
Abstract
Objective:
To investigate if alternated Epley (EP) and Semont (ST) maneuvers could be more effective than repetition of the same in benign paroxysmal positional vertigo of posterior semicircular canal (pBPPV).
Design:
We retrospectively reviewed the outcome of pBPPV patients treated with a second maneuver for the persistence of positional nystagmus.
Study Sample:
Forty-seven patients underwent 2 STs, 64 with 2 EPs, and 71 EPs followed by ST. Videonystagmography and Dizziness Handicap Inventory (DHI) questionnaire were performed.
Results:
Absence of positional nystagmus was achieved after 2 maneuvers in 136 patients with pBPPV: 65.9% in the ST group, 70.3% in the EP group, and 84.5% in the EP-ST group. Alternated EP and ST were significantly more effective than repeated ST (P = .03), while we found no significant difference when compared with repeated EP (P = .07). At 1-month follow-up, 12 patients showed persistent positional nystagmus without difference between groups. After 1 month, the 46 patients with negative outcome had significantly higher DHI values (P = .01) than other 136 patients with pBPPV.
Conclusions:
Alternated EP and ST seemed more effective than repeating the same maneuver in treating pBPPV, and this should be confirmed in prospective clinical studies. Resolution of nystagmus after maneuvers was fundamental to reduce handicap deriving from dizziness as reported in DHI.
Introduction
Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo, with an incidence of 64 per 100 000 persons per year and a lifetime prevalence of 2.4%. 1 Treatment success depends on identifying and specifying the type of BPPV and canal involved. The posterior semicircular canal is affected in 88% of cases (pBPPV), but other canals can cause BPPV as well. 2 The efficacy of maneuvers in BPPV has been established, and appropriate maneuvers are significantly more effective than sham. 3 In pBPPV, Semont liberatory maneuver (ST) was described in 1988, while Epley repositioning maneuver (EP) in 1992.4,5 To date, there was no clear evidence on which of the 2 was more effective for pBPPV. 6 Indeed, the comparison of these 2 maneuvers by a referral center was rarely performed according to a recent and detailed review. 7
Considerable variability was reported in the number of times maneuvers were applied for BPPV treatment across studies and in clinical practice. 8 According to a systematic review, there was a beneficial effect of repeated EP in pBPPV patients who were not fully cleared of symptoms after first maneuver. 9 Similar results were reported for repeated ST in a multicenter randomized double-blind study for pBPPV. 10 In a previous report, the authors changed maneuver in patients who had been resistant to the first selected. 11
In the present study, we retrospectively reviewed the outcome of consecutive pBPPV treated with a second maneuver (EP or ST) in the same session for the persistence of positional nystagmus. The aim was to investigate if alternated EP and ST could be more effective than repetition of the same maneuver in resolving pBPPV positional nystagmus.
Materials and Methods
Patients
The study was conducted in accordance with the principles of the Helsinki Declaration and was approved by our internal ethical committee. Data were examined in agreement with the Italian privacy and sensible data laws. Before undergoing treatment, all patients included in the study signed a detailed informed consent form.
In the present retrospective investigation, we included a series of consecutive pBPPV patients treated with a second maneuver for persistence of positional nystagmus. Exclusion criteria were as follows: (1) absence of nystagmus after first maneuver, (2) bilateral pBPPV or multiple canal BPPV, (3) previous BPPV episodes, (4) neurologic or psychiatric disease, other forms of peripheral or central vertigo, or head trauma, (5) limited motility that contraindicated physical therapy.
Vestibular Examination
All vestibular examinations were instrumental. We routinely prefer video nystagmography for the evaluation of disorders of equilibrium. The diagnosis of pBPPV was done in the presence of the typical upbeat-torsional nystagmus provoked by the Dix-Hallpike test. All patients completed the Italian version of the Dizziness Handicap Inventory (DHI) questionnaire before video nystagmography. 12
Video nystagmography was repeated 15 to 30 minutes after the first and second maneuver. As a positive outcome, we considered the absence of positional nystagmus.
