
Abstract
Objectives:
Alteration of smell and taste has been reported in patients with coronavirus disease 2019 (COVID-19). The incidence and clinical-symptomatic manifestation of COVID-19 is different between northern and southern Italy. This study aims to evaluate the onset of alteration of smell and taste in asymptomatic and symptomatic patients in Sicily (extreme south of Italy).
Methods:
This prospective cross-sectional study was performed on asymptomatic and symptomatic COVID-19 patients tested for severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) from May 1 to May 15, 2020. A questionnaire was used for evaluating the prevalence of smell and taste disorders in COVID-19 patients before performing nasopharyngeal swab.
Results:
Of the total 292 patients, 242 (83.2%) were negative for SARS-CoV-2 and 50 were positive (16.8%). Twenty-six of the 50 (52%) SARS-CoV-2 positive patients reported smell/taste disorders. Twenty-eight of the 50 (57.1%) SARS-CoV-2 positive patients were hospitalized (group A), and 22 (42.9%) were nonhospitalized (group B). The mean age in group A and group B was 45.4 ± 13.7 years and 57.0 ± 15.0, respectively (P = .007). The symptoms reported by hospitalized patients were fever (71.4%), cough (64.2%), fatigue (82.1%), and dyspnea (100%), while in nonhospitalized patients, the most reported symptoms were sore throat (72.7%), rhinorrhea (77.2%), and altered smell (81.8%). Anosmia/hyposmia reported in group A and group B was 28.5% and 81.8%, respectively (P = .001).
Conclusion:
These preliminary results indicate that the majority of SARS-Cov-2 positive patients in southern Italy did not require hospitalization and presented with milder symptoms or no symptoms and the alterations in smell and taste occurred.
Introduction
The epidemic, coronavirus disease 2019 (COVID-19) that appeared in December 2019 in the city of Wuhan, China, as atypical pneumonia, is caused by a novel coronavirus called severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). 1 The infection rapidly spread from China affecting the whole world, which was declared as global pandemic by the World Health Organization in March 2020. In Italy, the spread of the disease had a very different trend based on the population in north and south. According to a recent report, 2 the weekly incidence reported on May 5, 2020, was 19.07 in Italy, but the average incidence in the regions of central and northern Italy reached an average of 39.5, while in the south and islands, the average was 2.28. The rapid spread of COVID-19 pandemic is mainly related to the mode of transmission through respiratory droplets. The disease may present with flu-like symptoms characterized by cough, fever, chills, sore throat, or with more severe symptoms such as shortness of breath or difficulty in breathing, nausea, vomiting, or diarrhea, and most cases can be asymptomatic. Symptoms related to the alteration of smell and taste in COVID-19 patients have not been reported from China, where the disease originated. Smell disorders in COVID-19 were initially reported as case reports. 3 Bagheri et al, 4 for the first time, reported that the symptoms of smell and taste alterations in Iranian patients with COVID-19 could show up early. In Italy, in addition to the variations in the spread of the pandemic, the symptomatological manifestation may also have been different. Of the total patients hospitalized, patients admitted to intensive care units in each Italian region at the end of April 2020 showed differences in the incidence of alteration of smell and taste ranging from 5.04% to 20.7%, 2 with higher values observed in the regions of northern Italy. The studies conducted so far in Italy on the onset of symptoms of smell and taste alterations are mainly reported in the northern Italian population. 5,6 Since the course of the disease has shown a difference in terms of incidence and clinical-symptomatic manifestation between northern and southern Italy, this study aims to evaluate the appearance of alteration of smell and taste in asymptomatic and symptomatic patients in Sicily (extreme south of Italy).
