
Abstract
Objectives:
The most common type of noninvasive fungal rhinosinusitis is fungus ball (FB), which usually involves a solitary paranasal sinus. Multiple fungus balls (MFBs) are rarely reported in literature. The purpose of this study was to analyze and compare the clinical features of MFBs and solitary fungus ball (SFB).
Methods:
We retrospectively investigated consecutive cases of FB between 2001 and 2018 and compared the clinical records of SFB with MFBs with respect to demographics, clinical features, location, radiological findings, and operative outcome.
Results:
A total of 440 SFB and 43 MFBs cases were included in the study. The mean age was 55.3 ± 13.3 and 60.6 ± 10.9 years, respectively (P = .011). The incidence of MFBs obviously increased from 2001 to 2018. The clinical symptoms and laboratory examination were similar. On computed tomography images, complete opacification, septal deviation, Haller cells, and obstruction of ostiomeatal complex were more common (P < .05). The incidence of SFB on the left and right sides was similar, while MFBs were seen to involve both sides in 74.4%.
Conclusions:
Compared with SFB, MFBs showed some special characteristics. The MFBs affected older patients showed wide range of lesions and complex anatomy. Surgical technique is very important. Much more attention should be paid to this not so uncommon disease during the perioperative period.
Introduction
Fungi are ubiquitous in nature and the respiratory epithelium will be inevitably exposed to the environment with fungi. Asymptomatic fungal spores on the sinonasal mucosa are common and requires no treatment. Only a few fungi stay in the paranasal sinuses and cause fungal rhinosinusitis (FRS). Although Paknezhad et al suggested the existence of an intermediate form of fungal sinusitis, 1 FRS can be generally divided into invasive and noninvasive types based on whether the mucosa has been invaded.2,3 The invasive FRS often affected immunosuppressed patients, whereas the noninvasive FRS usually occurs in immunocompetent patients. The noninvasive FRS can be further classified into 2 categories: fungus ball (FB) and allergic fungal rhinosinusitis (AFRS).
Fungus ball has several different terminologies, such as mycetoma, aspergilloma, and chronic noninvasive granuloma. But actually mycetoma is a local disorder comprising a granulomatous infection affecting the skin of the lower limbs. 4 With the improving understanding of the pathophysiology of the disease, more researchers recommended using FB instead of mycetoma. Fungus ball is a kind of noninvasive aggregated dense coagulation of fungal hyphae in one sinus cavity, usually the maxillary sinus. Although it may affect multiple sinuses, it is rarely observed as multifocal FB. 5 Unilateral fungal ball and bilateral fungal balls (BFBs) have been reported in the literature,6-15 but there are few reports for multiple fungus balls (MFBs). The purpose of our study is to compare the clinical characteristics of solitary fungus ball (SFB) and MFBs in patients treated at a tertiary medical center in China (2001 to 2018).
Patients and Methods
We reviewed 483 consecutive cases of fungus ball from 2001 to 2018 and found 440 cases of SFB and 43 cases of MFBs including 3 patients had metachronous fungal ball in different sinuses. The diagnosis of FB was made according to DeShazo’s criteria. 2 Computed tomography (CT) was performed preoperatively in all cases. Serum total immunoglobulin E (IgE) and allergen test including Specific IgE (SIgE) and skin prick test (SPT) were performed. Blood eosinophilia percent (BEP) and value (BEV) were also assessed. Surgeries were performed in the department of Otorhinolaryngology Head and Neck Surgery of Peking University People’s Hospital. The intrasinusal mass was collected in all patients and sent to the pathology laboratory to confirm the presence of hyphae. A mucosal biopsy was performed to exclude invasive FRS. Allergic fungal rhinosinusitis was identified and ruled out through comprehensive analysis of demographic data (younger, atopic), symptoms (thick mucus), examination (thick, tenacious, peanut butter-like secretion), CT imaging (expansile, hyperattenuating material characteristic), histology (eosinophil-rich mucus, Charcot-Leyden crystals), treatment (surgical treatment with systemic corticosteroids), and prognosis (recurrent is not uncommon).16,17 The demographics, clinical features, radiological findings, structural variations, laboratory test, intraoperative presentations, the outcomes of the surgery, and postoperative management were recorded and analyzed. All patients were followed with endoscopy postoperatively every 1 or 2 months at least half a year in the outpatient department.
Statistical Analysis
The Pearson’s chi-square tests or Fisher exact tests were used to determine differences in the categorical risk factors (gender, symptoms, concomitant diseases, laboratory tests, the paranasal sinus involved in the lesion, and radiological findings). The 2 independent sample t test was conducted to examine for difference in age and follow-up periods between cases of SFB and MFBs. The change in the incidence of MFBs was performed using the linear by linear association. Value of P < .05 was considered statistically significant for all analyses. Statistical analysis was performed using SPSS version 24.
Results
Incidence
From 2001 to 2018, 3136 patients with chronic rhinosinusitis were admitted to the otorhinolaryngology in-patient department of our hospital and functional endoscopic sinus surgery (FESS) was performed, of which 483 were diagnosed with FB. The incidence of FB was 15.4%. The number of FB, MFBs, and SFB patients who underwent surgeries has increased obviously over the past 18 years. On a 6-year basis, not only the incidence of FB in chronic rhinosinusitis (CRS) (P = .022) but also the incidence of MFBs in FB statistically significantly (P = .002) increased (Figure 1).