Description of Maneuvers
We used a modified EP; the patient was placed in an upright position with the head turned 45° toward the affected ear. The patient was then rapidly returned to a supine head-hanging position. Next, the head was turned 90° toward the unaffected side. Following this rotation, the head was turned by a further 90° toward the unaffected ear with the trunk rolled onto the unaffected side. Each position was held for approximately 1 minute. Then the patient was brought into an upright sitting position, completing the maneuver.
For the ST, the patient was seated in an upright position and the patient’s head was turned 45° toward the unaffected side. Then the patient was rapidly moved to a side-lying position toward the affected side. Next, the patient was rapidly moved to the opposite side-lying position without changing the head orientation. Each position was maintained for approximately 2 minutes. Then the patient was brought into the upright sitting position.
Follow-Up
All patients underwent a follow-up control with DHI and video nystagmography after 1 month. No postural restrictions or soft cervical collars were suggested during this period.
Statistical Analysis
We used the Mann-Whitney U test and χ2 test as appropriate. A P value <.05 was considered significant. The Social Sciences version 17 statistical package (SPSS Inc) was used for all analyses.
Results
Patients’ Clinical Characteristics
In the present investigation, we considered 182 consecutive pBPPV patients treated with a second maneuver for persistence of positional nystagmus after the first one. We identified 47 patients treated with 2 ST maneuvers (ST group), 64 with 2 EPs (EP group), and 71 patients treated initially with EP and then with ST (EP-ST group). The different physicians according to their own preference made the choice of first and second maneuvers. Age, gender, affected side, and symptom duration (the period from symptoms onset to first maneuver) were not significantly different among the 3 groups (Table 1). Patients completed DHI questionnaire before video nystagmography. The mean results of DHI were 40.3 (SD: 18.2) in the ST group, 38.6 (SD: 20.1) in the EP group, and 37.1 (SD: 19.3) in the EP-ST group. The Mann-Whitney U test found no differences in DHI between the ST and EP groups (P = .21), ST and EP-ST (P = .14), and EP and EP-ST groups (P = .47).
Patients’ Demographic and Clinical Characteristics in the 3 Groups (ie, Repeated Semont [ST] and Epley [EP] Groups and Alternated EP-ST Group).
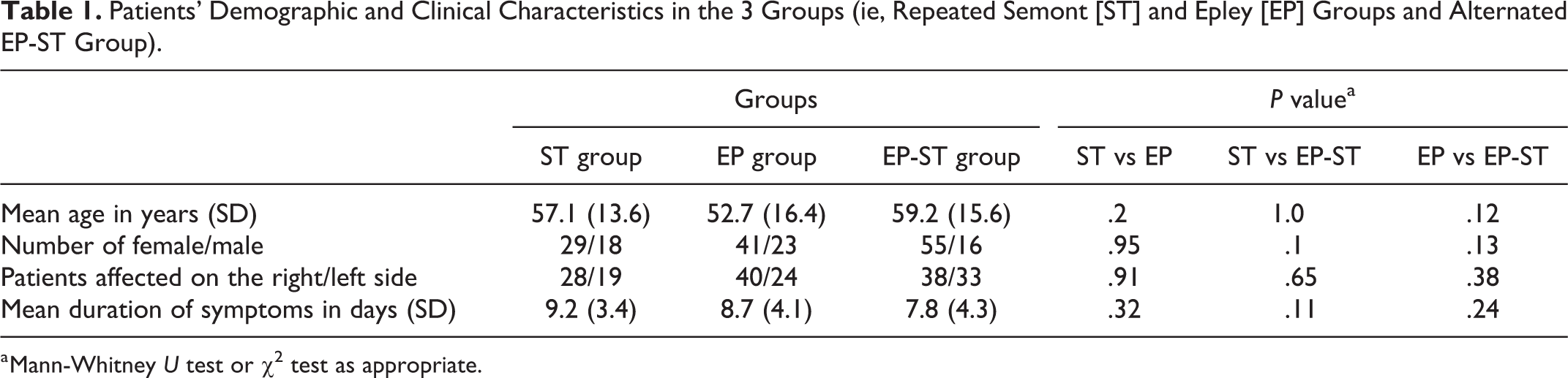
a Mann-Whitney U test or χ2 test as appropriate.
