
Abstract
Objectives:
Peritonsillar abscess (PTA) is the most common deep neck space infection and a frequent cause for otolaryngology consultation. Patients often undergo computed tomography (CT) scan for confirmation in addition to physical examination. Our aims were to determine whether patients unnecessarily undergo CT scans in the emergency department (ED) when presenting with sore throat and identify physical examination characteristics that predict PTA.
Methods:
The electronic medical records of all patients (>18 years) presenting to an ED between June 2014 and June 2015 with a primary diagnosis of acute pharyngitis, acute tonsillitis, or PTA were reviewed for presenting symptoms and diagnostic imaging use.
Results:
Four hundred eight patients met inclusion criteria; 21 were diagnosed with PTA, including 13 based on history and physical alone. A total of 21 CT scans were ordered, 11 (52.3%) of which did not demonstrate abscess. Soft palatal fullness, uvular deviation, drooling, and muffled voice were all significantly associated with increased CT usage (all P values <.02). Rising subjective pain scores were associated with increased use of CT imaging (P = .029). Multivariable analyses revealed that soft palatal fullness, uvular deviation, and drooling were all significant predictors of PTA (all P values <.001).
Conclusions:
Patients with severe symptoms of PTA, including uvular deviation, drooling, and soft palatal fullness, were most likely to undergo CT imaging. Given the high likelihood of PTA, patients presenting with these symptoms could forego CT imaging, reducing exposure to ionizing radiation.
Keywords
Introduction
Peritonsillar abscess (PTA) is the most common deep space neck infection in the head and neck and a frequent cause for otolaryngology consultation. First described in the third century B.C. by Celsus, it is technically defined as a suppurative fluid collection within the space between the palatine tonsil capsule (composed of pharyngobasilar fascia) and the surrounding pharyngeal musculature. 1 A thin layer of loose connective tissue separates the capsule from the musculature. Once the infection spreads beyond the tonsil capsule, it is unlikely to spontaneously resolve. Additionally, its anatomic location allows extension to parapharyngeal and retropharyngeal spaces, which necessitates timely diagnosis and treatment.2,3
There are conflicting theories as to the etiology of PTA. It was originally believed to be a progression from tonsillitis. 4 Passy described a different mechanism whereby blocked Weber salivary glands lead to development of the fluid collection. 5 This was supported in pathologic studies by Kordeluk et al which demonstrated normal tonsillar tissue with surrounding inflammation and fibrosis involving the Weber glands in patients with PTA. 6 Although still commonly thought of as a complication of acute tonsillitis, Powell et al concluded that PTA is more often than not a pathogenically separate entity. 7 The microbiota of PTA has been studied extensively and it is most often a polymicrobial infection with oropharyngeal microflora including group A Streptococcus, Fusobacterium, and Streptococcus milerii as the most commonly encountered strains. 7 Recognizing resistant strains, in particular to β-lactam antibiotics, is important when treating these infections. 8
Peritonsillar abscess primarily affects younger individuals with a peak incidence during teenage years. 9 Risk factors for development include smoking, male gender, and recurrent tonsillitis.9,10 Signs and symptoms commonly include severe sore throat, muffled voice, drooling, and soft palatal fluctuance. Patients presenting with PTA are more likely to utilize emergency departments (EDs) and urgent care centers rather than primary care or specialty clinics at the time of presentation. 11 Although physical examination has been the gold standard for diagnosis, imaging studies are being utilized more commonly to aid in its recognition. Computed tomography (CT) usage within EDs is steadily increasing.12,13 There is a known risk to excess ionizing radiation exposure in adult patients which becomes even more concerning in the pediatric population where it has been linked to development of malignancy later in life.14-17
The primary aim of this study was to determine the frequency of CT usage for diagnosis of PTA when patients present with chief complaint of sore throat, and if ED first responder documentation supports its necessity. Secondary aims included identifying physical examination characteristics as indicators of PTA presence or absence.