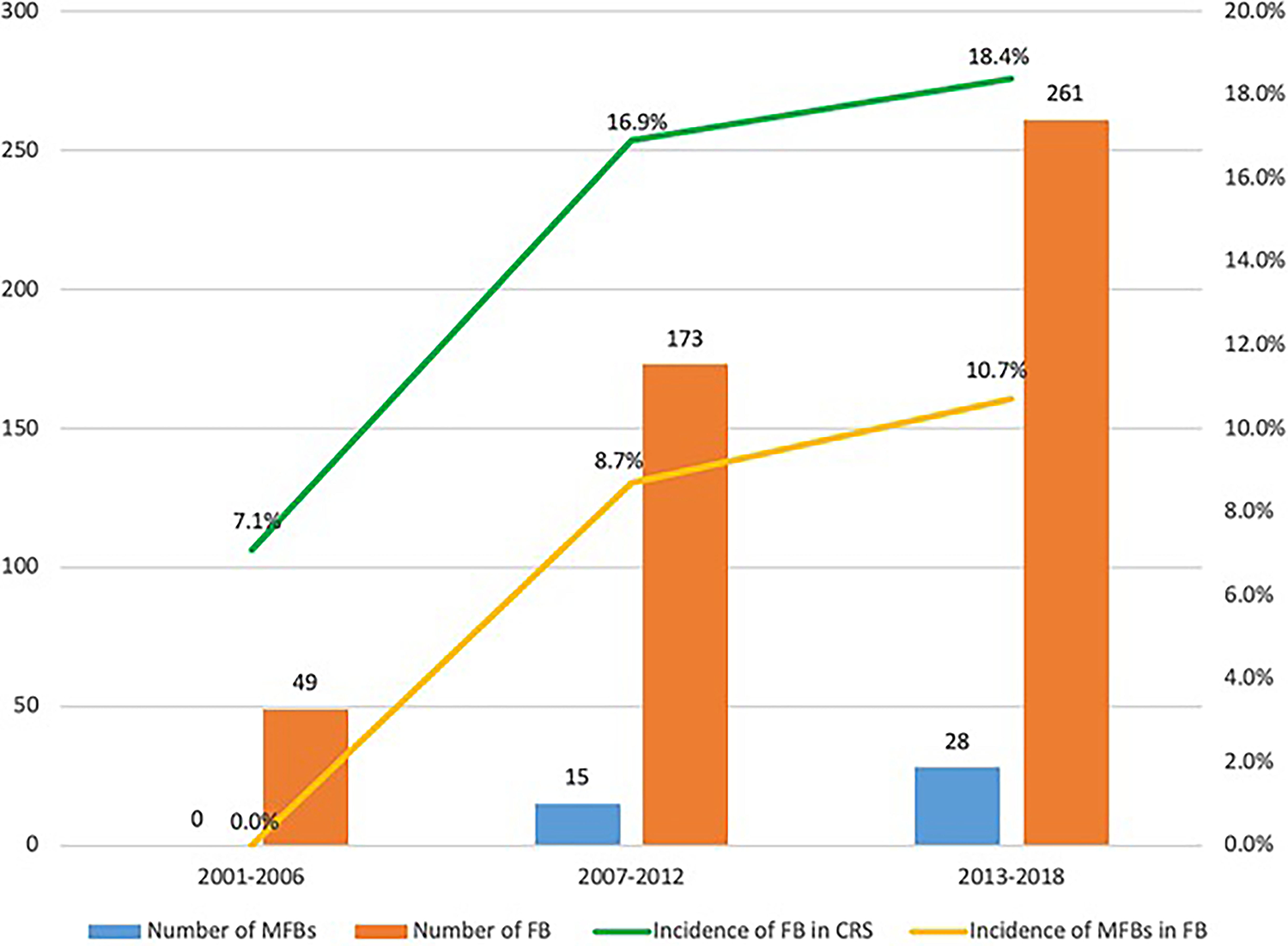
Change in the incidence and number of MFBs over 18 years. MFBs indicates multiple fungus balls.
Demographic Data
The average age of 440 SFB patients was 55.3 years (range: 24-84). There were 297 (67.5%) females and 143 (32.5%) males, showing a 2:1 female predominance. In 43 patients with MFBs, the average age was 60.6 years (range: 34-83). There were 30 (69.8%) females and 13 (30.2%) males, showing a similar female predominance (Table 1). The age of the patients in the 2 groups was statistically significant (P = .011). There was no difference regarding gender between the 2 groups of patients.
Demographic Data.
Abbreviations: IgE, immunoglobulin E; MFBs, multiple fungus balls; SFB, solitary fungus ball.
a P < .05.
Clinical Manifestations
The most common symptom in patients with SFB was pain, which was present in 263 (59.8%) patients. This was followed by purulent rhinorrhea, with 260 (59.1%) patients with this symptom, and other symptoms including nasal obstruction, foul odor, cheek tenderness, and orbital and periorbital pain. The most common symptom in patients with MFBs was pain, followed by purulent rhinorrhea and nasal obstruction (Table 1). Thirty-one (7.0%) patients with SFB and 3 (7%) patients with MFBs did not present with any symptoms, and FB was discovered incidentally on the head and neck images during a workup for other diseases. There was no difference in symptoms between the 2 groups of patients.
Concomitant Diseases
Among the 239 (54.3%) cases of SFB with concomitant disease, hypertension was the most common (30.9%), followed by heart disease (11.6%), diabetes mellitus (10.7%), and others including tumor, allergic rhinitis, liver disease, renal disease, immunological disease, and asthma. Among MFBs patients, 28 (65.1%) patients had concomitant diseases, with heart disease and hypertension occupying the top 2 places. Heart disease were more common in patients with MFBs than those in SFB (P = .028; Table 1).