Results of the Maneuvers
Forty-six out of the 182 patients with pBPPV (25.3%) had persistent nystagmus after 2 maneuvers. Table 2 showed the outcome after 2 maneuvers in the 3 groups of patients with pBPPV. The positive outcome was the absence of positional nystagmus after the second maneuver. The use of alternated EP and ST maneuvers was significantly more effective than repetition of ST (χ2 test, P = .033). However, a comparison of alternated EP and ST to repeated EP did not achieve significance (χ2 test, P = .075).
Outcome After the Maneuvers and at 1-Month Follow-Up in the 3 Groups (ie, Repeated Semont [ST] and Epley [EP] Groups and Alternated EP-ST Group).
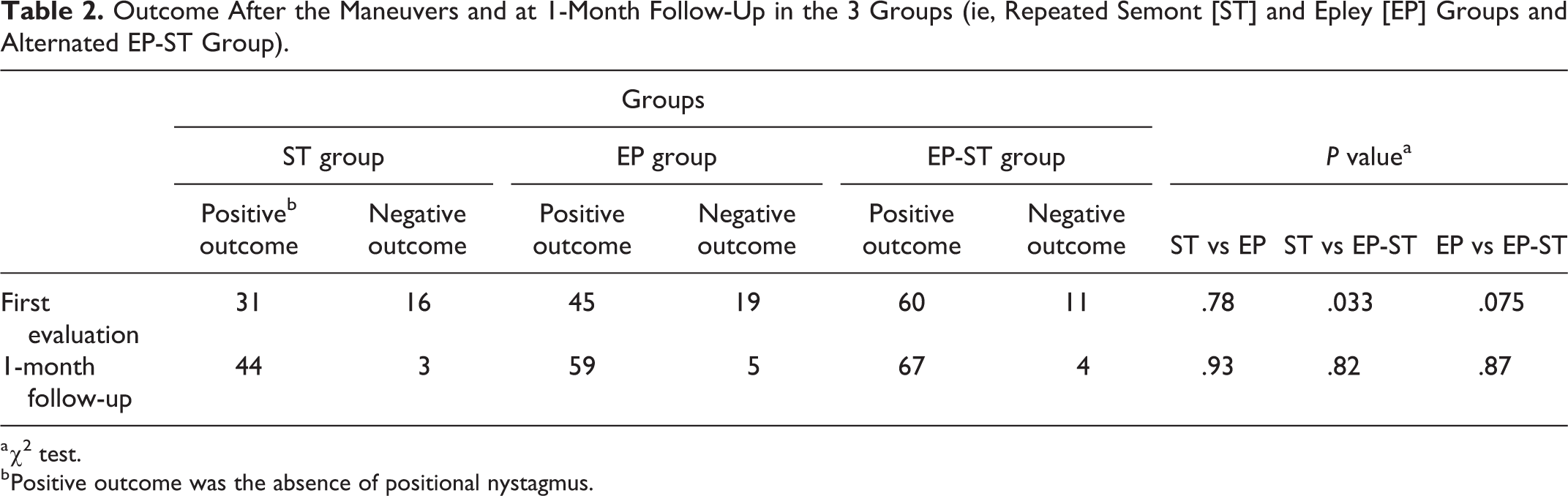
a χ2 test.
b Positive outcome was the absence of positional nystagmus.
Follow-Up
One month after first evaluation, DHI tended to be higher in the ST group (mean: 9.5, SD: 4.5) than the EP-ST group (mean: 4.2, SD: 3.9), but this difference did not achieve statistical significance (Mann-Whitney U test, P = .07). The DHI of the EP group (mean: 5.9, SD: 4.5) was not different when compared with others (Mann-Whitney U test, ST, P = .9, EP-ST, P = 1.0). The DHI was significantly higher (Mann-Whitney U test; P = .01) in the 46 patients with persistent positional nystagmus (mean: 16.3, SD: 6.7) when compared with 136 patients with good outcome after the maneuvers (mean: 4.5, SD: 3.0). At 1-month follow up, video nystagmography showed persistence of positional nystagmus in 12 patients (6.6%), with no differences between the 3 groups (Table 2).
