
Abstract
Objectives:
Traumatic amputation of the ear constitutes a great aesthetic deformity that can have a tremendous negative impact. Reports describing the survival of near-complete ear amputation using non-microsurgical replantation are scarce. We aimed to study the surgical outcome of patients with near-complete ear amputations supplied by small pedicle bridges that were treated with primary reattachment.
Methods:
We retrospectively studied patients with near-complete ear amputation who were admitted at Al Ain Hospital from January 2016 to December 2019.
Results:
Five patients were studied. The most common mechanism of injury was motor vehicle injury, followed by cutting injury. The skin pedicle was inferior in 3 (60%) patients of patients. The median width of the skin pedicles was 8.5 mm. The median interval between the injury and the surgical management was 4 hours. All patients underwent primary reattachment of the ear without microsurgery. One patient developed a small area of necrosis of the ear lobe. All patients recovered with a completely healed pinna and satisfactory overall appearance.
Conclusions:
Primary reattachment without microsurgery of the near-complete ear amputation can be safely performed in the presence of an intact skin pedicle. It can achieve an aesthetically satisfactory outcome without severe complications.
Introduction
Although relatively uncommon, traumatic ear amputation (EA) constitutes a great aesthetic deformity that can have a tremendous negative impact on the patient’s psychological status. 1 They can be caused by a wide range of mechanisms, including motor vehicle collisions, work-related injuries, and penetrating injuries from assaults, bites, and falls onto sharp objects.2-4 Given the limited evidence base, there is a significant controversy determining a definitive method for repairing near-complete ear amputation (NEA) injuries in an acute setting.
There are different surgical techniques to reconstruct EA ranging from simple reattachment to microsurgical reconstruction of the injured ear.3-5 The decision regarding the proper management should be made at the time of the initial presentation based on the mechanism of trauma, the extent of the injury, the condition of the ear, and the surgeon’s experience.
In the literature, many reported cases of ear avulsions were repaired with microsurgical revascularization. Reports describing the survival of near-complete EA using non-microsurgical replantation are scarce. We aimed to study the surgical outcome of patients with NEA supplied by small pedicle bridges that were treated with primary reattachment.
Methods
This study was approved by Al-Ain Medical District Human Research Ethics Committee, Al-Ain, Abu Dhabi, United Arab Emirates (Ethical Approval Number: AAH/EC-09-20-025).
All patients who had NEA supplied by a narrow pedicle bridge and were admitted to Al-Ain Hospital during the period of January 2016 to December 2019 were retrospectively studied. Written informed consent was obtained from all patients who agreed to publish their clinical data and images.
Al-Ain Hospital is located in the center of Al-Ain city, the largest city in the eastern district of Abu Dhabi Emirate of the United Arab Emirates, with a population of 738 000 inhabitants. 6 It is a university-affiliated hospital which is specialized in acute care and provides expertise in microvascular repair and reconstruction.
A study protocol was designed to collect the required data. Data collected from patients’ records included demography, mechanism of injury, skin pedicle site and width, associated injuries, adjuvant therapy, injury to surgery time, length of hospital stay, complications, follow-up period, and outcome. The collected data were entered into a Microsoft Excel spreadsheet (Microsoft Corporation), and a descriptive statistical analysis was performed.
Results
Presentations
Five patients were retrieved and studied; all were males. The patients had a median (range) age of 34 years (31-50). The most common mechanism of injury was motor vehicle injury (60%) in 3 patients, followed by cutting injury (40%) in 2 patients. On examination, all patients had NEA with a small skin pedicle bridge (Figure 1). The skin pedicle was inferior in 3 patients and superior in 1 patient. One patient had 2 small pedicles located superiorly and inferiorly (Figure 2). The median (range) width of the skin pedicle bridge was 8.5 (5-20) mm. Two patients had an injury to another body region in addition to the ear. One patient had associated injuries to his mandible and chest, and the other had an associated lower limb injury (Table 1).

A 34-year-old man sustained a near-complete left ear amputation attached by a 7-mm skin pedicle after being involved in a motor vehicle collision (A). Five days postprimary reattachment of the ear showing a small area of necrosis of the left ear lobe (B). Two months postoperative follow-up shows a satisfactory clinical outcome.

Preoperative view of a 50-year-old man with a near-complete right ear amputation after being trapped between a piece of heavy machinery and the side rail. The ear was transected across the external auditory meatus and attached on posterior skin (A). The ear appeared well perfused after 7 days of primary reattachment (B). At 2 years postoperative follow-up, healing of the ear was complete, and the patient was aesthetically and functionally satisfied (C).
Patients With Near-Complete Ear Amputations Managed With Primary Reattachment at Al-Ain Hospital During the Period of January 2016 to December 2019.
