
Abstract
Objectives:
In the present report, we aimed to investigate the impact of the coronavirus disease (COVID-19) pandemic on vertigo/dizziness outpatient cancellations in Japan.
Methods:
We examined 265 vertigo/dizziness outpatients at the ear, nose, and throat department of the Nara Medical University between March 01, 2020, and May 31, 2020, during the COVID-19 pandemic in Japan. We also focused on 478 vertigo/dizziness outpatients between March 01, 2019, and May 31, 2019, before the COVID-19 pandemic, to compare the number of cancellations between these 2 periods. The reasons for cancellation and noncancellation were investigated using telephone multiple-choice questionnaires (telMCQs), particularly for patients with benign paroxysmal positional vertigo (BPPV) and Meniere’s disease (MD).
Results:
There were many cancellations for medical examinations during the 2020 study period. The total number of vertigo/dizziness outpatients decreased by 44.6% in the 2020 period compared to the same period in 2019. The percent reduction in clinic attendance from 2019 to 2020 (ie, [2019-2020]/2019) for patients with BPPV was higher than that for patients with MD. Compared to the other vertigo-associated conditions, patients with MD exhibited a lower percent reduction in clinic attendance. According to the results of the telMCQs, 75.0% of BPPV cases and 88.2% of MD cases cancelled their appointment and gave up visiting hospitals due to fear of COVID-19 infection, even if they had moderate to severe symptoms. On the contrary, 25.0% and 80.0% patients with BPPV and MD, respectively, did not cancel their appointment; they should not have visited the hospital but stayed at home because they had slight symptoms.
Conclusions:
These findings suggest that advanced forms should be prepared for medical care, such as remote medicine. These forms should not only be for the disease itself but also for the mental distress caused by persistent symptoms.
Keywords
Introduction
The coronavirus disease (COVID-19) pandemic began in Wuhan, China, in December 2019, and the outbreak has rapidly spread worldwide. The first Japanese patient tested positive for COVID-19 in Nara prefecture on January 28, 2020. The patient was a tour bus driver and took Chinese tourists from Wuhan for sightseeing. The World Health Organization (WHO) declared COVID-19 to be a pandemic in March 2020. 1,2 Owing to the high risk of exposure and infection to COVID-19 from aerosol and droplet contamination, the current COVID-19 pandemic leads to a significant occupational hazard for physicians and paramedical staff. 3 -11 Particularly, the physicians and paramedical staff in the ear, nose, and throat (ENT) department are always at risk of being exposed to outpatients with nasal and/or respiratory symptoms due to COVID-19. The same risk can presumably be applied to the patients. Outpatients with vertigo/dizziness who are COVID-19 negative may be infected by nose and throat patients who have COVID-19 at the same outpatient clinic. In the present report, we investigated the impact that the COVID-19 pandemic has had on vertigo/dizziness outpatient cancellations in Japan.
Methods
This clinical study was registered with the UMIN clinical trials registry (identification number: 000018399) and was approved by the Ethics Committee of the Nara Medical University (identification number: 0889).
Patients
We retrospectively examined 265 vertigo/dizziness outpatients at the ENT department of Nara Medical University between March 1, 2020, and May 31, 2020, during the COVID-19 pandemic in Japan. We also focused on 478 vertigo/dizziness outpatients between March 1, 2019, and May 31, 2019, prior to the COVID-19 pandemic, to compare the number of cancellations between these 2 periods. Patients who had already been diagnosed with a disorder resulting in vertigo/dizziness and were scheduled to attend follow-ups during the above study periods were enrolled. Patients attending for an initial assessment were excluded. “Cancellation” in the present study indicates that a patient with a prior diagnosis who had made a reservation for their next ENT visit to the hospital chose to cancel that reservation. “Non-cancellation” meant that a patient with a prior diagnosis who had made a reservation for their next ENT visit to the hospital attended that reservation.
