
Abstract
Specific bacterial infections can cause rapid necrosis of the nasal mucosa in immunocompromised patients, mimicking an invasive fungal infection. The exclusion of the latter is a priority because rapid deterioration and death may ensue within hours to days. The time lag between investigations and final diagnosis warrants empiric administration of Amphotericin B but patients are exposed to significant side effects. Histopathology and culture of the nasal tissues provide the necessary diagnostic clues to avoid inappropriate treatment.
Case Description
A 63-year-old male was referred to our Department with a 10-day history of severe pain and swelling in the facial and periorbital region on the right side. Bilateral nasal congestion without discharge was also reported. The patient had diabetes, ischemic heart disease, and myelodysplastic syndrome. He was on a daily dose of 64 mg of methylprednisolone for the last 3 months due to relapsing polychondritis. The patient was hemodynamically stable and apyrexial on examination. Moderate edema of the periorbital region but no exophthalmos, conjunctival injection, or chemosis were noted (Figure 1). On nasal endoscopy, crusts and necrotic areas were identified bilaterally in the anterior nasal cavity (Figure 2A and C). Opthalmologic assessment confirmed normal ocular motility and papilla. Initial diagnostic workup revealed marked leukocytosis with neutrophilia (white blood cell: 25.67 K/μL), anemia (hemoglobin: 8.7 mg/dL), elevated inflammatory indices (C-reactive protein: 3.57), and mild mucosal thickening with no indication of invasive inflammation or bony erosion in the paranasal sinus computerized tomography (CT) scan (Figure 3). Endoscopic biopsies from the nasal septal mucosa, inferior and middle turbinates were taken. Microscopic examination revealed fungal spores. An invasive fungal sinusitis was suspected on clinical grounds, and the patient was started on Amphotericin B until further diagnostic information became available. After appropriate staining, necrotic foci with an inflammatory infiltrate were noted in the nasal mucosa without any indication of fungal elements (negative periodic acid-Schiff and silver methenamine staining) granulomas or neoplastic cells. Tissue culture confirmed the presence of Klebsiella pneumonia and Pseudomonas aeruginosa. The patient received intravenous ciprofloxacin and ceftazidime/avibactam and was discharged 2 weeks post-diagnosis on oral antibiotics. Marked resolution of the crusts and necrotic areas was noted at 6 weeks posttreatment (Figure 2B and D).

Patient’s picture showing moderate edema of the right periorbital region with no noted exophthalmos, conjunctival injection, or chemosis.
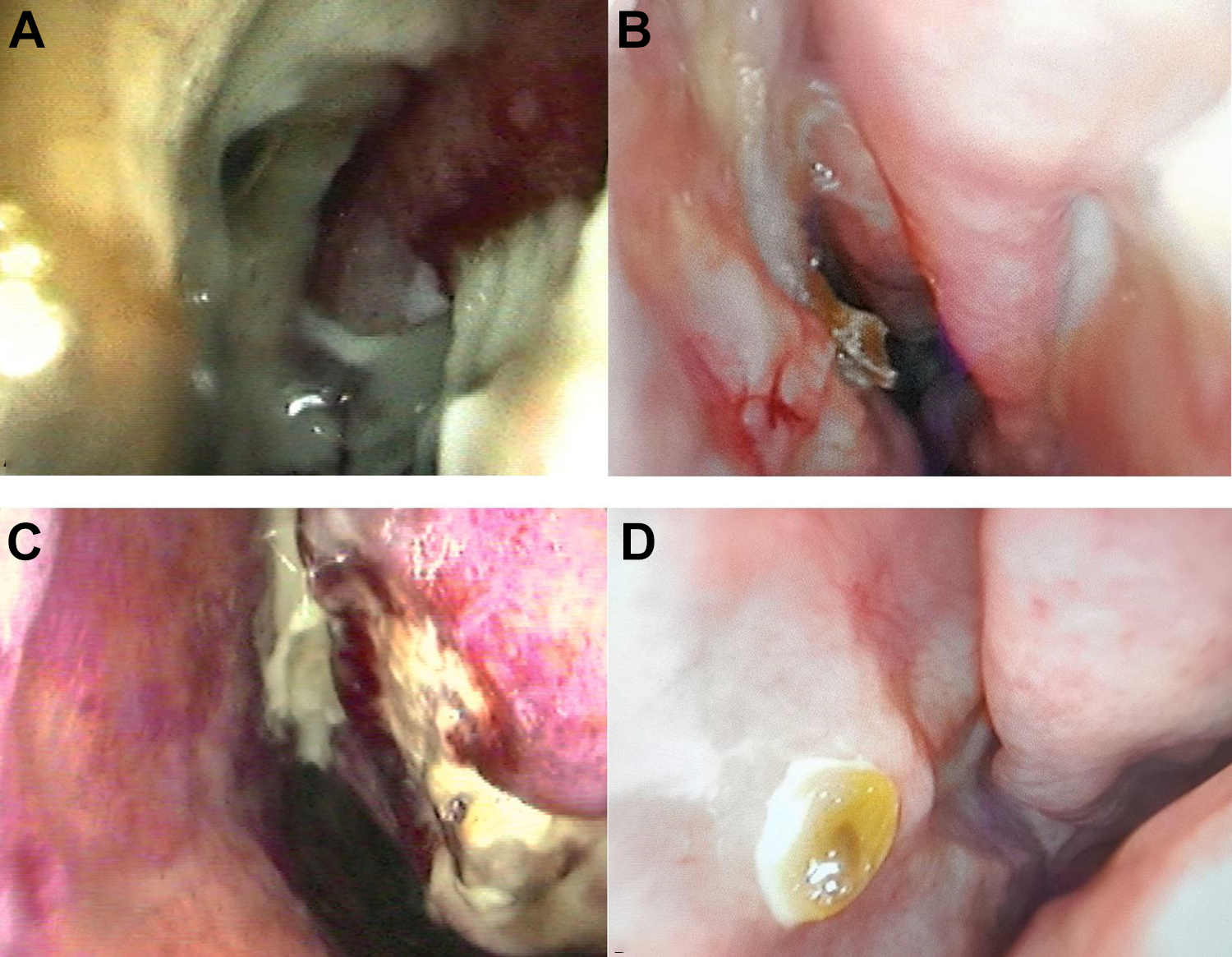
