
Abstract
Objectives:
To determine the number of patients with idiopathic subglottic stenosis (iSGS) who have contracted coronavirus disease 2019 (COVID-19), the impact of the pandemic on patients’ attitudes on seeking help and attending hospitals, as well as the delays in the offer of treatment from the local health care systems.
Methods:
A 29-question survey was distributed to an international mailing list of patients with subglottic stenosis to assess the patient experience during the COVID-19 pandemic.
Results:
A total of 543 patients with iSGS participated. Fewer than 1 in 10 patients with iSGS have experienced COVID-19 symptoms, which were predominantly mild to moderate, with only 2 hospitalizations. Most patients with iSGS (80.0%) have not been advised they are high risk for COVID-19, despite 36.5% of patients with iSGS being obese (body mass index of 30+). Delays to surgeries and in-office procedures have impacted 40.1% of patients currently receiving treatment, with 38.8% of patients increasingly struggling to breathe as a result. Anxiety and stress are increasing among patients, with 3 in 4 (75.2%) reporting they are anxious about travelling by public transport, contracting the virus in hospital and infecting loved ones (69.0% and 71.9%, respectively). Of greater concern is that 23.1% with increasing dyspnea state they are staying away from hospital despite their deteriorating health.
Conclusions:
The COVID-19 pandemic has had an impact on the physical and psychological health of patients with iSGS. Surgeons managing cases of laryngotracheal stenosis need to offer appropriate support and communication to these high risk patients. During the pandemic, this should include self-isolation if they are dyspneic or on treatments that may have reduced their immunity. In addition, they should offer safe clinical pathways to airway assessment and treatments, if they become necessary. To minimize unnecessary travel, much of the clinical monitoring can be carried out remotely, using telephone or video-based consultations, in conjunction with local health professionals.
Introduction
Idiopathic subglottic stenosis (iSGS) is a rare fibroinflammatory disease of the subglottis, leading to airway stenosis, seen predominantly in Caucasian women after puberty. 1 The most common symptoms of iSGS include dyspnea, cough, wheezing, stridor, and difficulty clearing secretions. 1,2
The novel coronavirus disease 2019 (COVID-19) was designated a pandemic by the World Health Organization in March 2020. It has caused particular concern among patients with iSGS. An airway stenosis such as that seen in iSGS adversely affects lung function and reduces mucociliary clearance. The need for intubation and ventilatory support, in theory, is more likely in these patients. Intubation of a stenosed and inflamed airway is not only technically more challenging but runs the risk of causing worse long-term laryngotracheal stenosis and irreversibly damaging laryngeal functions such as the voice and swallowing. These factors probably make patients with iSGS more at risk of short and long-term COVID-19 complications.
Research was needed for a better understanding of the impact of the pandemic on the normal care pathways for patients with iSGS, their attitude to visiting hospitals and clinicians, but also to learn about its impact on their physical and psychological health. From those patients with iSGS, who had contracted the COVID-19 virus, it is important to know about their experiences and journey to recovery.
Methods
A survey was conducted among members of an international, online iSGS support group, Living with iSGS. The iSGS support group is independently run through a social media platform (Facebook, www.facebook.com; Menlo Park, California) and currently contains 4550 members.
A 29-question survey, taking an average of 7 minutes to complete, was designed and conducted by patient advocate, founder, and administrator of the iSGS patient support group (Catherine Anderson) with input from a panel of expert clinicians, acknowledged below. The survey consisted of questions relating to patient demographics, symptoms and treatments, comorbidities, concurrent medical treatments, body mass index (BMI), impacts of delays in receiving medical care, and attitudes toward travel and hospital visits (questionnaire provided in appendix).
The survey was programmed using an online survey platform (SurveyMonkey, www.surveymonkey.com; San Mateo, California) and emailed to members of the iSGS support group (past and present). Participation was voluntary and anonymous and open to all patients who had provided an email address. The survey was left open for a 1 week period between May 18 and 25, 2020. Duplicate responses were prevented through SurveyMonkey’s monitoring of IP addresses, allowing 1 response per person. During the time the survey was open, 1 email reminder was sent out, and there were 2 announcements in the Facebook group. If patients had a diagnosis other than idiopathic (including autoimmune, polytrauma, or iatrogenic) or an idiopathic stenosis in an area other than the subglottis (supraglottis, glottis, or trachea), they were excluded from the analysis (n = 94).
Results
Impact of COVID-19 on Patients With iSGS
An email invitation to participate was sent to 938 group members. A total of 543 women and 1 man, diagnosed with iSGS, responded to our survey (58% response rate).