In accordance with the diagnostic guidelines of the International Classification of Vestibular Disorders 2015, all the enrolled patients were definitively diagnosed with benign paroxysmal positional vertigo (BPPV), Meniere’s disease (MD), vestibular neuritis (VN), sudden deafness with vertigo (SDV), or orthostatic dysfunction (OD). 12 -16 If necessary, these patients received various kinds of vertigo/dizziness examinations, including the caloric test, vestibular evoked cervical myogenic potentials, subjective visual vertical assessment, inner ear magnetic resonance imaging, the Schellong test, and self-rating questionnaires for depression as described previously. 17,18 After careful interviewing and examinations, patients with dizziness of unknown origin were classified into unknown (UK).
Questionnaires
During the study period between March 1, 2020, and May 31, 2020, the telephone reservation center at the Nara Medical University called all patients to determine their cancellation or noncancellation intentions as a result of the COVID-19 situation in the Nara Prefecture. This system was not enforced by law but had been recommended as an aid to patients to help them make decisions regarding attendance during that period.
After the Japanese government ended the emergency declaration in June 2020, the reasons for cancellation (Table 1A) and noncancellation (Table 1B) were investigated by means of telephone multiple-choice questionnaires (telMCQs), especially in patients with BPPV and MD at the ENT department. Among the diseases that cause vertigo/dizziness, BPPV, and MD are the most common ailments. Benign paroxysmal positional vertigo does not show progressive or irreversible symptoms, while MD can cause recurrent vertigo attacks and fluctuating/progressive sensorineural hearing loss.
Telephone Multiple-Choice Questionnaires (telMCQs) of Cancellation (A) and Noncancellation (B) to Visit Hospitals.
