
Abstract
Purpose:
COVID-19 pandemic transformed the health system response worldwide. The aim of this study is to report changes about numbers and reason for ENT consultations in emergency department (ED) during COVID-19 pandemic comparing with those occurred the previous year (2019).
Methods:
Data about patients admitted to adult and pediatric ED were collected from March 1 to May 31, 2019 and 2020. Patients referred for urgency from general practitioners were excluded from the study.
Results:
Global ED admission (except for dyspnea or COVID-19–related symptoms) dramatically decreased during pandemic (−50.9% among adults and −71.4% among pediatrics). At the same time, ENT consultancy significantly reduced too, by 71.5% (P < .01) among adults and 45.1% (P < .01) for pediatrics. Among adults, it was reported a statistically significant decrease in consultation for ear problems (−88.5%, P = .0146). Reduction in ENT referral for bone fracture (−40%, P = .059), vertigo (−77.8%, P = .637), and tonsillitis (−87.5%, P = .688) was consistent, but not significant. Among pediatric patients, it was observed an increase by 25% about foreign bodies (12 vs 15, P < .01). A reduction in numbers of consults for ear problem (−90.8%; P = .045), epistaxis (−80%; P = .196), and nasal fracture (−70%; P = .36) was also observed.
Conclusion:
Fear of infection and the forced lock down caused a significant decrease in the number of ED accesses and in ENT consultancy. These data may suggest that some ED referral usually could be deferred, but on the other hand, pandemic will cause a great diagnostic delay.
Introduction
At the end of July 2020 in Italy, 247 537 patients had been infected by COVID-19 and 35 141 of them died. 1 The pandemic crisis changed drastically our lives since the end of February 20202,3; in order to limit the spreading of new coronavirus, a lockdown was imposed by a lot of governments worldwide, including Italy. 4 These measures had consequences also on the Italian health care system; indeed, both surgical and clinical activities have a massive limitation. During this period, only urgency/emergency and oncologic-related activities were allowed. 5 The aim of these measures was to (1) concentrate resources on the large numbers of patients infected by COVID-19 and (2) drastically reduce the number of noninfected patients accessing to hospitals that could be a high-risk place for new infections. The only service that had no limitations of access was the emergency department (ED). 6 Nevertheless, during the pandemic crisis (March to May 2020), it has been observed a drastic fall in the total number of access in ED despite the high number of people infected by COVID-19 using this service; this was probably due to the fear of the contagion. 7 As a consequence, consultations requested by both adult and pediatric ED operators also strongly diminished. The aim of this retrospective study was to report changes about numbers and reason for ENT consultations in (ED) during COVID-19 pandemic, making a comparison with those that occurred the previous year (non-COVID-19).
Methods
This is a retrospective study conducted from March 1 to May 31, 2020, at the ENT clinic of the University of Eastern Piedmont, Ospedale Maggiore della Carità in Novara, Italy. The study was carried out in accordance with the ethical standards of the Helsinki Declaration, and due to its observational nature, no ethical approval was required. Informed consent was obtained from all included patients. Inclusion criteria were informed consent about the use of clinical data and the need of ENT referral in ED. Exclusion criteria were declined informed consent and patients referred for urgency directly from general practitioner.
For each patient were collected general demographic information and ENT-related data (diagnosis and hospitalization details, if needed). These data were compared to those about the same period in the previous year (from March 1 to May 31, 2019). χ2 test and Fisher exact test were used.
Results
Data about 354 patients were analyzed (Table 1).
Demographic Characteristics of Population.
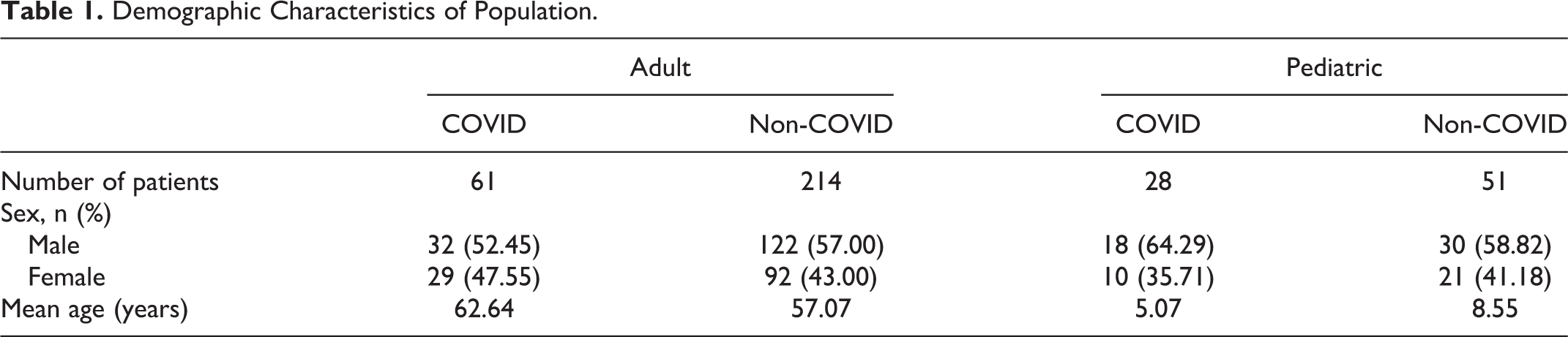
Population is divided into 4 groups: adult patient requiring ENT consults during COVID-19 pandemic (A1), adult patient requiring ENT consults in the same months in 2019 (A2), pediatric patient requiring ENT consults during COVID-19 pandemic (P1), and pediatric patient requiring ENT consults in the same months in 2019 (P2).
