a common carotid body tumor, the most frequently identified paraganglioma in the head and neck. 7 Due to the nature of the lesion and its location, a team of otolaryngologists, vascular surgeons, and maxillofacial surgeons was convened in order to plan the best therapeutic process for the patient. A magnetic resonance angiography should have been performed but, taking into account the worsening of symptoms, it was preferred to intervene surgically ensuring the presence of the vascular surgeon in the operating room.
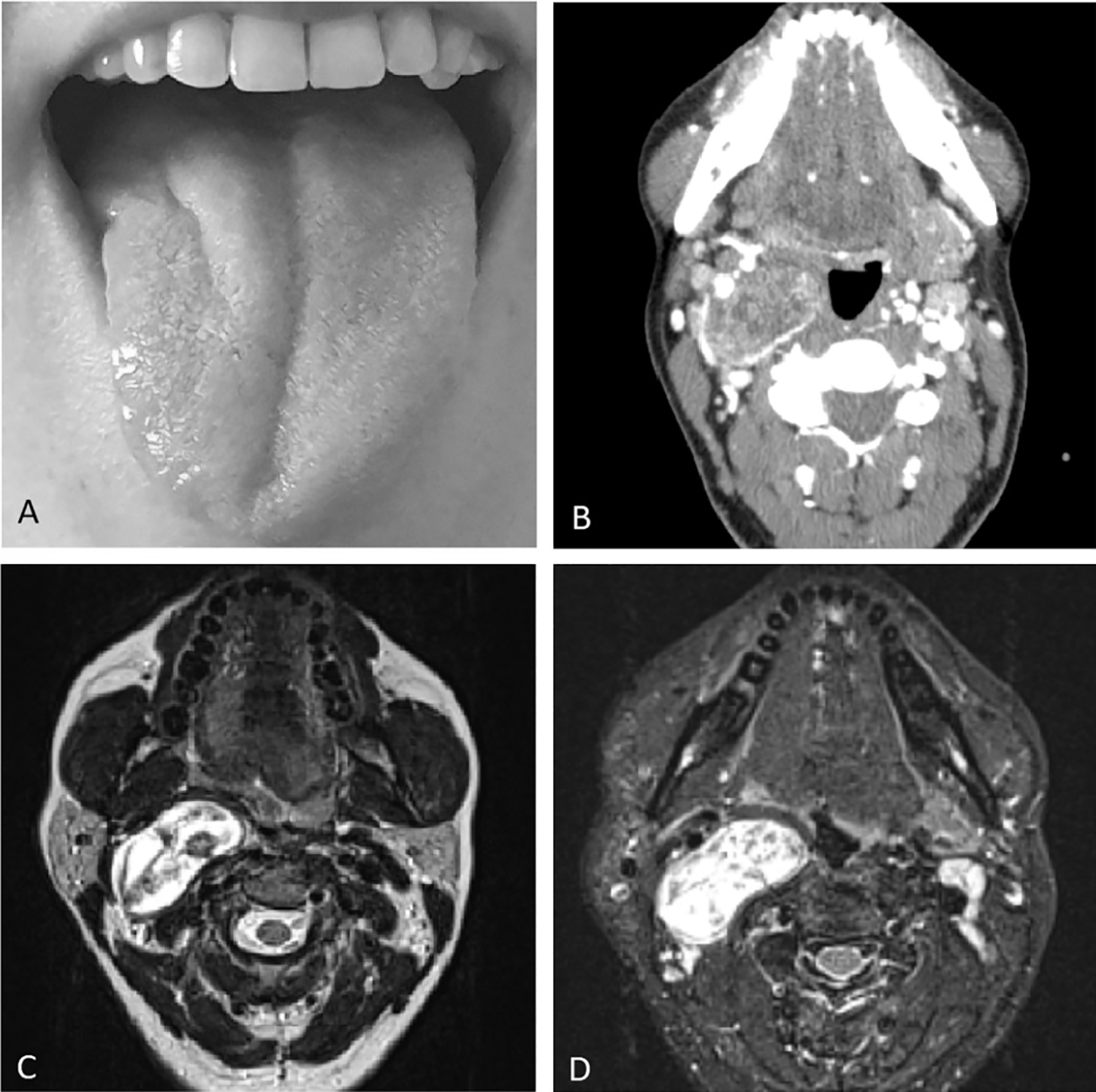
Right lateral deviation of the tongue during the protrusion is illustrated in (A). Contrast-enhanced computed tomography scan and axial T2-weighted and fat sat magnetic resonance images are illustrated in (B), (C), and (D), respectively.
The mass was finally excised through a transcervical approach: A careful sharp and blunt dissection of the parapharyngeal space and of the submandibular lodge was performed with sparing of the trunk of the hypoglossal nerve. Based on the strict association of the tumor with this structure and on the clinical evidence of tongue paresis, the tumor was considered to be arisen from the right XII cranial nerve.
In fact, pathologic examination of the mass revealed a mesenchymal neoplasm with morphological and immunophenotypic aspects compatible with peripheral nerve sheath tumor. Immunostaining for H3K27me3 was positive with an overall expression of Ki67 not exceeding 5% of cellularity; these 2 analyses are considered diagnostic and prognostics markers mostly used for malignant peripheral nerve sheath tumors.8,9 Moreover, the periwound lymph nodes sent with the surgical piece were free of morphological figures attributable to neoplasm.