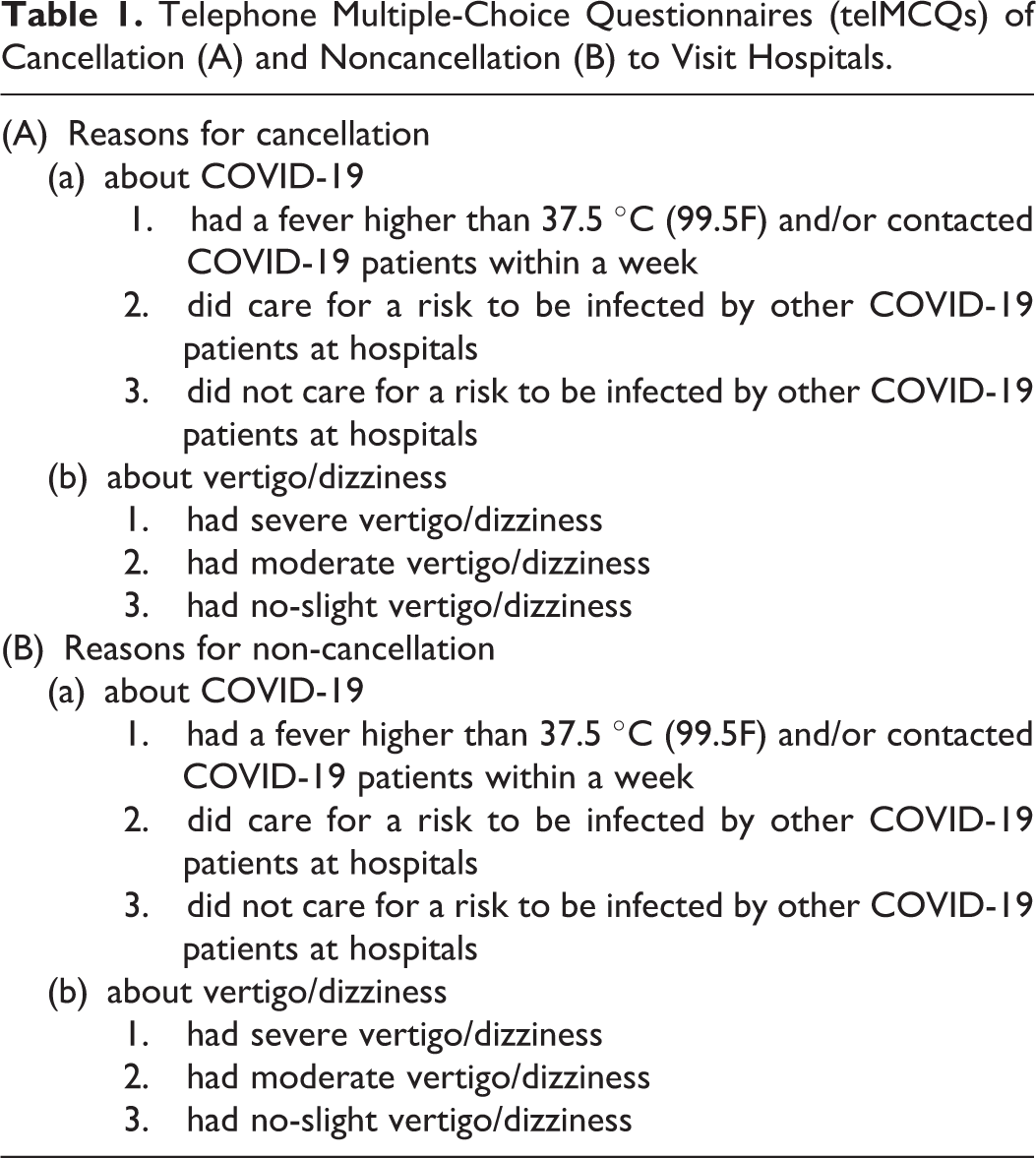
The telMCQs addressed the reasons for cancellation or for noncancellation. For both, the questions asked were concerned with the current COVID-19 pandemic (questions a-1,2,3) and their vertigo/dizziness symptoms (questions b-1,2,3). Each cancellation or noncancellation for a patient with either BPPV or MD was picked up randomly from the smaller medical record number until 20 cases were collected.
Statistical Analyses
Chi-square tests were used to determine significant differences between the outpatients’ backgrounds during the 2019 and 2020 study periods. The Kruskal-Wallis and paired t tests were performed to examine significant differences between the changes in the percent reduction in clinic attendance in 2020 compared to the same period during the previous year (ie, [2019-2020]/2019) for various types of vertigo/dizziness diseases. All reported P values were 2-sided, and those under 0.05 were considered significant. All statistical analyses were performed using SPSS version 18.0 (SPSS Inc).
Results
Of the 478 vertigo/dizziness outpatients between March 1, 2019, and May 31, 2019, 210 (43.9%) had BPPV, 143 (29.9%) had MD, 34 (7.1%) had VN, 20 (4.2%) had SDV, 14 (2.9%) had OD, 44 (9.3%) had others, and 13 (2.7%) were UK (Figure 1A). Of the 265 vertigo/dizziness outpatients between March 1, 2020, and May 31, 2020, 76 (28.7%) had BPPV, 121 (45.7%) had MD, 22 (8.3%) had VN, 13 (4.9%) had SDV, 7 (2.6%) had OD, 20 (7.5%) had others, and 6 (2.3%) were UK (Figure 1B). The total number of vertigo/dizziness outpatients decreased by 44.6% in the 2020 period compared to the same period in 2019. The percent reduction in clinic attendance from 2019 to 2020 due to cancellation was as follows: BPPV ([210-76]/210: 63.8%), MD ([143-121]/143: 15.4%), VN ([34-22]/34: 35.3%), SDV ([20-13]/20: 35.0%), OD ([14-7]/14: 50.0%), others ([44-20]/44: 54.5%), and UK ([13-6]/13: 53.8%).