Endoscopic view of the nose. (A) Right nasal cavity at initial presentation, (B) right nasal cavity 6 weeks posttreatment, (C) left nasal cavity at initial presentation, and (D) left nasal cavity 6 weeks posttreatment.

Coronal image of paranasal sinus computerized tomography (CT) scan showing mild mucosal thickening with no indication of invasive inflammation or bony erosion.
The presence of necrotic tissue in nasal cavity may pose a diagnostic challenge. 1 There is a broad range of underlying benign or life-threatening diseases that could be considered in the differential diagnosis: bacterial or fungal infections, autoimmune diseases/vasculitides, neoplasms, and lesions from local illicit drug abuse. 2 Most of these entities present with a more protracted course and rarely cause acute facial edema. Klebsiella species shows a variety of presentations ranging from acute, as noted in this case, to chronic necrotic infections such as primary atrophic rhinitis and rhinoscleroma. 3 Diagnosis of the latter entities is based on epidemiological clues (endemic infections in tropical/subtropical and deprived areas), clinical clues (a chronic course with or without foul smell), radiology (atrophic changes in the nasal mucosa with resorption of the underlying bone), and histology (mucosa atrophy or granulomata and Mikulicz cells). 3
An invasive fungal infection should always be excluded in a timely fashion when an immunocompromised patient presents with sinonasal necrosis. 4 Aspergillus and mucor species are typically associated with an alarming clinical picture in neutropenic patients. Occasionally, the initial phase of an invasive fungal sinusitis may be characterized by mild or nonspecific symptoms, even, subtle changes in CT and thus cause a delay in treatment. 4 The presence of leukocytosis, as noted in our case, does not exclude a fungal infection. Long and high doses of oral steroids render patients immunosuppressed by definition and therefore susceptible to a fungal infection. Steroids may also be responsible for an elevated white cell count. On the contrary, the mere presence of fungus in the microscopic examination of sinonasal material may suggest colonization rather than infection. Nasal mucosal areas exposed to traumatic insult can be colonized by fungi and lead to ulceration and crusting. 2 The diagnosis will eventually rely on histology and culture. The absence of hyphae angioinvasion and thrombosis in the nasal mucosa precludes an invasive fungal rhinosinusitis. The abundance of inflammatory cells and the culture of specific bacteria, particularly Klebsiella and Pseudomonas species, point to a bacterial cause of the necrotic sinonasal infection.5,6
Footnotes
Authors’ Note
The authors declare that written informed consent for patient information and images to be published was provided by the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.