Laboratory Examination
Of the 440 patients with SFB, 165 had been tested for total serum IgE, and 30 (18.2%) of them had higher than normal results. Of the 43 MFBs patients, 22 had the test and 6 (27.3%) of them had above-normal results. The above-normal results were no difference between the 2 groups. A total 286 of the 440 SFB patients and 37 MFBs patients were tested for allergens by means of SIgE or SPT. A total of 85 (29.7%) SFB patients and 10 (27%) MFBs patients were positive for allergens. There was no statistical difference between the 2 groups (Table 1). Of the 440 patients with SFB, 7 (1.6%) had higher results than normal in BEP (0.4%-8% is the normal range) and 10 (2.3%) in BEV (0.02-0.52 × 10 ^ 9 is normal range), while BEP and BEV in 43 patients with MFBs were both within the normal range. There was no difference between the 2 groups (Table 1).
Location of the Lesion
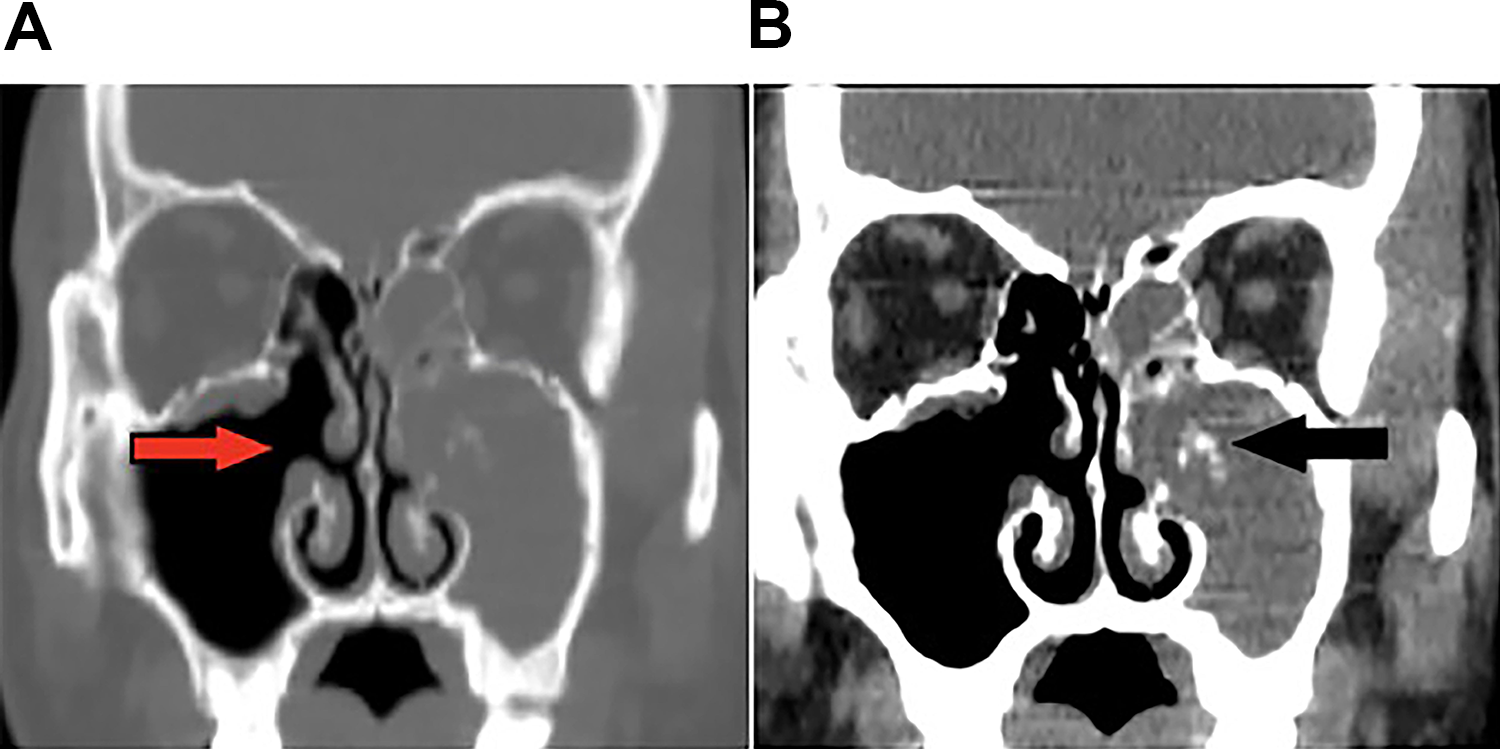
In SFB patients, 211 (48.0%) cases had lesions on the right side and 229 cases (52.0%) on the left side. The most frequently involved sinus was maxillary sinus (89.8%), followed by sphenoid sinus and ethmoid sinus, and no frontal sinus was involved. In patients with MFBs, unilateral lesions were observed in 11 (25.6%) patients (3 left, 8 right) and bilateral lesions in 32 (74.4%) cases (Figures 2 and 3). There were 9 (20.9%) involved ipsilateral maxillary sinus and ethmoid sinus in MFBs patients. The most common sinus involved was maxillary sinus (90.7%), followed by sphenoid sinus, ethmoid sinus, and frontal sinus. (Table 2). The maxillary sinus was most frequently involved in both groups, but there was no statistical difference between the 2 groups. Sphenoid sinus and ethmoid sinus were more common in MFBs patients.