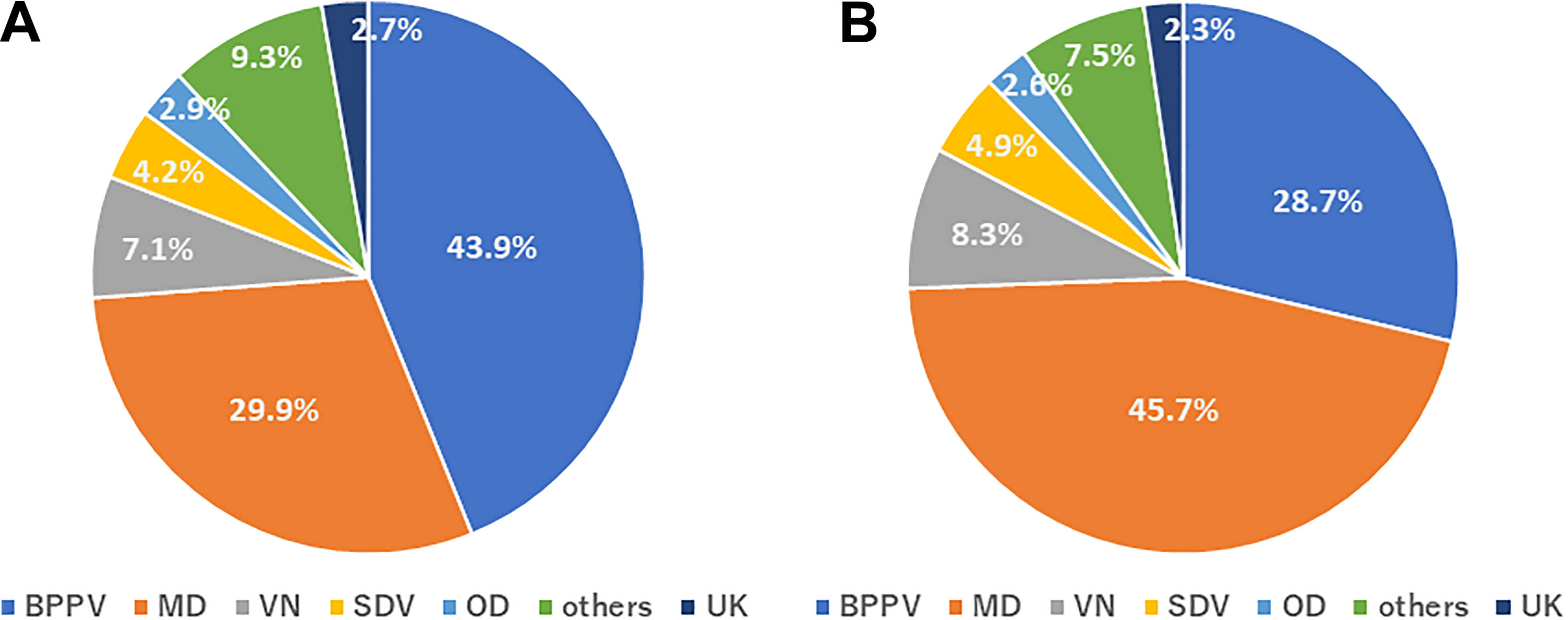
The ratios of vertigo/dizziness outpatients with benign paroxysmal positional vertigo (BPPV), Meniere’s disease (MD), vestibular neuritis (VN), sudden deafness with vertigo (SDV), orthostatic dysfunction (OD), others, and unknown (UK) cause at the ear, nose, and throat (ENT) department in 2019 (nonpandemic) and in 2020 (COVID-19 pandemic). (A) The disease percentages for 478 vertigo/dizziness outpatients between March 1, 2019, and May 31, 2019. (B) The disease percentages for 265 vertigo/dizziness outpatients between March 1, 2020, and May 31, 2020.
The percent reduction in clinic attendance for patients with BPPV was higher than for those with MD. Compared to the other vertigo-associated conditions, patients with MD exhibited a lower percent reduction in clinic attendance from 2019 to 2020 (Figure 2).