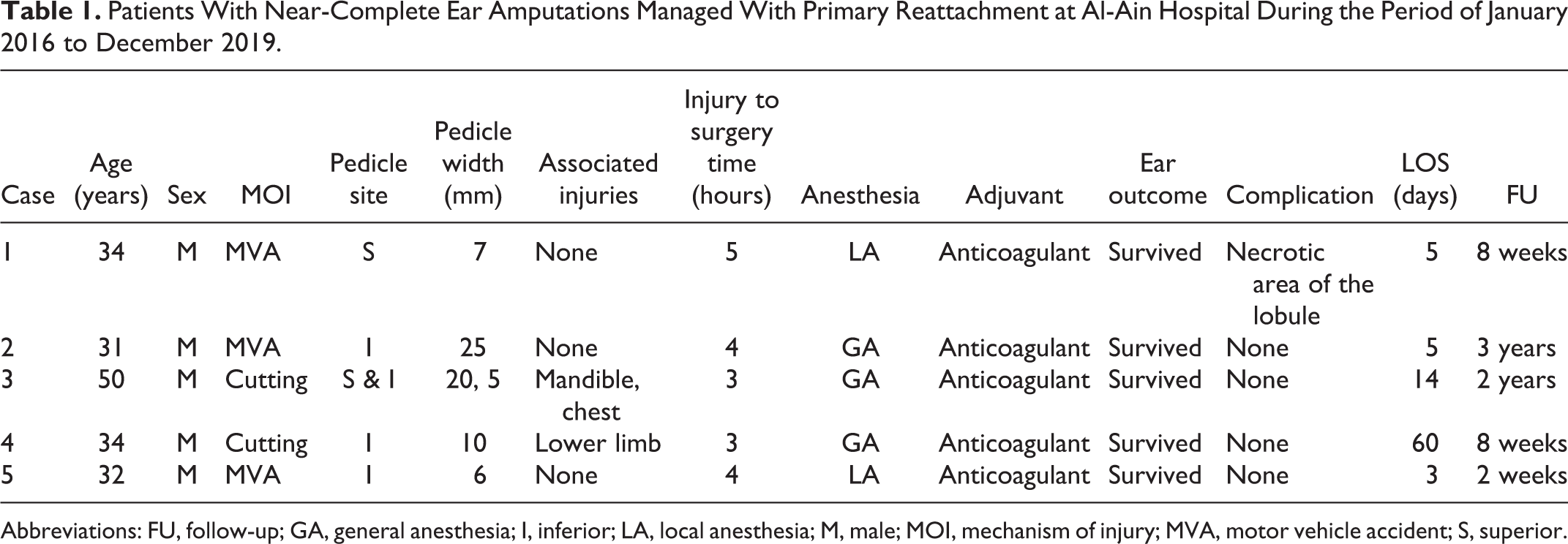
Abbreviations: FU, follow-up; GA, general anesthesia; I, inferior; LA, local anesthesia; M, male; MOI, mechanism of injury; MVA, motor vehicle accident; S, superior.
Management and Outcome
Preoperatively, all patients received intravenous antibiotics (amoxicillin-clavulanate 1000 mg/200 mg twice daily) and tetanus toxoid. The median (range) interval between the injury and the surgical management was 4 (3-5) hours (Table 1). All patients underwent primary reattachment without microsurgery of the ear. Surgical repair was performed under general anesthesia in 3 patients, and local anesthesia with a regional block in 2 patients. Wound margins were meticulously debrided with the use of normal saline and povidone iodine 10%. A 3-layer reattachment of the ear was performed. A 5-0 Vicryl suture was used to repair the cartilage layer, and 4-0 Vicryl Rapide and 5-0 Prolene sutures were used to reattach anterior and posterior skin of the pinna. A head bandage with slight compression was applied after the application of Fucidin ointment to all suture lines.
Postoperatively, all patients received systemic antibiotics and heparin for 5 days. A postoperative complication was noticed in 1 patient who developed a small area of necrosis of the distal portion of the ear lobe, which was debrided and eventually healed by secondary intention (Figure 1). Patients stayed for a median (range) of 5 days (3-60) in the hospital. The median (range) follow-up time was 8 weeks (2 weeks-3 years). Follow-up ear assessment revealed a completely healed pinna with a satisfactory overall appearance in all patients (Figures 1 and 2; Table 1).
Discussion
Traumatic EA is a rare facial trauma. 1 Due to the low frequency and high variability of surgical approaches, determining the best management option can be challenging. Our study has shown that the NEA with an intact small pedicle bridge could entirely survive with a good aesthetic outcome and without significant complications when repaired primarily. To our knowledge, this is the largest reported series of NEAs that were repaired with primary reattachment.