Materials and Methods
This prospective cross-sectional study was performed with COVID-19 asymptomatic and symptomatic patients, submitted to a nasopharyngeal swab for SARS-CoV-2 from May 1 to May 15, 2020. Patients were recruited from the Otolaryngology Unit and Infectious Disease Unit of Cannizzaro Hospital, Catania and Public health, Epidemiology and Preventive Medicine, ASP Trapani, Italy. The exclusion criteria were age <18 years, physical or cognitive inability to cooperate, patients admitted to intensive care units, patients with a previous history of hypo/anosmia or taste disturbances. A questionnaire was used for evaluating the prevalence of smell disorders in the context of SARS-CoV-2 infection using the questions included in the COVID-19 Anosmic Reporting Tool of the American Academy of Otolaryngology Head and Neck Surgery, 7 (supplemental materials) which was translated into Italian (See Supplemental Material online). This questionnaire was administered by a physician before performing the nasopharyngeal swab. Severe acute respiratory syndrome-coronavirus-2 infection was diagnosed with a positive reverse transcription-polymerase chain reaction test. Demographic and clinical data were collected anonymously together with the relative responses from a specific database. The study was performed according to the Guidelines for Biomedical Studies Involving Human Subjects (Helsinki Declaration). All patients provided written informed consent. According to the institutional review board of the University of Catanzaro, Italy, this study was exempt from ethical committee approval because the study was based on anonymized data.