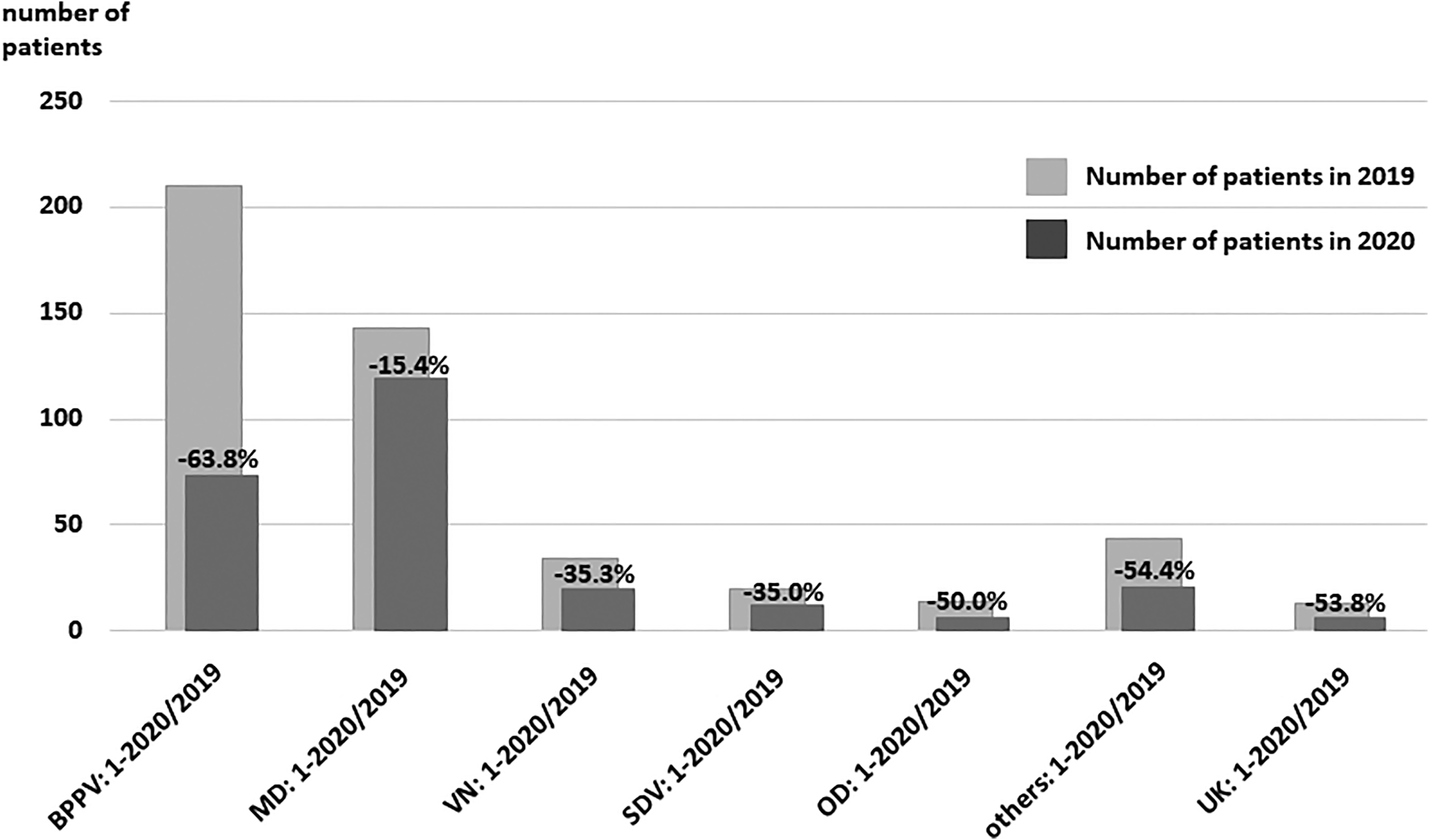
The percent reduction in clinic attendance for different vertigo/dizziness diseases from 2019 (nonpandemic) to 2020 (COVID-19 pandemic). Percent reduction in clinic attendance for different vertigo/dizziness diseases from 2019 to 2020 ([2019-2020]/2019) were as follows: BPPV ([210-76]/210: 63.8%), MD ([143-121]/143: 15.4%), VN ([34-22]/34: 35.3%), SDV ([20-13]/20: 35.0%), OD ([14-7]/14: 50.0%), others ([44-20]/44: 54.5%), and UK ([13-6]/13: 53.8%). BPPV indicates benign paroxysmal positional vertigo; MD, Meniere’s disease; OD, orthostatic dysfunction; SDV, sudden deafness with vertigo; UK, patients with dizziness of an unknown origin were classified as unknown; VN, vestibular neuritis.