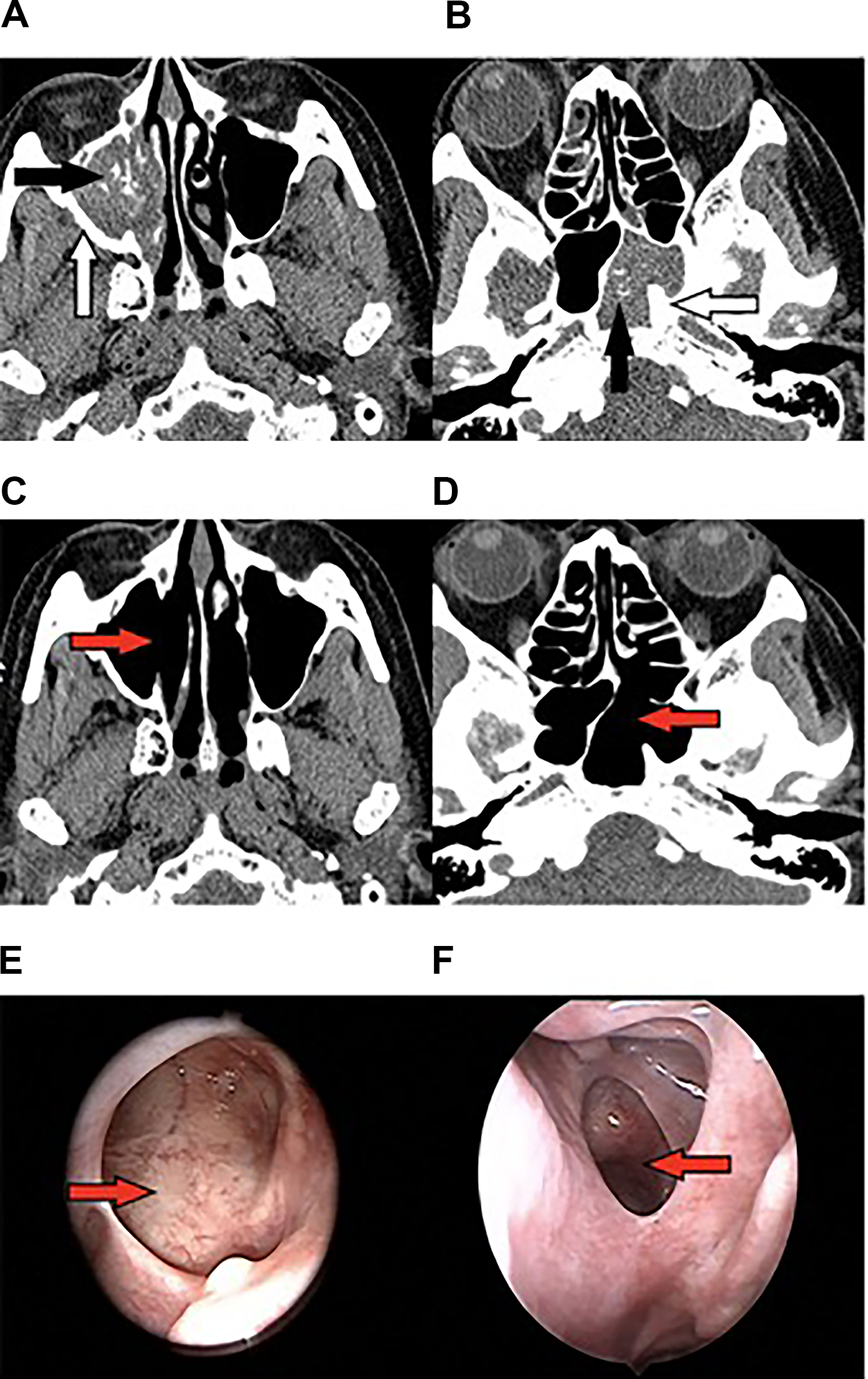
Bilateral MFBs: Preoperative (A, B) and postoperative (C, D) CT scans, and postoperative endoscopic views (E, F). Calcification (black arrow). Sclerosis (white arrow). Patient ostia (red arrow). CT indicates computed tomography; MFBs, multiple fungus balls.
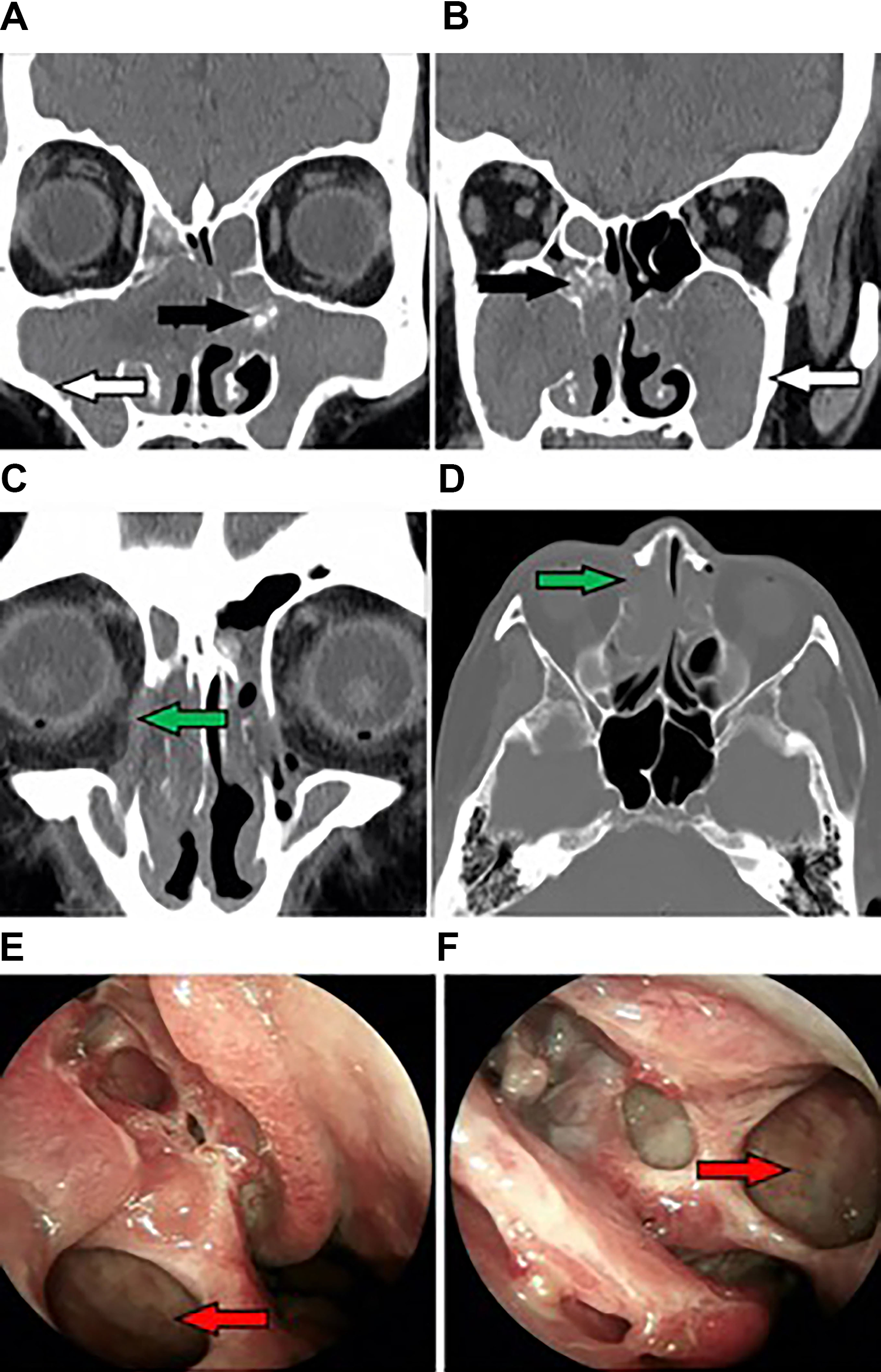
Bilateral MFBs: Preoperative CT scans show (A, B) calcification (black arrow), sclerosis (white arrow), and erosion of bone (C, D) (green arrow). Postoperative endoscopic views (E, F) patent ostia (red). CT indicates computed tomography; MFBs, multiple fungus balls.
Localization of SFB and MFBs.
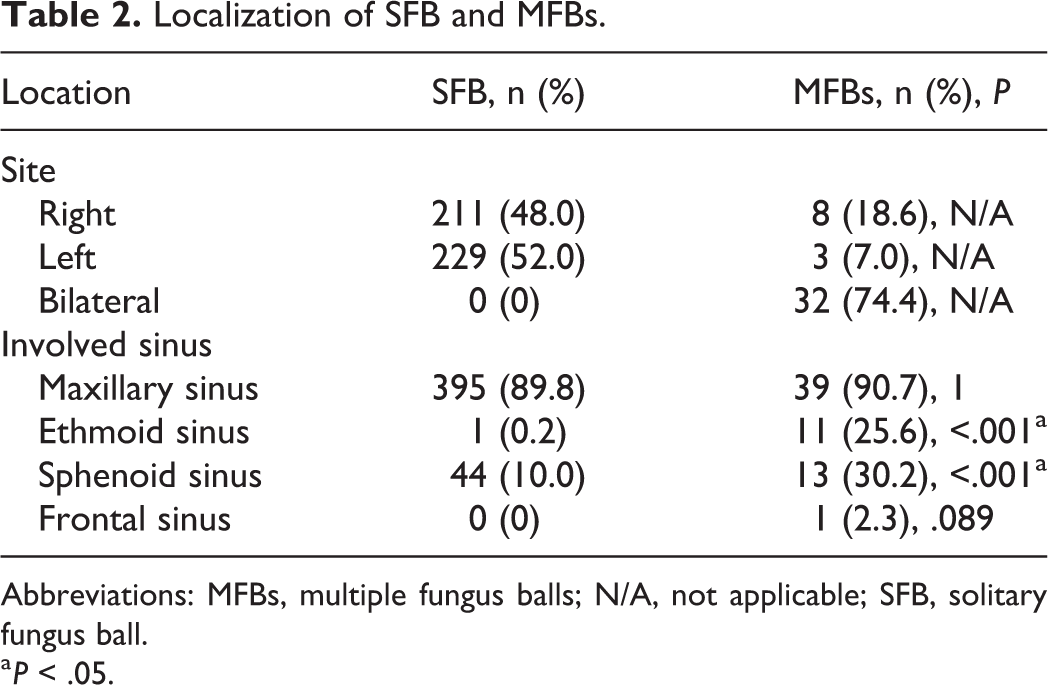
Abbreviations: MFBs, multiple fungus balls; N/A, not applicable; SFB, solitary fungus ball.
a P < .05.
It was interesting to note that 3 bilateral maxillary FBs presented metachronous unilateral lesion, which is not mentioned in other literature involving FB. One male patient presented right maxillary FB when he was 35 years old and had left maxillary FB at age 47 (Figure 4). The other 2 female patients showed right maxillary FB at 59 and 65 years old, respectively, and the left maxillary sinus fungal balls at 62 and 68 years old, respectively.
Metachronous bilateral MFBs: The CT scans show after the first right antrostomy, before the second left antrostomy (A, B). The patent maxillary ostium (red arrow). Calcification (black arrow). CT indicates computed tomography; MFBs, multiple fungus balls.