Statistical Analyses
Statistical analyses were performed with MedCalc software using the chi-square test and Fisher’s exact test. Correlations between the groups and clinical data were examined with the Mann-Whitney U test. A P value of <.05 was considered statistically significant.
Results
Overall, 434 patients were recruited; 142 were excluded for incomplete questionnaire. Finally, 292 patients with an average age of 47.6 ± 13.7 years were included in the study, with 180 men (61.6%) and 112 women (38.4%). While performing the nasopharyngeal swab, 241 (82.5%) patients were asymptomatic and 51 (17.4%) symptomatic. Thirty-nine patients (13.4%) were hospitalized, and 253/292 (86.6%) were nonhospitalized. Of the 253 nonhospitalized patients, 52 were quarantined, 48 were health workers, and 153 patients, defined as not at risk, underwent nasopharyngeal swab for different reasons (hospitalization for other causes, outpatient visit). Of the total of 292 patients, 242 (83.2%) were negative for SARS-CoV-2, and 50 were positive (16.8%). Twenty-six of the 50 (52%) SARS-CoV-2 positive patients reported smell/taste disorders. Twenty-eight of the 50 (57.1%) SARS-CoV-2 positive patients were hospitalized (group A), and 22 (42.9%) were nonhospitalized (group B). The mean age in group A and group B was 45.4 ± 13.7 years and 57.0 ± 15.0, respectively (P = .007). The univariate analysis did not reveal any other significant differences in the anamnestic and clinical characteristics between the 2 groups of patients (Table 1).
