
Abstract
Approaching the petrous apex can be complex and fraught with danger. Identifying favorable pathology and gaining access endoscopically is a direct, fast, and minimally invasive. Supported by navigation, it can be safely used in the vicinity of vital structures. A mucocele requires creation of a wide drainage pathway and can be an ideal lesion for such an approach.
Case
A 38-year-old male patient presented with complaints of headache and diplopia for 1 year. Lateral rectus palsy was identified. No other cranial nerve deficits were observed. A high-resolution computed tomography (CT) showed a space-occupying lesion in the petrous apex with dehiscence of the internal carotid artery (ICA) canal and erosion into sphenoid. Contrast-enhanced magnetic resonance imaging (CE-MRI) showed a T1 and T2 hyperintense lesion with smooth margins and no contrast enhancement. The horizontal petrous and vertical lacerum ICA segments were intimately associated with the lesion. The patient underwent a navigation guided transnasal transsphenoidal drainage of the mucocele (Figure 1). Greenish mucoid fluid collection was drained. The drainage pathway was widened. The patient had no significant postoperative complaints or complications. Cytology showed acellular mucoid material. The final diagnosis of petrous apex mucocele was established.
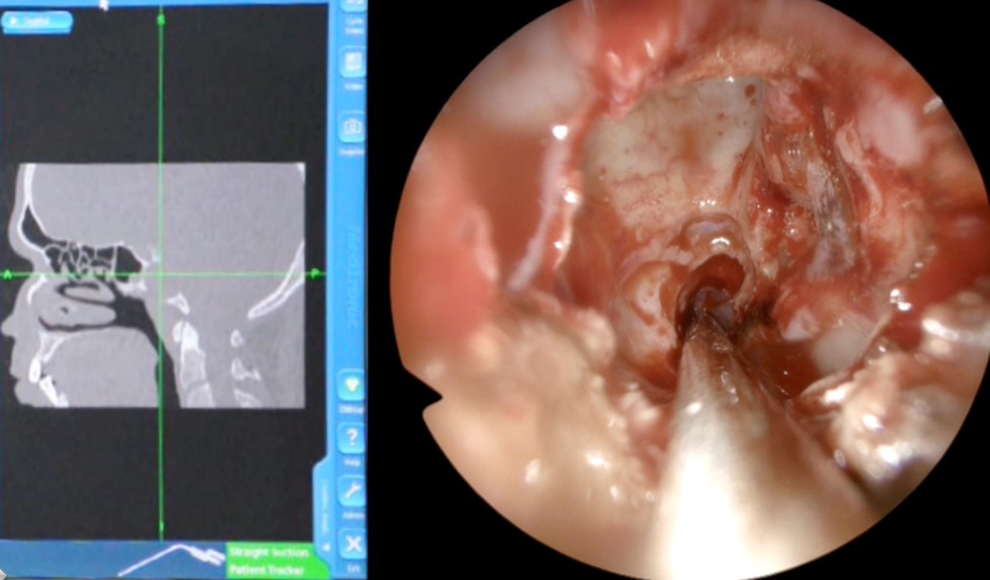
Endoscopic visualization of the mucocele, confirmed by neuronavigation system.
Follow-up endoscopy at 10 months showed a well-draining cavity (Figure 2). The lateral rectus palsy had fully recovered at the time of last follow-up, 24 months after the surgery.

Patent petrosphenoid opening on endoscopy at 10 months follow-up.
Discussion
Petrous apex is a complex area surrounded by important neurovascular structures. Primary petrous apex pathologies are usually diagnosed late on account of being rare and asymptomatic in the early stages. A cystic or lytic defect in and around the petrous apex can be caused by cholesteatoma, meningioma, schwannoma, giant cell tumor, cholesterol granuloma, ICA aneurysm, metastasis, or mucocele. 1
The clinical features are due to the mass effect of the lesion. They can impinge on cranial nerves IV, V, and VI. Larger lesions can involve VII to VIII nerve complex. Dural erosion may lead to cerebrospinal fluid otorrhea.
On CT, mucoceles appear as nonenhancing cystic lesions. 1 Cholesteatomas are typically hyperintense on diffusion-weighted MRI. 2 On histology, the cysts are lined by simple cuboidal epithelium. 3
Surgical drainage is the treatment modality of choice for symptomatic mucoceles. Surgical access to the petrous apex may be gained laterally via the translabyrinth, transtemporal, retrosigmoid, or middle cranial fossa approach or anteriorly via the transsphenoid approach. The location of the petrous apex makes the approach selection is a result-defining step in the management.
In 1979, DeLozier et al 4 used the transcochlear approach in the first reported case of petrous apex mucocele. The pterional, subtemporal, retrosigmoid, and middle fossa approaches require cerebellar or temporal lobe retraction, and the translabyrinthine/transcochlear route sacrifices hearing. Endoscopic approach provides a narrow corridor. Hui et al, 5 in 2012, were the first to drain the mucocele via this approach.
Advantages of endoscopic approaches include avoidance of a craniotomy, faster recovery, and shorter hospitalization. Common complications associated with lateral approaches, such as facial weakness and hearing, and vestibular loss, are not seen. When the petrous apex lesion is not accessible via the sphenoid sinus, a transpterygoid approach can be used. Following the vidian canal, which acts as a landmark for the petrous ICA, the petrous apex can be safely reached. Navigation helps in identification of the critical structures and enables creation of a wider opening.
The choice of surgical approach depends on the presentation, pathology, extent of the tumor, anatomic position of the vessels, and surgeon’s experience. Endoscopic transsphenoid approach with image guidance is a safe and effective method to create a drainage pathway for the mucocele of the petrous apex.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.