Computed Tomography Findings
All 440 SFB and 43 MFBs patients undertook CT preoperatively, but CT scans of 207 SFB and 14 MFBs patients were not available to review because their CT scans were undertaken in other hospitals. So we analyzed the CT images of 262 patients in 2 groups. In patients with MFBs, complete opacification was more common than that of SFB (P = .036; Table 3). Sclerosis of the sinus wall and bony erosion of the sinus wall were also more common in patients with MFBs, but there was no difference between the 2 groups. Punctate calcifications were observed in 188 (80.7%) SFB patients and 27 (93.1%) in MFBs (P = .1; Figures 2–4). In contrast, soft tissue density was noted in 45 (19.3%) patients in the SFB group and 6 (20.7%) in MFBs group (P = .86). In both groups, calcification was more common than soft tissue density. We also evaluated the obstruction of ostiomeatal complex and anatomical variation. Obstruction of ostiomeatal meatus, deviation of nasal septum, and Haller cells were more common in MFBs patients (5.6% vs 82.8%, 53.6% vs 75.9, 12.4% vs 55.2%, respectively, P < .05), but there was no statistical difference in Concha bullosa between the 2 groups (P = .284).
Imaging Features of Patients With SFB and MFBs.
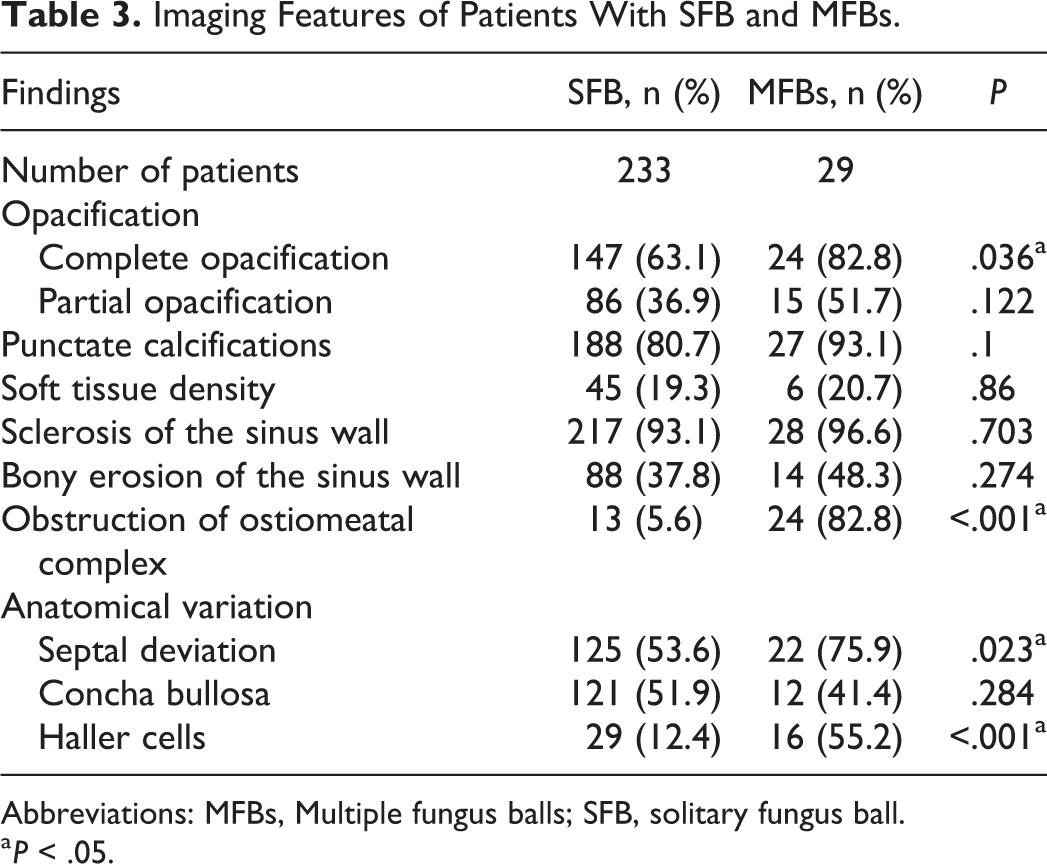
Abbreviations: MFBs, Multiple fungus balls; SFB, solitary fungus ball.
a P < .05.
Treatment and Outcomes
Functional endoscopic sinus surgery was performed in all SFB and MFBs cases. All fungus ball could be removed through malleable angled suction and 50 mL syringe irrigation after sinusotomy. Intrasinusal mass exhibited clay-like material which was confirmed FB by histopathology. No tissue invasion was found in all cases. The mean follow-up time of patients with SFB and MFBs was 20.9 ± 8.4 months and 21.4 ± 9.7 months, respectively (P = .711). Among the patients with SFB, only 1 (0.2%) relapsed, while none of the MFBs patients recurred (P = 1).
Discussion
Fungus ball is the most common category of FRS, and MFBs is a special type of FB. Multiple fungus balls is not like the common SFB, which usually only affects one sinus. Multiple fungus balls can affect multiple, usually bilateral sinuses. Because MFBs is a much more uncommon and special type of FB, very few studies address it. Some papers reported a few cases of bilateral paranasal sinuses involvement of FB6-15 (Table 4). Few papers particularly address multiple paranasal sinuses involvement in FB 5 (Table 4). In this retrospective study, there were 43 cases of MFBs in 483 cases (8.9%) of FB; 32 of the 43 patients (74.4%) had bilateral paranasal sinuses involvement. To the best of our knowledge, this is the first original article to address the special type of MFBs issue. On a 6-year basis, we can see both the number and incidence of MFBs increased obviously. Although the incidence of FB in the general population is unknown, many recent studies have shown that the incidence of FB has increased steadily in the past decades. 11 The exact reasons are not clear, which may be related to longer life expectancy, improved diagnostic experience, and advances in imaging techniques.9,11 We think maybe the incidence of both the FB and MFBs will increase in the future. It is therefore necessary for us to be familiar with MFBs.