Discussion
Epley originally mentioned the use of repeated maneuvers until no nystagmus was found during the last cycle or until no progress was apparent in the last 2 cycles. 5 Nevertheless, a treatment approach based on a single physical maneuver during the first treatment session was commonly reported for BPPV.13,14 A recent systematic review underlined the effectiveness of repeated maneuvers for pBPPV. 9 The authors recommended the use of repeated application of EP, either in the same or in a consequent session, in patients who were not symptom-free after the first maneuver. 9 Gordon and Gadoth 15 evaluated 125 patients with pBPPV: The group of patients treated with repeated EP maneuvers in the same session showed absence of positional nystagmus in 92% of cases, while a good outcome was achieved in only 80% of patients in the group managed with a single EP. von Brevern et al 16 considering 35 patients with pBPPV found after one EP a success rate of 43% that raised up to 80% after the second maneuver in the same session. Korn et al 17 reported a 68% success rate following a single-maneuver session, as opposed to an 88% success rate when up to 4 maneuvers were applied in the first session. In a recent multicenter, randomized, double-blind study, Lee et al 10 compared EP, ST, and sham maneuver for the treatment of 99 pBPPV patients: 32 patients were assigned to ST groups; positional nystagmus was absent in 37.5% of cases after first ST and in 65.6% after the second ST in the same session. 10
In the present study, we retrospectively reviewed the outcome of consecutive pBPPV treated with repeated maneuvers in the same session for the persistence of positional nystagmus. We included 47 patients managed with 2 STs, 64 with 2 EPs, and 71 patients who underwent EP followed by ST. The aim was to investigate if alternated EP and ST could be more effective than repetition of the same maneuver. The main weaknesses of the present investigation were the retrospective design and the limited number of included patients. The main strength was the homogeneity of the case series considered. In fact, there were no significant differences in terms of age, gender, affected side, symptom duration, and DHI at presentation among the 3 groups. Furthermore, all patients had a negative medical history of previous vestibular pathologies, and all underwent an objective instrumental vestibular examination by video nystagmography before and after all the maneuvers. Most of the reports on pBPPV relied only on bedside examination.9,10,13,14
In the present investigation, positive outcome (ie, absence of positional nystagmus) was achieved after 2 maneuvers in 136 patients with pBPPV: 65.9% in the ST group, 70.3% in the EP group, and 84.5% in the EP-ST group. Alternated EP and ST maneuvers were significantly more effective than repeated ST (P = .03), while we found no significant difference when compared with repeated EP (P = .07). Toupet et al 11 used an alternate maneuver after EP. In their series of 113 pBPPV after EP, the success rate was 52%, and it changed to 64% with an alternate ST. A previous report compared the efficacy between repetition of EP and switch to alternate ST maneuver in treating pBPPV. 18 The authors found no differences between the 2 approaches. Variations in the canal geometry of the membranous and bony labyrinth were described in human inner ear specimens. 19 Johnson Chacko et al 19 using high-resolution X-ray microtomography images found that semicircular canals of the bony and membranous labyrinth were not aligned exactly on the same planes. Thus, it was reasonable to hypothesize that some patients with persistent positional nystagmus could respond better to a different maneuver, as suggested by our results.
At 1-month follow-up visit, only 6.6% of patients showed the persistence of positional nystagmus, confirming that pBPPV had a good prognosis as reported by a systematic review. 9 Nevertheless, the 46 patients with negative outcome after the first maneuver session had significant higher DHI results after 1 month. This suggested that resolution of nystagmus was crucial to reduce the global handicap deriving from dizziness as reported by the questionnaire. The DHI comprised 25 items subdivided into physical, functional, and emotional subscores, and it provided a useful, reliable and valid assessment of self-perceived handicap associated with dizziness. 12
In conclusion, according to our preliminary results, in pBPPV, alternated maneuvers (ie, EP followed by ST) were more effective than repeated ST, while the comparison with EP showed no significant difference. It is possible larger sample sizes would have elucidated a differences with the latter treatment strategy. The resolution of nystagmus was associated with significantly lower symptoms as reported by the DHI at 1-month follow-up. Our results should be necessarily confirmed in prospective randomized clinical trials.
Footnotes
Authors’ Note
All authors have contributed sufficiently and approved the manuscript. All procedures performed in the study were in accordance with the ethical standards of our institutional research committee and with the 1964 Helsinki Declaration and its later amendments.
Acknowledgments
The authors thank Jane Castelman for correcting the English version of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.