With regard to the telMCQs, no patients with BPPV or MD cancelled because of (a-1) a fever higher than 37.5 °C (99.5 °F) and/or because they had contracted COVID-19 within one week before they were meant to attend the hospital. The reasons for cancellation for patients with BPPV (n = 20) were as follows: n = 2 for a-2-b-1, n = 10 for a-2-b-2, n = 4 for a-2-b-3, n = 0 for a-3-b-1, n = 1 for a-3-b-2, and n = 3 for a-3-b-3. Those with MD (n = 20) cancelled for the following reasons: n = 6 for a-2-b-1, n = 9 for a-2-b-2, n = 2 for a-2-b-3, n = 0 for a-3-b-1, n = 1 for a-3-b-2, and n = 2 for a-3-b-3 (Figure 3A). The reasons for noncancellation for patients with BPPV (n = 20) were as follows: n = 12 for a-2-b-1, n = 4 for a-2-b-2, n = 0 for a-2-b-3, n = 1 for a-3-b-1, n = 3 for a-3-b-2, and n = 0 for a-3-b-3. The reasons those with MD (n = 20) did not cancel were as follows: n = 3 for a-2-b-1, n = 10 for a-2-b-2, n = 2 for a-2-b-3, n = 2 for a-3-b-1, n = 2 for a-3-b-2, and n = 1 for a-3-b-3 (Figure 3B).
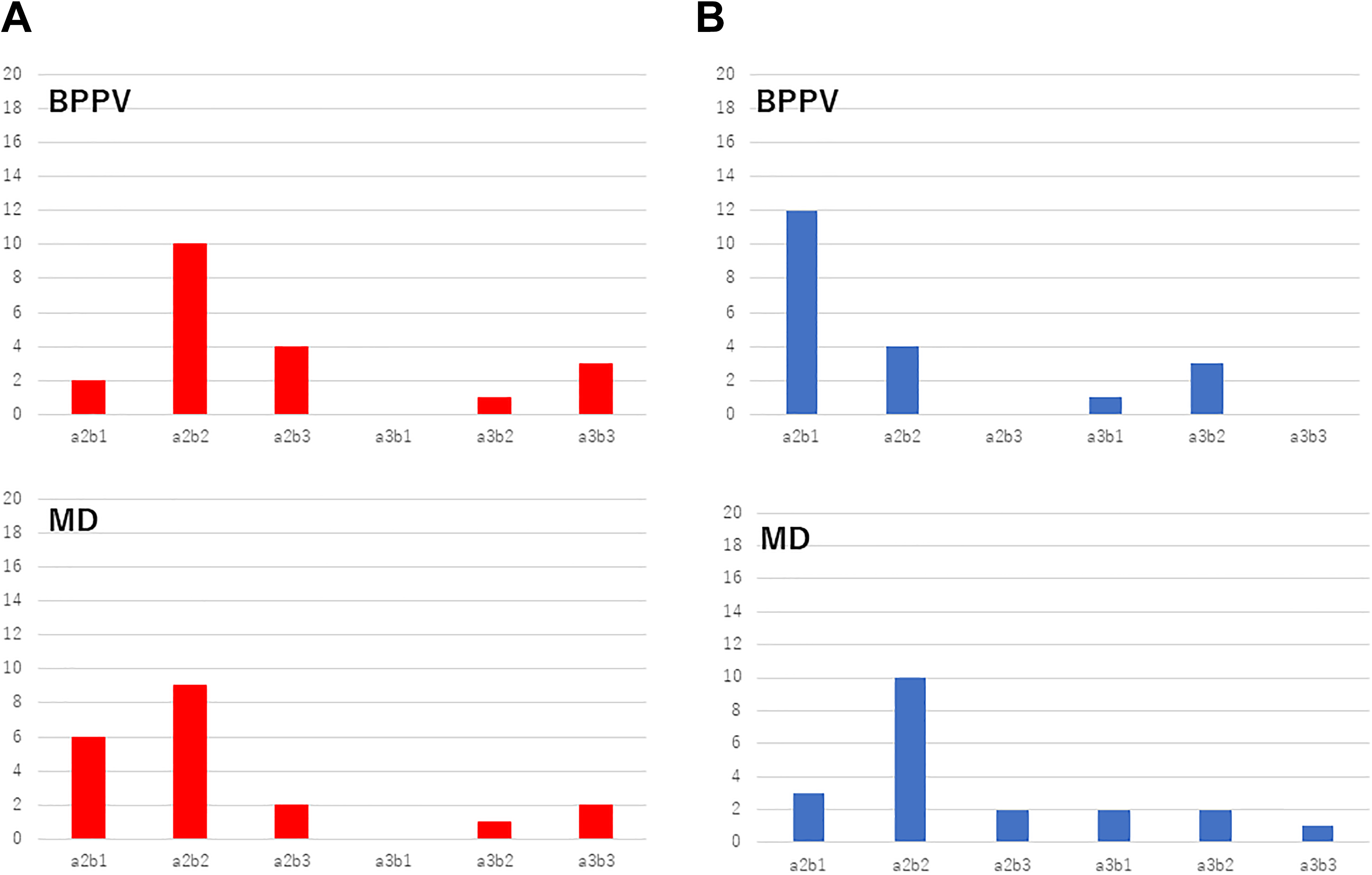
Results of the telephone multiple-choice questionnaires (telMCQs) regarding the reason for cancellation or noncancellation in patients with benign paroxysmal positional vertigo (BPPV) or Meniere’s disease (MD). (A) There were no patients with BPPV or MD belonging to a-1 in the present study. The reasons for cancellation for BPPV patients were as follows: n = 2 for a-2-b-1, n = 10 for a-2-b-2, n = 4 for a-2-b-3, n = 0 for a-3-b-1, n = 1 for a-3-b-2, and n = 3 for a-3-b-3. The reasons patients with MD cancelled were as follows: n = 6 for a-2-b-1, n = 9 for a-2-b-2, n = 2 for a-2-b-3, n = 0 for a-3-b-1, n = 1 for a-3-b-2, and n = 2 for a-3-b-3. (B) There were no patients with BPPV or MD belonging to a-1 in the present study. The reasons for noncancellation for patients with BPPV were as follows: n = 12 for a-2-b-1, n = 4 for a-2-b-2, n = 0 for a-2-b-3, n = 1 for a-3-b-1, n = 3 for a-3-b-2, and n = 0 for a-3-b-3. The reasons those with MD did not cancel were as follows: n = 3 for a-2-b-1, n = 10 for a-2-b-2, n = 2 for a-2-b-3, n = 2 for a-3-b-1, n = 2 for a-3-b-2, and n = 1 for a-3-b-3. There