Summary of Studies Related to BFBs and MFBs.
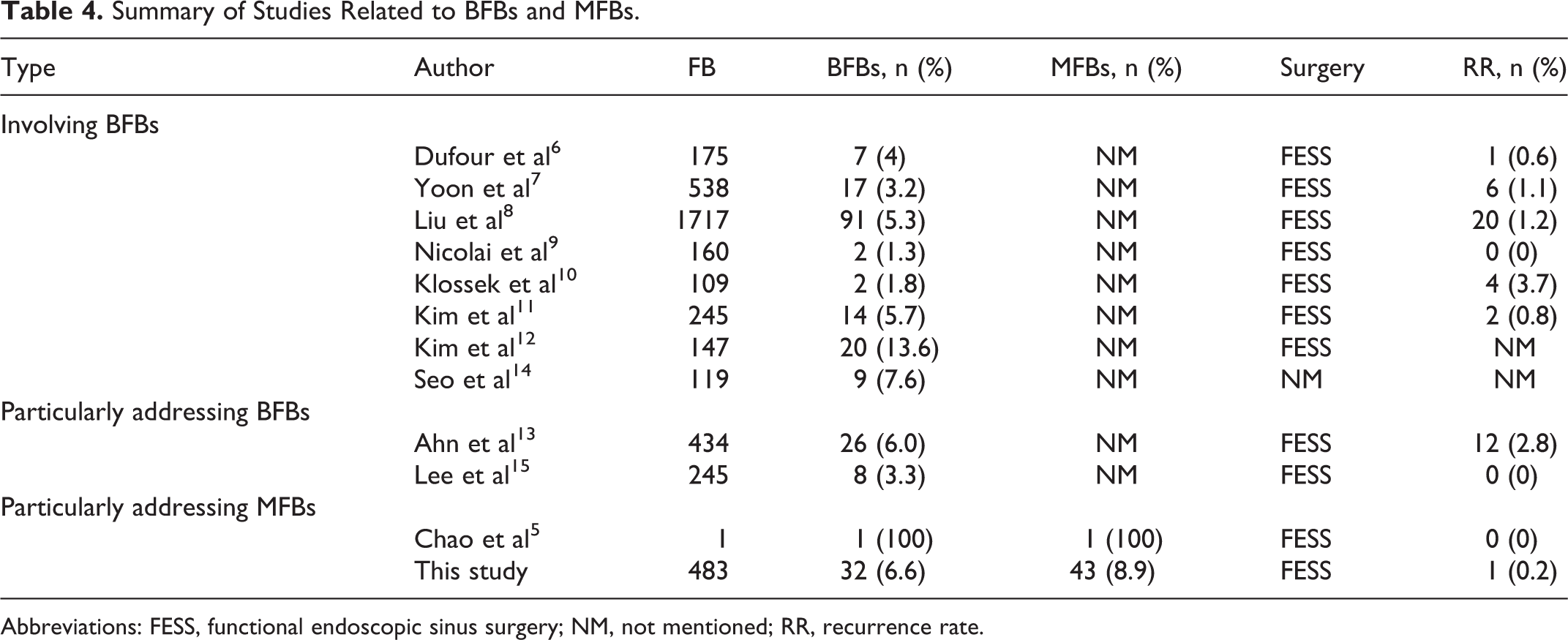
Abbreviations: FESS, functional endoscopic sinus surgery; NM, not mentioned; RR, recurrence rate.
There is an evident female predominance in many FB studies.6,8,11,12 A female predominance was also seen in our research, showing a 2:1 female predominance approximately in the 2 group and there was no statistical difference. No consensus has been reached about the etiology of the female predominance, several studies have suggested that the possible explanation may be associated with the environmental and hormonal factors.6,12
Fungus ball has also been reported to affect the elderly patients.5,8,9,11,12 Our series is in accordance with the results. In our study, the average ages of the 2 groups were 55.3 and 60.6, respectively. The age difference between the 2 groups was statistically significant. It proved that MFBs affected older patients than SFB in this research. With respect to concomitant diseases, heart disease was more common in patients with MFBs than those in SFB. Although it was unclear whether the higher occurrence of concomitant diseases was associated with age or with MFBs, it was certain that the older the patients were, the more likely they were to get concomitant diseases and the greater the risk of surgery. Therefor it is necessary to diagnose MFBs and perform surgery as early as possible for the patients.
The most common symptoms of both groups were pain (59.8% vs 67.4%, including: headache, cheek tenderness, orbital and periorbital pain, toothache, and eyeball pain), purulent rhinorrhea (59.1% vs 53.5%), and nasal obstruction (50.0% vs 41.9%). Robey et al 18 reported that the top 3 symptoms of FB were headaches, nasal obstruction, and mucus discharge. Our results agreed with those of previous FB reports.