Although a variety of ways exist to approach EA in the acute setting, none appear to have addressed the problem optimally. NEA may require either microsurgical replantation or primary reattachment of the amputated segment.4,5 This is determined by the mechanism of injury, vasculature of the remaining part, and the degree of venous congestion. 7 In an ideal situation, microsurgical anastomosis can be considered the surgical method of choice in delivering the best aesthetic outcomes. However, challenges of finding properly sized vessels and postoperative venous congestion may be encountered.2,8 Furthermore, the technical complexity of microvascular replantation may require specialized expertise and lengthy operative time. With severe crush injuries, microsurgical reconstruction may not be the procedure of choice as the ear’s skin, and cartilage can be severely destroyed. As a result, the vessels are damaged and unsuitable for revascularization. Microvascular repairs are appropriate in clear-cut ear injuries with short ischemic interval and identified vessels for anastomosis.4,8,9 As no suitable vessels were identified on our patients’ initial examination; the microsurgical repair was not attempted. In cases where the amputated part is not suitable for replantation, other salvage approaches have been described, such as banking of the de-epithelialized auricular cartilage followed by delayed replantation, 10 local flap coverage, 11 and secondary reconstruction with rib cartilage. 12 Several features of the auricle are attributed to the high survival rate of the amputated ear. These include a low metabolic rate of the ear cartilage and easily formed new blood vessels from the highly vascularized facial soft tissue. 11
Primary reattachment is the most straightforward technique that requires short operative time and minimal hospital stay. In our patients, the finding of an intact skin pedicle, good skin color, and active bleeding points has suggested good blood circulation of the ear and strengthened our confidence in utilizing the primary reattachment technique.
Direct reattachment of the NEA is possible with a good result when the injury involves trauma due to a sharp cut.3,5,13 Conversely, very few successful repairs are described in total EA, which usually ends up with necrosis and loss of the attached segment. 1 In contrast to others,3,5 the most common mechanism of injury in our study was motor vehicle injury, followed by cutting injury (Table 1).
Understanding the vascular anatomy of the auricle is crucially important when deciding the best reconstructive approach. The auricle is supplied by an interconnection of arterial branches originating from the superficial temporal artery (STA) and the posterior auricular artery (PAA). 7 The upper auricular branch of STA communicates with the posterior vasculature by supplying the arterial arcade along the helical rim. 5 This feature gives the ear the possibility to survive based on a single-arterial pedicle. Venous drainage of the external ear, analogous to the arteries, is via the superficial temporal and posterior auricular veins into the retromandibular and external jugular veins, respectively. 14
In our series, all ears survived on small skin pedicle with a width ranging between 5 and 20 mm. Based on previously published reports, the width of the skin pedicle in a successfully repaired NEA with primary reattachment ranged from 3 mm to 30 mm with almost equally reported cases with superior and inferior skin pedicles.15,16 The anatomic study by Erdmann et al 5 showed that the preserved superior branch of STA in the skin pedicle at the helical root supplied the entire ear and resulted in its survival. Park et al 7 noted better chances for ear survival when the PAA, which has the most significant impact on auricular blood flow, is preserved at the ear’s posterior aspect. They have also noted that the ear lobe consistently contained a perforator from PAA. 7
We think that the arterial support in case 1 has been provided by the superior branch of STA and in the other 4 cases by the lower branch of STA and perforators from PPA. The ischemic intervals were short. The mean interval between the injury and the surgical management was 4 hours (Table 1).
General anesthesia was the preferred type of anesthesia to reconstruct the ear in our patients (Table 1). Similarly, most of the previously reported cases of NEA were repaired with general anesthesia.2,3,17,18 Local anesthesia must be used cautiously in these patients as it can increase edema at the pedicle site and can potentially damage the vessels.13,9
A variety of adjunct postoperative therapies have been applied to augment tissue perfusion and survival but with no consensus on the preference of one therapy concept over the other. These therapies included the administration of anticoagulants, Aspirin, Dextran-40, Vitamin E, local hypothermia, leeches, and hyperbaric oxygen therapy (HBOT).9,16,18,19 The most common applied adjunct therapies were anticoagulants, followed by leeches and HBOT.9,17,19 Similar to others,9,17 we have administered anticoagulants in all patients to promote venous outflow (Table 1). Leeches, alone or in combination with other anticoagulants, are commonly used by many surgeons after ear replantation to relieve venous congestion, especially when a microsurgical venous anastomosis could not be achieved.5,19 Although its exact mechanism of action is still not clear, HBOT has been shown to increase neovascularization and stimulate granulation tissue formation. This treatment has been utilized successfully to minimize necrosis of pedicled flaps. 20
The most commonly reported complications after primary reattachment of NEAs in the literature were venous congestion, followed by necrosis of the lobule and necrosis of helical root.2,5,19 As shown in Table 1, in this study, 1 patient developed a small necrotic area of the ear lobe. This was debrided and eventually healed by secondary intention. All patients achieved satisfactory surgical and aesthetic outcomes.
We have to acknowledge that our study is a single-institution study with small sample size. Given the rarity of these injuries, this manuscript is unique in its nature as it is the largest reported series of NEAs that were repaired with primary reattachment.
Conclusions
The decision regarding the proper surgical approach to manage the NEA should be made at the time of the initial presentation. Primary reattachment without microsurgery of the NEA can be safely performed in the presence of an intact skin pedicle. It requires shorter operative time and can achieve an aesthetically satisfactory outcome without severe complications. Conducting a larger multicentric study could help defining the indications for primary reattachment or microsurgery. Our conclusions are based on our personal experience and the available literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.