Anamnestic and Clinical Characteristics of Group A and Group B.a
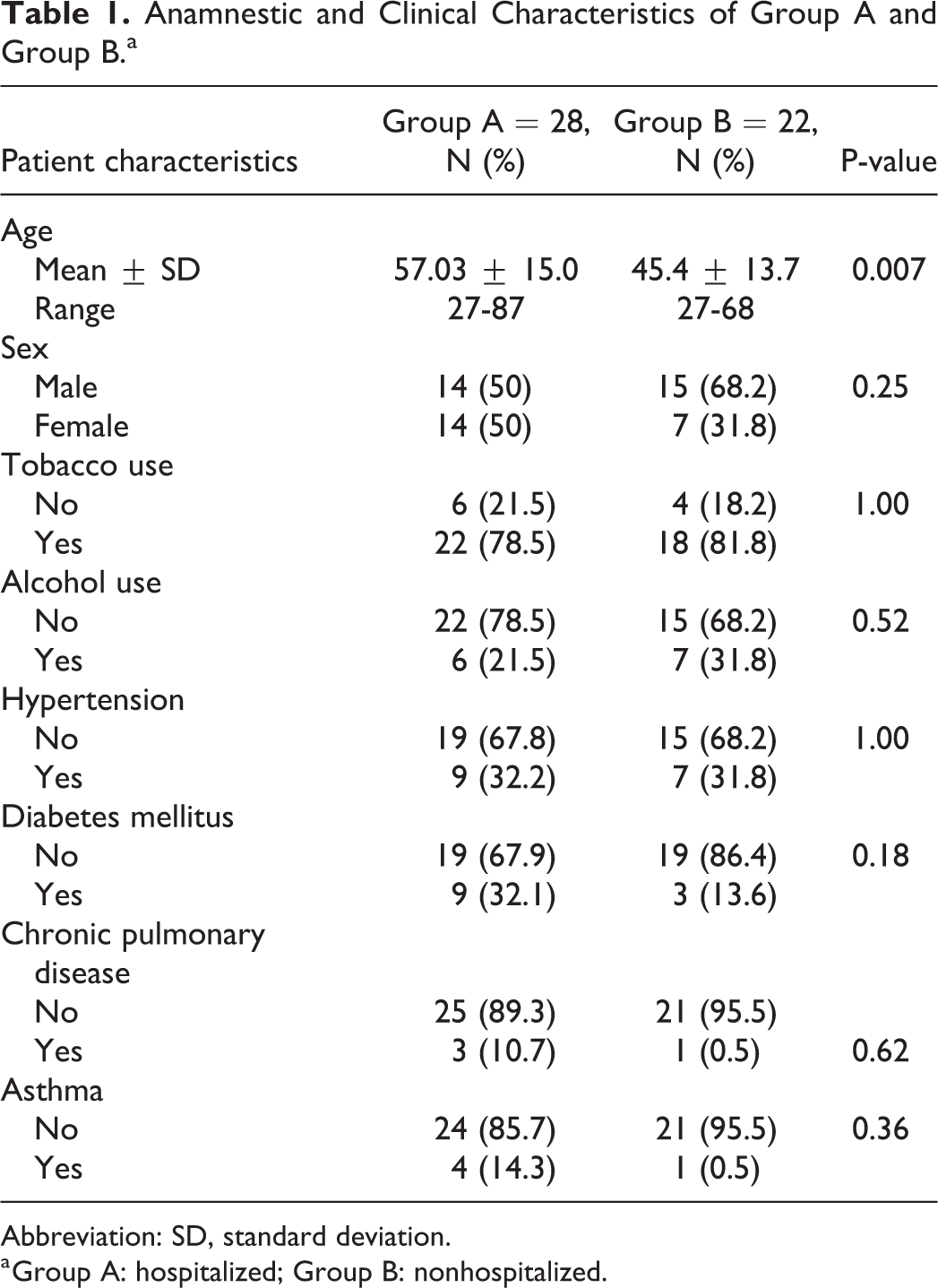
Abbreviation: SD, standard deviation.
a Group A: hospitalized; Group B: nonhospitalized.
The symptoms most reported by hospitalized patients were fever (71.4%), cough (64.2%), fatigue (82.1%), and dyspnea (100%), while in the group of nonhospitalized patients, the most reported symptoms were sore throat (72.7%), rhinorrhea (77.2%), and altered smell (81.8%). Anosmia/hyposmia reported in group A and group B was 28.5% and 81.8%, respectively (P = .001).
The univariate analysis showed a statistically significant difference between the 2 groups in relation to the symptoms of fever, dyspnea, and fatigue, mostly reported in group A, while rhinorrhea, alteration of smell and taste were significantly reported in group B (Table 2).
Self-Reported Symptoms of the 2 Groups of SARS-CoV-2 Positive Patients.a
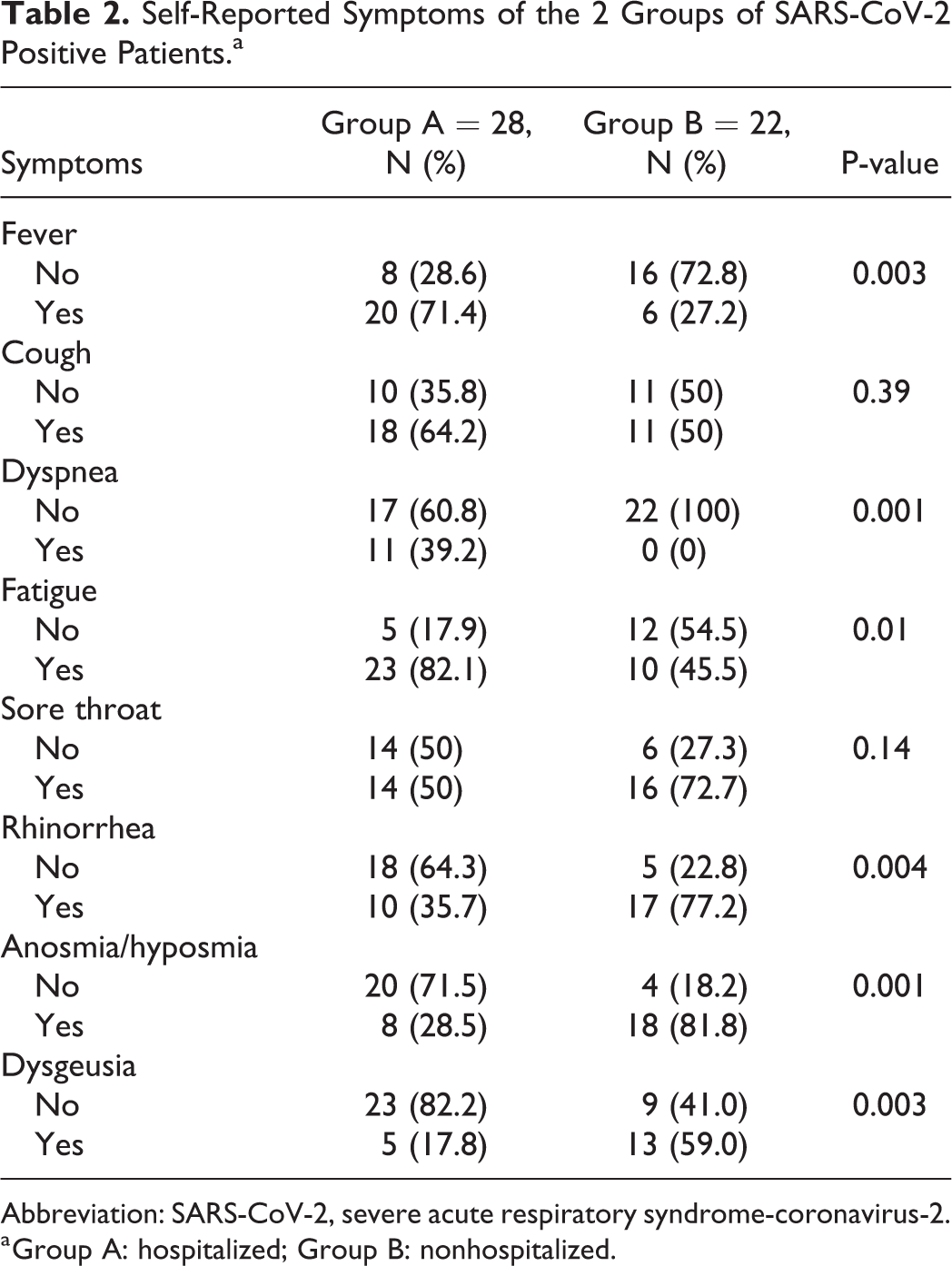
Abbreviation: SARS-CoV-2, severe acute respiratory syndrome-coronavirus-2.
a Group A: hospitalized; Group B: nonhospitalized.
The multivariate analysis showed that age was the only predictive factor associated with hospitalization (P = .018). Considering the alteration of the sense of smell, the multivariate logistic analysis showed that the alteration of the taste was significantly associated with the smell disorders (P = .002). An inverse correlation was instead found between alteration of the sense of smell and hospitalization status (P = .015).