There was no significant difference in laboratory tests between the 2 groups. In patients with SFB, the incidence of the disease on the left and right sides was close to 1:1, while the most often affected locations of MFBs were bilateral lesions (74.4%). In both groups, the most affected sinuses were maxillary sinus, followed by sphenoid sinus and ethmoid sinus, and sphenoid sinus and ethmoid sinus were more common in MFBs patients, indicating that the lesions in MFBs were more extensive. It should be emphasized that in patients with MFBs, 9 cases were involved ipsilateral maxillary sinus and ethmoid sinus. For the unilateral multiple fungus balls, multiple fungus balls may be spread of a fungus ball to an adjacent sinus. But for bilateral fungus balls, the mechanism is not clear. It is supposed that bilateral fungal balls might represent spread of disease via irrigation or spores spread via breathing. But why don’t the fungus hyphae spread to the ipsilateral near sinuses? Therefore, this hypothesis is not seeming reasonable and further studies are needed to clarify the etiology. The 3 cases of metachronous bilateral MFBs were very interesting. It is a pity that we cannot get all the radiological data to further analyze the 3 cases. One possible hypothesis is that maybe they live in a humid environment and the fungi was easily affecting their sinuses.
Computed tomography is the imaging procedure of choice for the diagnosis of FB. Characteristic findings of FB include complete or partial opacification of the sinus, calcifications, sclerosis, and erosion of the bony walls.19-21 In our study, complete opacification and obstruction of ostiomeatal complex were more common in MFBs patients which we presume may be associated with extensive lesions of MFBs. In anatomy, septal deviation and Haller cells were more common in MFBs patients. We speculate that the complex anatomical relationship leads to the occurrence of MFBs, but further experiments are needed to prove our inference.
For MFBs, we should be aware that some involve continuous sinuses and some involve bilateral sinuses. We should read the CT scans carefully before operation and differentiate it from AFRS (multiple sinuses, high density shadow). Allergic fungal rhinosinusitis associates with multiple, bilateral sinuses, sometimes pansinusitis. In this respect, MFBs is similar with AFRS. However the etiology of FB is different from AFRS. Fungus ball is the collection of fungal hyphae in the sinuses of nonatopic host. But AFRS is recognized as an IgE-mediated type I and type III hypersensitivity to a variety of fungi, eliciting allergic mucosal inflammation in an immunocompetent atopic host. 22 Concomitant allergic diseases such as allergic and asthma usually accompanied with AFRS. Multiple fungus balls occurs in elderly patients, which is different from AFRS, which commonly affects younger individuals. In CT, although the intralesional hyperdensity was very common in both the MFBs and AFRS, actually the intralesional hyperdensity was different. The hyperattenuating of MFBs in CT was fungal hyphae and may demonstrate punctuate calcifications, while the thick, allergic mucin of AFRS showed expansile, hyperattenuating material characteristic within the lumen of the paranasal sinus. 23
The best choice for treatment of FB patients was endoscopic sinus surgery, which could completely clear the FBs and reconstruct the drainage pathway. In our study only one SFB patient recurred and no recurrent MFBs patient was found. Compared with SFB, the operation time of patients with MFBs is relatively longer, and the patients are older and have relatively more concomitant diseases, resulting in higher Caprini score. 24 These are risk factors of deep vein thrombosis and pulmonary embolism, in order to prevent patients from developing the postoperative complication, so surgeons read CT scans carefully, accurately judged MFBs before operation, paid much attention to make sure all the fungus balls removed thoroughly and quickly during the operation, and allowed patients to move as soon as possible after operation. No patient developed venous thrombosis or pulmonary embolism in our study. Surgery technique is another factor to prevent recurrence. Maxillary sinus is the most commonly affected sinuses. Most cases are very easy to manage by a purely endoscopic approach. But for some cases, the lesion located anteriorly and inferiorly in the maxillary sinus, removal of the fungal elements become challenging only with the endoscopic technique. Some literature25,26 suggest Gauze technique or external approach, such as Caldwell-Luc approach, or trans maxillary wall osteoplastic approach to address the most difficult maxillary cases. All our cases were successfully treated with endoscopic approach. According to our experience, after antrostomy we use a malleable angled suction to move the fungus ball from attaching to the anterior or inferior sinus wall and then vigorously irrigate the fungus ball with saline water. Unlike the others using 20 mL syringe, we used a 50 mL syringe connected a cannula to perform the procedure. We think the bigger volume syringe can provide a more high-pressure turbulent flow, and the fungus debris has more chance to be moved out. Our good results may be related to this treatment procedure. This method can also be used to deal with some difficult sphenoid fungus ball cases when the fungus hyphae located laterally to the lateral sphenoid recess.
Conclusion
The incidence of MFSs increased obviously in these years. There were some special entities of MFBs although the symptoms and examination were similar. The older patients were more easily be affected in MFBs. The lesions of MFBs were relatively extensive and the anatomical variation of MFBs patients was complex. Endoscopic surgery could have a good result. The recurrence rate was low and there were no complications. Understanding clinical features of MFBs can help physicians to seek appropriate procedures to manage MFBs.
Footnotes
Authors’ Note
Hui Li and Yu-Xiao Wu contributed equally to this article. Hui Li contributed to conception, data acquisition, interpretation, drafting, revising, approval, and accountable; Yu-Xiao Wu contributed to conception, data acquisition, interpretation, revising, approval, and accountable; Min Wang contributed to conception, revising, approval, and accountable; Zhi-Min Xing contributed to conception, revising, approval, and accountable; Lin Han contributed to conception, revising, approval, and accountable. The study protocol was approved by the Institutional Ethical Committee of Peking University People’s Hospital, and was conducted in accordance with the Helsinki Declaration. All methods were performed in accordance with the guidelines and regulations of the ethical committee. Informed consent was obtained for all patients who participated in the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research and Development Foundation of the People’ Hospital of Peking University (RDB-2015-03), Capital Health Development Foundation (No: 2016-1-2052), and Capital Health Development Foundation (No: 2020-1-2051) supported this study.