It has been observed that during COVID-19 pandemic, accesses to the ED in our center decreased about 50.88% (13 392 vs 6579) for adults and 71.37% (3653 vs 1046) for pediatrics.
Similarly, the number of ENT consults diminished from 214 (A2) to 61 (A1) during COVID-19 pandemic for adults (−71.5%, P < .01) and from 51 (P2) to 28 (P1) for pediatrics (−45.1%, P < .01). All these data are reported in Table 2.
Accesses to Adult and Pediatric ED During COVID-19 Pandemic and the Same Period in 2019.

Figure 1 presented a month-related reduction in percentage of ENT referral (among adult and pediatric).
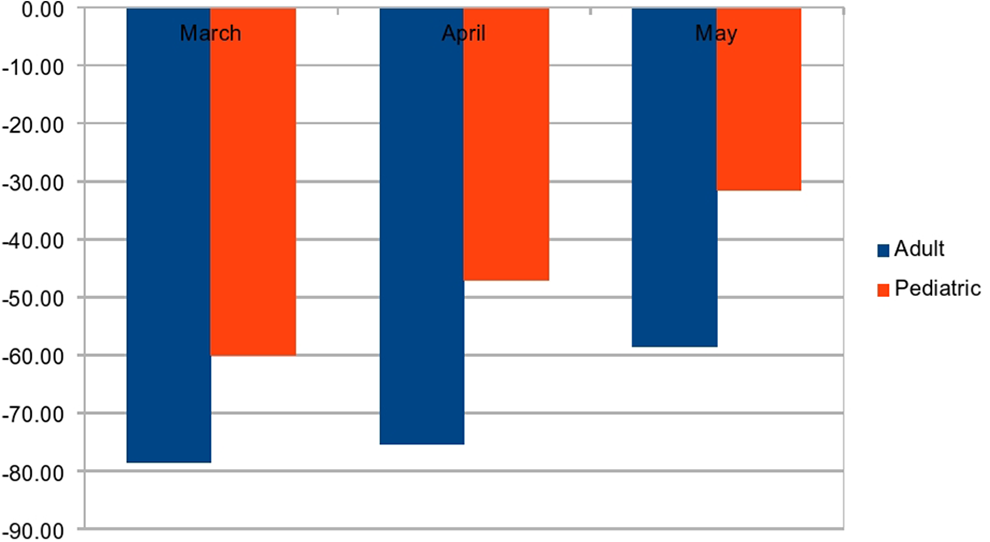
Reduction in percentage in ENT consult in adults and pediatrics during COVID-19 pandemic.
In May 2020, when lockdown began to be more permissive in Italy, accesses to the AD began to rise again compared to March and April even if no statistical significance was reached (group A1, P = .12; group P1, P = .66; Table 2).
Table 3 summarized the ranking of the 5 more common causes of consult request for each group.
Ranking of the 5 More Common Causes of Consult Request for Each Group.
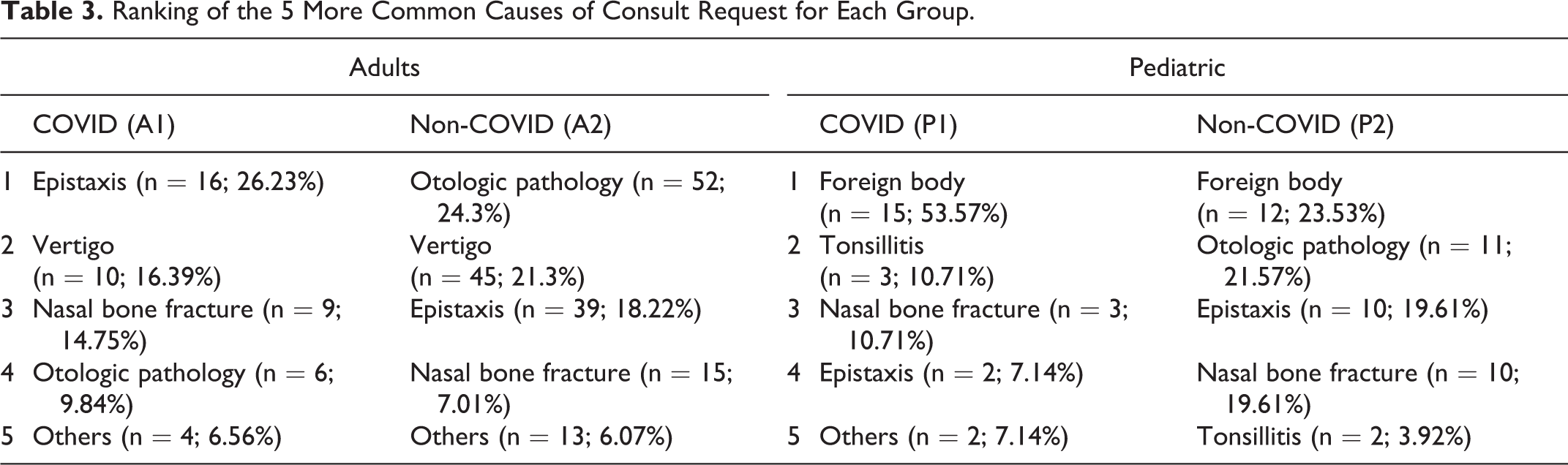
In group A1, a significant reduction in consults for otologic pathology (−88.5%, P < .01) was observed, compared to group A2; it is highlighted that 86.5% and 83.3%, respectively, of otologic pathology were represented by external/media otitis and earwax plugs. Reduction for vertigo (−77.8%, P = .637), tonsillitis (−87.5%, P = .688), and nasal bone fracture (−40%, P = .059) were consistent, but not statistically significant. In group A1, no complications consequent to surgical procedures were identified.