Based on these findings, after a multidisciplinary discussion, a strict follow-up was proposed. After 1 month, the patient has almost completely recovered the paralysis of the tongue (Figure 2A), and on postoperative MRI, a moderate fluid flap was found in the operative site, nevertheless without postcontrast enhancements indicative of residues or relapses of disease (Figure 2B).
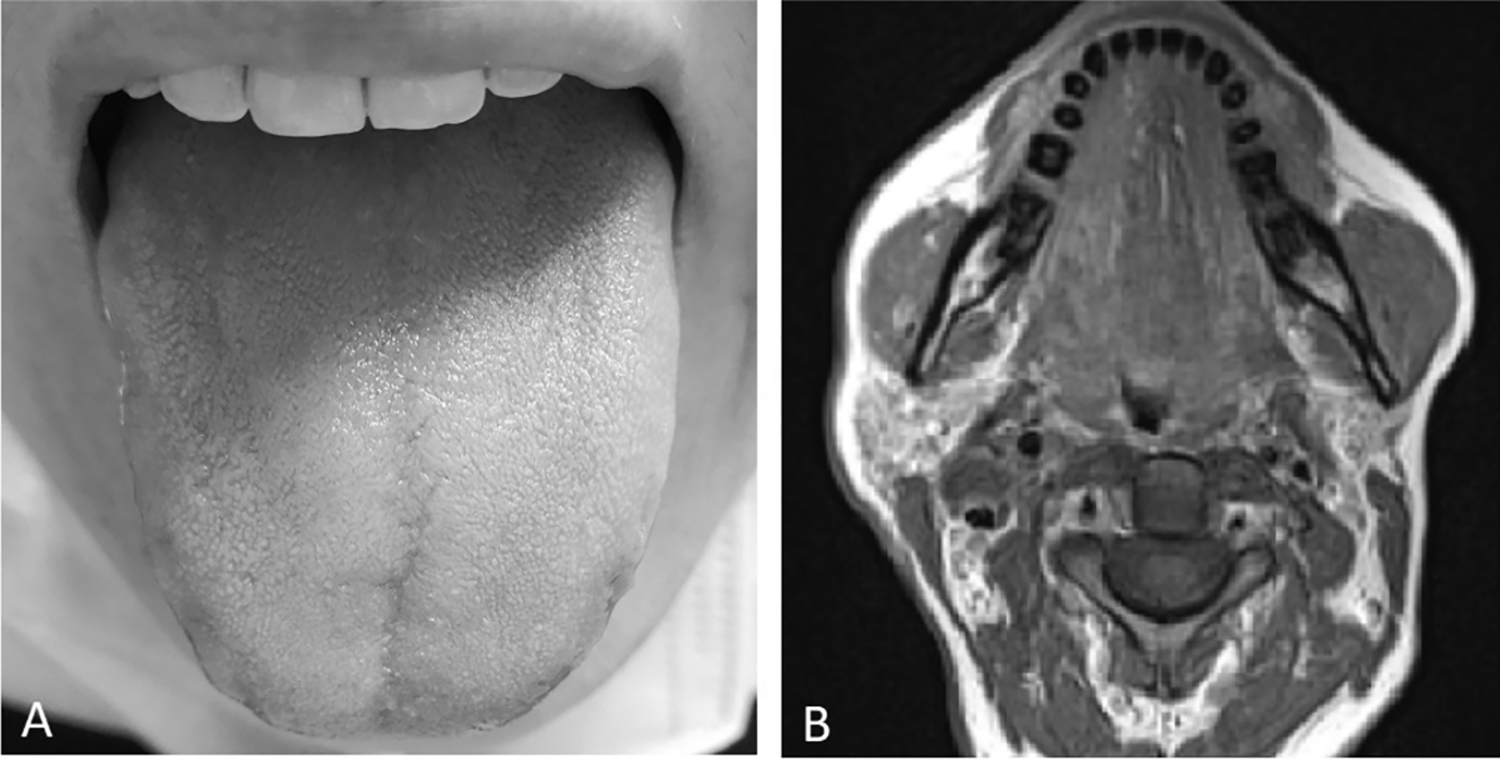
The complete recovery of the tongue paralysis is illustrated in (A). A postoperative magnetic resonance imaging performed at 1 month after surgery showing no residues of pathology is illustrated in (B).
The parapharyngeal space is defined as the deepest space in the neck and salivary gland; neurogenic or malignant tumors rarely develop in this region. The advent of modern imaging techniques has made it possible to better highlight the presence of retrostyloid neoformations, pointing out a relevant differential diagnostic challenge for clinicians; in fact, as reported in this case, a parapharyngeal space tumor could initially misunderstood for a neck abscess or a carotid tumor, emphasizing the importance of a multidisciplinary approach and clinical ENT evaluation in its proper management. After surgery was conducted, we faced a pathological entity that rarely affects this area; for this reason, we would recommend a review of the literature aimed at identifying the epidemiological and clinical features of hypoglossal Schwannoma with exclusively extracranial localization.
Footnotes
Authors’ Note
All the clinicopathologic investigations detailed in the manuscript have been conducted in accordance with the Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent for publication of data and images was obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.