Patients and Methods
Approval for the study was obtained from the institutional review board of the University of Louisville. Electronic medical records of patients presenting to the University of Louisville Hospital ED between June 2014 and June 2015 with primary diagnoses of acute pharyngitis (International Classification of Diseases [ICD 9, 462], ICD 10 [J02.9]), acute tonsillitis [ICD 9 [463], ICD 10 [J03.9]), or peritonsillar abscess (ICD 9 [475], ICD 10 [J36]) were queried. Inclusion criteria were evaluation by an ED first responder (resident physician, nurse practitioner, or attending physician), primary diagnosis of indicated ICD codes, and complete availability of electronic medical record. Patients were excluded if they were transferred from an outside facility with diagnosis of peritonsillar abscess from CT imaging.
Physician documentation of important presenting signs and symptoms was recorded including symptom days prior to presentation, otalgia, soft palatal fullness/peritonsillitis, uvular deviation, drooling, trismus, muffled voice, tonsillar hypertrophy, tonsillar erythema, tonsillar exudate, cervical lymphadenopathy, and pain. Computed tomography results and otolaryngology consultation were also recorded. If PTA was suspected or identified, procedural management and performing physician were noted. Return of purulence via surgical exploration (incision and drainage) was recorded when documented.
Mean, standard deviation and frequency summary statistics were calculated. Chi-square relative risk (RR) models tested frequency of CT usage. Univariate logistic regressions tested predictive factors for frequency of CT usage and predictive factors for presence of PTA. A multivariable regression tested the predictive value of presenting symptoms on a diagnosis of PTA. A univariate logistic regression then assessed the impact of pain ratings on likelihood of PTA diagnosis. All analyses were conducted in SPSS v. 26 (IBM) with α set at .05.
Results
Four hundred and eight patients met inclusion criteria (Table 1). The average age was 31.6 ± 12.3 years. Only one patient was admitted for inpatient management, while the remainder were discharged from the ED. Presenting symptoms were present an average of 7.6 ± 44.8 (range: 1-728) days prior to presentation, with the vast majority of cases presenting within 30 days. Pain ratings were available for 309 patients, averaging 7.2 ± 2.5 on a 0 (no pain) to 10 (severe pain) scale.
Emergency Department Recording of Presenting Characteristics.a