Discussion
Our study considered asymptomatic and symptomatic patients who underwent nasopharyngeal swab for SARS-CoV-2. The preliminary results showed that 16.8% of all examined patients tested positive for SARS-CoV-2; this result reflects the epidemiological data on the spread of the pandemic in Sicily. Of the SARS-CoV-2 positive patients, 52% had smell/taste disorders, and 81.8% of them were not hospitalized. Hospitalized patients presented mainly fever, fatigue, and dyspnea. In the nonhospitalized group, the most frequent symptomatology was the alteration of the sense of smell, rhinorrhea, and dysgeusia. Regarding the prevalence of disorders of smell and taste in Europe, a multicenter study 8 conducted on a total of 417 hospitalized or quarantined patients found smell/taste disorders in 85.6% of cases. Giacomelli et al 5 conducted a study on 59 patients affected by COVID-19 and hospitalized in the “Sacco” hospital in Milan, Italy, of which 33.9% were affected by smell/taste disorders, and 72.8% of them had an atypical pneumonia. From a recent study by Paderno et al, 6 in a total of 508 positive SARS-CoV-2 patients with 58% of hospitalized patients and 42% of quarantined patients, a prevalence of smell and taste disorders were detected in 73.4% of hospitalized patients and in 93.1% of nonhospitalized patients. Our results are similar to those reported by Paderno et al, 6 probably because the sample of SARS-CoV-2 positive patients is very similar to ours, consisting of a similar percentage of hospitalized and nonhospitalized patients. Recently, Yan et al 9 reported that hospitalized patients with COVID-19 are 10 times less likely to report hyposmia/anosmia than SARS-CoV-2 positive outpatients. This would confirm the earliness of the onset of smell and taste disorders in nonhospitalized COVID-19 patients, where the prevalence of these symptoms is more significant than that in hospitalized patients with more serious symptoms. Moreover, the sense of smell and taste disorders was also reported in several patients hospitalized in intensive care units or with infectious diseases, but the severity of the symptomatology that occurred subsequently influenced the answers given by the patient on the previous symptomatology. The data collected in Italy on the smell/taste symptomatology in patients affected by the COVID-19 are few and concern the population of northern Italy. This can be attributed to the variations in the geographical spread of COVID-19 infection in Italy. Recently, Adorni et al 10 conducted a study on nonhospitalized Italian patients and found that participants in a web-based survey on self-reported symptoms of COVID-19 infection were mostly from northern regions. This reflects the higher incidence of COVID-19 outbreak in the northern regions than in the southern regions. In addition to the higher incidence of the spread of infection in the regions of northern Italy, an increase in mortality owing to COVID-19 was observed. Stortichini et al 11 found an increase in mortality attributable to COVID-19 infection in some northern provinces that was 400% greater than the rest of country. Mortality rates were lower in central Italy and minimal or absent in the south and the islands. The different spread of the infection between the north and south could be attributed to different climatic and socioeconomic conditions. Cai et al 12 reported an association between the SARS-CoV-2 outbreak and metrological factors, including temperature, humidity, wind velocity, and air pollution. Higher temperature and humidity reduce SARS-CoV-2 transmission rate owing to their impact on the viral growth rate. 13,14 The higher relative humidity and high wind velocity decrease the suspending time of the viruses in the air. In the southern regions, the weather is warmer, and there are more sunny days during the year than in the northern regions; therefore, the exposure to the ultraviolet light is higher. It is known that the ultraviolet light promote vitamin D production, which through several mechanisms increases the immune system and reduces the risk of virus infections. 15 For this reason, the southern population could acquire an immune resistance to the SARS-CoV-2. 16 In contrast, the northern regions of Italy present a socioeconomic contest, with industrialization and urbanization favoring air pollution. In these conditions, the air is less rarefied and can contribute to the persistence of the droplets of SARS-CoV-2 in the air. 16 For these reasons, both the type and severity of the symptoms could be different in different regions of Italy. Our study is still ongoing, and there are several hypothesis for the interpretation of this data. It is possible that in patients who regain a sense of smell, an antibody response develops early, which avoids the patient’s more serious symptomatology that requires hospitalization. However, a lack of objective olfactory testing represents a limitation of our study and further studies have been done to confirm this our hypothesis.
Conclusion
In summary, these preliminary results indicate that the majority of SARS-Cov-2 positive patients in Sicily did not require hospitalization were presenting with milder symptomatology, and the disturbances of smell and taste represent prodromal symptoms of the infection.
Supplemental Material
Supplemental Material, sj-doc-1-ear-10.1177_0145561320981447 - Alteration of Smell and Taste in Asymptomatic and Symptomatic COVID-19 Patients in Sicily, Italy
Supplemental Material, sj-doc-1-ear-10.1177_0145561320981447 for Alteration of Smell and Taste in Asymptomatic and Symptomatic COVID-19 Patients in Sicily, Italy by Maria Rita Bianco, Domenico M. Modica, Gaetano D. Drago, Alfio Azzolina, Gianfranco Mattina, Massimo De Natale, Giuseppe Rossi, Marta Amata, Gaspare Canzoneri, Giovanni Manganaro, Francesco Di Gregorio, Rosario Russo, Salvatore Pricoco, Vincenzo Saita and Eugenia Allegra in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.