were no patients with BPPV or MD who had a fever higher than 37.5 °C (99.5 °F) and/or contracted COVID-19 within one week before they were meant to attend the hospital, an answer of a-1. The telMCQs revealed that 64 (80.0%) of 80 participants felt anxious about COVID-19 infection at their visit. A total of 12 (75.0%) of 16 BPPV patients and 15 (88.2%) of 17 MD patients with mild to severe symptoms gave up their reservation due to fear of COVID-19 infection. On the other hand, 4 (25.0%) of 16 BPPV patients and 12 (80.0%) of 15 MD patients with slight to moderate symptoms completed their medical examination despite fear of COVID-19 infection. “Cancellation” in the present study meant that a patient who already had a diagnosis and had made a reservation for their next ear, nose, and throat (ENT) visit to the hospital chose to cancel that reservation. “Non-cancellation” meant that a patient who already had a diagnosis and had made a reservation for their next ENT visit to the hospital chose to attend that reservation. Please see Table 1 for details of the telMCQs questions asked.
The telMCQs revealed that 64 (80.0%) of 80 participants felt anxious about COVID-19 infection at their visit. A total of 12 (75.0%) of 16 BPPV patients and 15 (88.2%) of 17 MD patients with moderate to severe symptoms cancelled their reservation due to fear of COVID-19 infection. On the other hand, 4 (25.0%) of 16 BPPV patients and 12 (80.0%) of 15 MD patients with slight to moderate symptoms completed their medical examination despite fear of COVID-19 infection.
Discussion
The Nara Medical University is situated within the Nara Prefecture. The first Japanese patient to test positive for COVID-19 was a tour bus driver in Nara Prefecture and is believed to have contracted the virus after direct contact with Chinese tourists during the bus tour in Japan. The Nara Prefecture is next to the Osaka Prefecture, one of the biggest cities in Japan, with many COVID-19 positive patients thereafter. Therefore, outpatients who visit university hospitals may fear contracting the COVID-19 infection while traveling from their home to the hospital and vice versa.