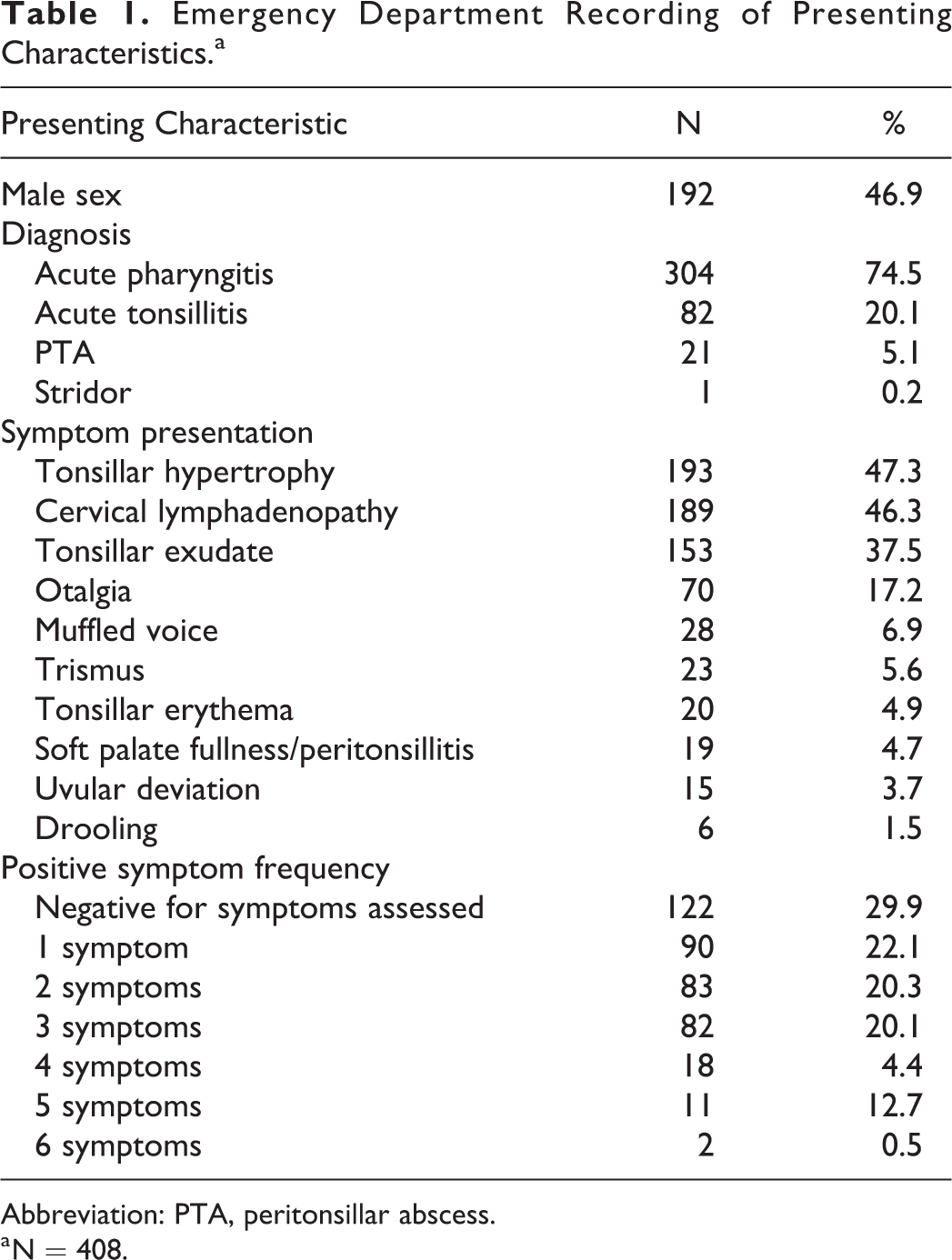
Abbreviation: PTA, peritonsillar abscess.
a N = 408.
Twenty-one CT scans were performed in total. Abscess was identified in 10 (47.6%) patients, whereas 11 (52.4%) CT scans identified no abscess. The otolaryngology service was consulted on 27 (6.6%) of 408 patients. Twenty-six patients subsequently underwent incision and drainage, of which 20 (76.9%) were performed solely by otolaryngologists. Return of purulence was noted in 17 (73.9%) cases.
Univariate logistic regression models revealed that ED providers were more likely to order CT scans when they recorded soft palatal fullness (RR = 14.4, 95% CI = 4.8-43.3, P < .001), uvular deviation (RR = 31.6, 95% CI = 4.1-243.9, P < .001), drooling (RR = 5.3, 95% CI = 2.0-14.3, P = .020), or muffled voice (RR = 10.8, 95% CI = 3.1-38.0, P < .001). Computed tomography ordering became more frequent as the number of presenting positive signs/symptoms increased, specifically 4 or more symptoms (odds ratio [OR] = 30.0, 95% CI = 5.4-165.3, P < .001). There was a small but significant increase in CT utilization when pain ratings were higher (OR = 1.3, 95% CI = 1.0-1.8, P = .029).
Among patients diagnosed with PTA, 13 (59.1%) were diagnosed by means other than CT imaging. A multivariable logistic regression entered presenting symptoms and revealed that presence of soft palatal fullness (OR = 74.2, 95% CI = 10.2-540.5, P < .001), uvular deviation (OR = 54.0, 95% CI = 5.7-507.9, P < .001), and drooling (OR = 21.1, 95% CI = 1.2-371.1, P = .037) emerged as significant positive predictors of the presence of PTA. A univariate logistic regression revealed that higher pain ratings were also associated with greater likelihood of PTA (OR = 1.4, 95% CI = 1.1-1.9, P = .014).
Discussion
Since the beginning of medicine, history and physical examination have been the cornerstones in diagnosis of disease. As new technologies emerge, physicians seek ways to use them to improve upon these building blocks. Some may even call into question the utility of physical examination when other means, such as CT and magnetic resonance imaging, exist today. However, these technologies are not without expense and risk to the patient. In the case of peritonsillar abscess, physical examination may prove difficult secondary to location and factors such as pain and trismus. The question then becomes how we can best leverage these technologies to assist with diagnosis, while minimizing risk to the patients.