Comparing P1 and P2 groups, it was noticed how during Covid-19 period the number of foreign bodies raised from 12 to 15, corresponding to an increase of 25% (P < .01). In the same way, it has been registered a higher number of tonsillitis in group P1 compared to group P2 (P = .34).
In group P1, a reduction in the numbers of consults for otologic pathology (−90.8%; P = .045), epistaxis (−80%; P = .196), and nasal bone fracture (−70%; P = .36) compared to P2 was observed.
Concerning hospitalizations, it was observed that in group A1, 4.9% of patients needed hospitalization and 12.6% in group A2 (P = .105). Overall, a decrease of 88.8% of hospitalizations was described between adults.
Among pediatric patients, in group P1, 2 of 28 patients needed hospitalization; in group P2, 1 of 51 (7.1% vs 1.9%; P = .285).
Discussion
During COVID-19 outbreak, literature data reported a worldwide reduction in ED admission (a part from dyspnea). 5
In our experience, admission to ED drastically decreased for both adult and pediatric patients (−50.9% and −71.3%, respectively), especially when compared to those occurred during the same period in 2019; this happened despite the high number of people infected by COVID-19 and requiring health care. 8
Following this trend, ENT consults also strongly decreased by 71.5% (P < .01) in the adult population and 45.1% (P < .01) in pediatrics. This reduction could be partially due to lockdown restriction regarding human mobility 4 and partially due to widespread fear of contagion. 9 This is the reason why during May, despite lockdown policy having become less strict in Italy, ED admission continued decreasing, by 58.5% (adults) and 31.6% (pediatrics). This study reported a significant reduction, especially among ear problems (mainly otitis and earwax plugs) and vertigo, which can be easily treated by general practitioners as first consultation or by telemedicine. 10 The reduction among tonsillitis (−87.5%, P = .688) and nasal bone fractures (−40%, P = .059) were probably influenced by movement restriction and limited contact with other people, including physical activity (especially for contact sports). 11 In group A1, no complications after surgery were reported: These data were justified by the restrictions in surgery activity, which allowed only oncological and emergency surgery. 5
On the contrary, during COVID-19, the number of referral for foreign bodies increased about 25% (P < .01): This is well known as such kind of accidents most frequently occur in domestic context. 12 On the other hand, it was noticed a reduction in numbers of consults for otologic pathology (−90.8%; P = .045), epistaxis (−80%; P = .196), and nasal bone fracture (−70%; P = .36). These data can be justified by the same issues explained for adults. 10
The number of hospitalizations was basically comparable between group A1 and group A2 and between group P1 and group P2.
The fear of contagion and “nosophobia” related could lead to diagnostic delays and generate an emerging problem: This should be carefully monitored and managed in the next future in order to avoid a heavy impact on patients’ quality of life and socioeconomic system. 13
This study has some limitations: First of all, a relatively small number of patients involved and enrolled in a single center; second, pivotal bias should be considered that our hospital belongs to a geographical “red zone” for COVID-19 diffusion. It could be supposed that in the southern part of Italy (with a very low rate of viral spread), a different trend in ED accesses had occurred.
Conclusion
Among the commonest causes of ENT consulting, it was noticed a reduction mainly in referral for ear problem and vertigo. Also, accesses for nasal bone fracture and tonsillitis decreased probably due to the limitations in personal movements of lockdown.
All these data seem to suggest that part of routinary ED accesses are not fully appropriate and do not require a specialist examination; such kind of pathology should be easily managed outside the hospital by family doctors.
This reduction in ED accesses will probably cause some diagnostic delays in the following months.
Footnotes
Authors’ Note
Consensus was obtained by the patient involved in the retrospective study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.