Among the diseases that cause vertigo/dizziness, BPPV does not show progressive or irreversible symptoms. Most of the outpatients that cancelled during the COVID-19 pandemic had BPPV. This might be a reasonable reaction because BPPV is the most common cause of vertigo, with a lifetime prevalence of 2.4%. 19 The vertigo and dizziness symptoms associated with BPPV is considered to result from debris that is composed of small calcium crystals from the utricle that are stuck to the crista ampullaris 20 and/or floating in the ear canal. 21 BPPV is usually self-limiting. For the posterior semicircular canal type of BPPV, symptoms generally subside or disappear approximately 1 month after onset, and within 2 weeks of onset in the horizontal semicircular canal type of BPPV. 22 MD can cause recurrent vertigo attacks and fluctuating/progressive sensorineural hearing loss. Outpatients with MD had the least number of cancellations during the COVID-19 pandemic. This is also a reasonable reaction, because MD is characterized by recurrent vertigo attacks, fluctuating hearing loss, and tinnitus, which is a common disease with an incidence of 15 to 50 people per 100 000. 23 Some patients with MD are prevented from participating in activities of daily life, including interaction with their social environment, work, and schooling, due to frequent attacks of vertigo, especially with progressive sensorineural hearing loss, in spite of various kinds of medication. This type of MD is generally called intractable and sometimes requires surgical intervention. 24,25
According to the results of the telMCQs, 75.0% of BPPV cases and 88.2% of MD cases cancelled their appointment and avoided visiting hospitals due to fear of COVID-19 infection, even if they still had moderate to severe symptoms. It is problematic that patients who needed appropriate treatment gave up their appointments due to fear of COVID-19 infection. On the contrary, 25.0% of BPPV cases and 80.0% of MD cases that did not cancel their appointment should not have visited the hospital but stayed home because of their slight symptoms. It is also problematic that patients who do not need to visit the hospital, do so because they are worried about their health. Both visiting hospitals and not visiting hospitals during the COVID-19 pandemic could be stressful for patients, especially those with vertigo/dizziness, and this kind of stress might negatively influence their symptoms. 26,27
This study has 2 limitations. Firstly, the dramatic reduction in the number of outpatients at the ENT department of the Nara university hospital during the 2020 pandemic was compared to the same period in 2019. In our medical records, the total number of vertigo/dizziness patients and the variants of vertigo/dizziness diseases were constant during the most recent 3 years, 2017 to 2019. Therefore, it was only possible to discuss the number of outpatients between 2019 and 2020. Secondly, the severity of vertigo/dizziness in the patients with BPPV and MD was not determined by the relevant guidelines but by the patients’ subjective complaints. However, it is possible that conclusions derived from patients’ subjective data will become part of advanced medical care in the future.
Conclusion
Under the current COVID-19 circumstances, remote medicine is considered a suitable alternative to face-to-face appointments across many medicine-related fields worldwide. Remote medicine also called telehealth, online care, and web-based connected care, began to rapidly play an active part in the medical care system once the pandemic began. 28 -30 The WHO also recommends the use of information and communication technology to maintain and improve health, so-called e-Health. 31 In the ENT field related to vertigo/dizziness, online medicine may include video-lectured diagnosis and canalith repositioning treatment for BPPV, 32 stress less life guidance for MD, and vestibular rehabilitation for VN and SDV. After the COVID-19 pandemic ends, it will be time to prepare for an advanced way of providing medical care, not only for the disease itself but also for the mental distress behind persistent symptoms.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a Japan Society for the Promotion of Science KAKENHI Grant (2020-2022), the Japan Agency for Medical Research and Development (Grant Number 18dk0310092h000a), and a Health and Labour Sciences Research Grant for Research on Rare and Intractable Diseases (R02-Nanchito (Nan)-Ippan-04) from the Ministry of Health, Labour and Welfare of Japan [grant number R02-Nanchito (Nan)-Ippan-04].