Although it is accepted among otolaryngologists that history and physical examination are the gold standard for diagnosis of PTA, there is a lack of literature to support this notion. Scott et al demonstrated an overall 78% sensitivity and 50% specificity for diagnosis of PTA with history and physical alone but did not reveal which characteristics were used for diagnosis. 18 Hsiao et al noted in a study of 56 children that fever and unilateral neck mass were the most common presenting signs. 1 Uvular deviation and trismus were observed but did not show a statistically significant association. 1 In the current study, signs of soft palatal fullness, uvular deviation, and drooling were significant positive predictors of PTA. Trismus and muffled voice were not significantly associated with the diagnosis of abscess in our study. Similarly, while the average pain rating among patients diagnosed with PTA (8.8) was slightly higher, it was not substantially different from patients diagnosed with acute pharyngitis (7.1) or acute tonsillitis (7.4), precluding diagnostic distinction based on severity of pain rating alone.
Computed tomography has been used to aid in the diagnosis of a great many diseases, as is the case with PTA. Computed tomography usage within EDs as a whole is increasing with a 16% annual growth rate. 12 Previous studies have demonstrated great sensitivity and specificity using CT to diagnose PTA.18-20 Scholz et al demonstrated that low-dose CT (80 kVP) has enhanced abscess delineation and near perfect interobserver agreement in PTA diagnosis when compared with standard dose (120 kVP) CT scans, with much lower radiation exposure. 21 However, ionizing radiation at both doses carries the risk of malignancy, along with adverse effects related to contrast administration.14,16 In the present study, relatively few CTs were ordered when patients presented with sore throat symptoms. However, approximately 52% of the time when a CT was ordered, no abscess was identified. This may be because ED providers were ordering CTs on patients who complained of more pain, or who had trismus or muffled voice. Although these were all noted to increase CT usage in our study, we did not observe them to be significant predictors of PTA presence.
Other diagnostic imaging methods with less risk to the patient have been utilized for PTA diagnosis, namely ultrasound. Carratola et al showed that patients in the ED worked up for PTA without CT scan had shorter times to otolaryngology consultation, admission, and bedside procedure. 22 Constantino et al demonstrated 100% diagnostic accuracy for PTA with intraoral ultrasound (IOU) compared to 64% with needle aspiration. 23 Scott et al compared IOU to CT for PTA and demonstrated IOU had sensitivity of 89% and specificity of 100%. 18 Nogan et al demonstrated sensitivity of 100% and specificity of 70% for IOU. 24 The usefulness of IOU becomes limited when trismus is present, and transcervical ultrasound has shown promise in these clinical situations.25,26 Additionally, trials comparing transcervical ultrasound protocols to CT-guided diagnostics have demonstrated that use of transcervical ultrasound in the diagnosis of PTA in the ED provides decreased length of stay, lower costs, and less radiation exposure for patients.27,28 Although there are barriers, such as training and equipment costs, to using ultrasound within EDs, its use is gaining popularity and should be considered when choosing a diagnostic imaging modality for PTA.29,30
The ultimate goal of this study, among others, is to diagnose conditions such as PTA in a way that minimizes unnecessary risk to the patient. Wilson et al recently demonstrated that machine learning algorithms may help diagnose PTA in patients using input including trismus, otalgia, symptom duration, neck pain, and other history and physical findings with 72.3% accuracy. 31 Future studies analyzing pertinent positive and negative combinations of physical examination findings, such as those identified in this study, may help guide the creation of machine learning algorithms that identify common conditions such as PTA without the need for unnecessary imaging.
This study is not without limitation, including its retrospective nature and relatively small sample size, so findings must be interpreted with caution. The role of otolaryngology consultation prior to ordering a CT in the setting of suspected PTA remains to be fully elucidated. Varelas et al found that otolaryngology consultation reduced the use of CT scans in the setting of pediatric PTA. 32 It is unclear in this study if ED first responders are ordering CTs without consulting otolaryngologists or are doing so under the direction of the consultant. 33
Conclusion
Peritonsillar abscess represents the most common deep space neck infection encountered by the otolaryngologist. However, to date there remains no consensus on recommended steps in diagnosis and management of this disorder. Patients typically present in an acute setting, putting the burden of diagnosis on first responders, often in an ED. Diagnosis is not always apparent as signs and symptoms are nonspecific and differential diagnoses must be kept in mind. However, when patients present with signs of soft palatal fullness, uvular deviation, and/or drooling it is reasonable to forego CT scanning and proceed with definitive treatment. Furthermore, IOU has shown promise in diagnosing PTA without the need for CT. Future studies should focus on prospectively evaluating a diagnostic and treatment algorithm using the findings of this study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.