All of these patients indicated their stenosis as being idiopathic in nature. Demographic data are presented in Table 1.
Demographic Data.
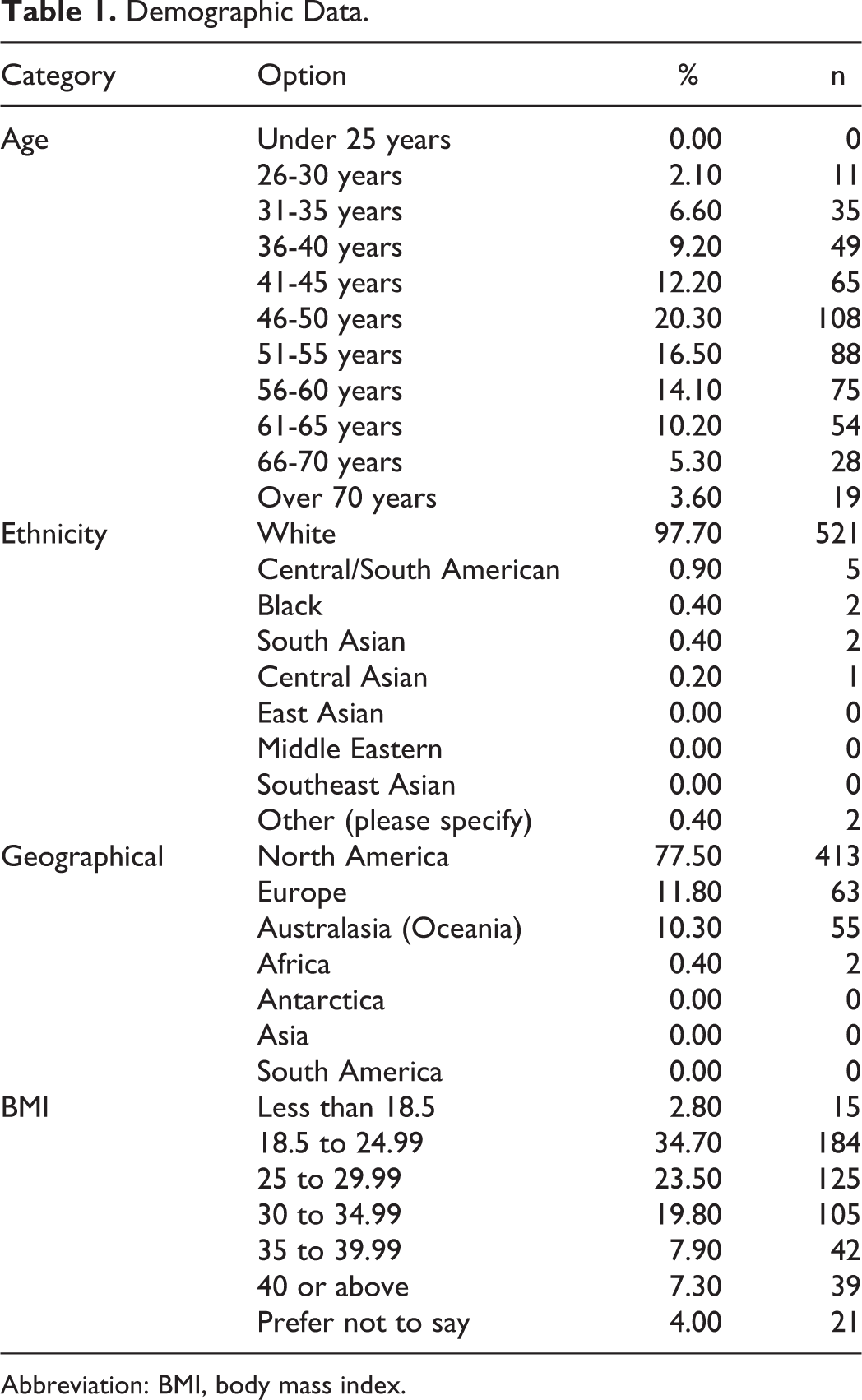
Abbreviation: BMI, body mass index.
At the early stages of the pandemic, access to COVID-19 testing was limited and varied by countries. 3,4 We decided to include responses from all patients with iSGS who experienced possible COVID-19 symptoms, regardless of their test results. Although many of these patients might have experienced other respiratory illnesses, the psychological impact is, nevertheless, equivalent.
A total of 9.7% (n = 52) of patients with iSGS self-reported as having experienced symptoms associated with COVID-19. 5 Just 4% (n = 2) have tested positive, 65% (n = 35) had not been tested, and 31% (n = 17) had tested negative (Figure 1).
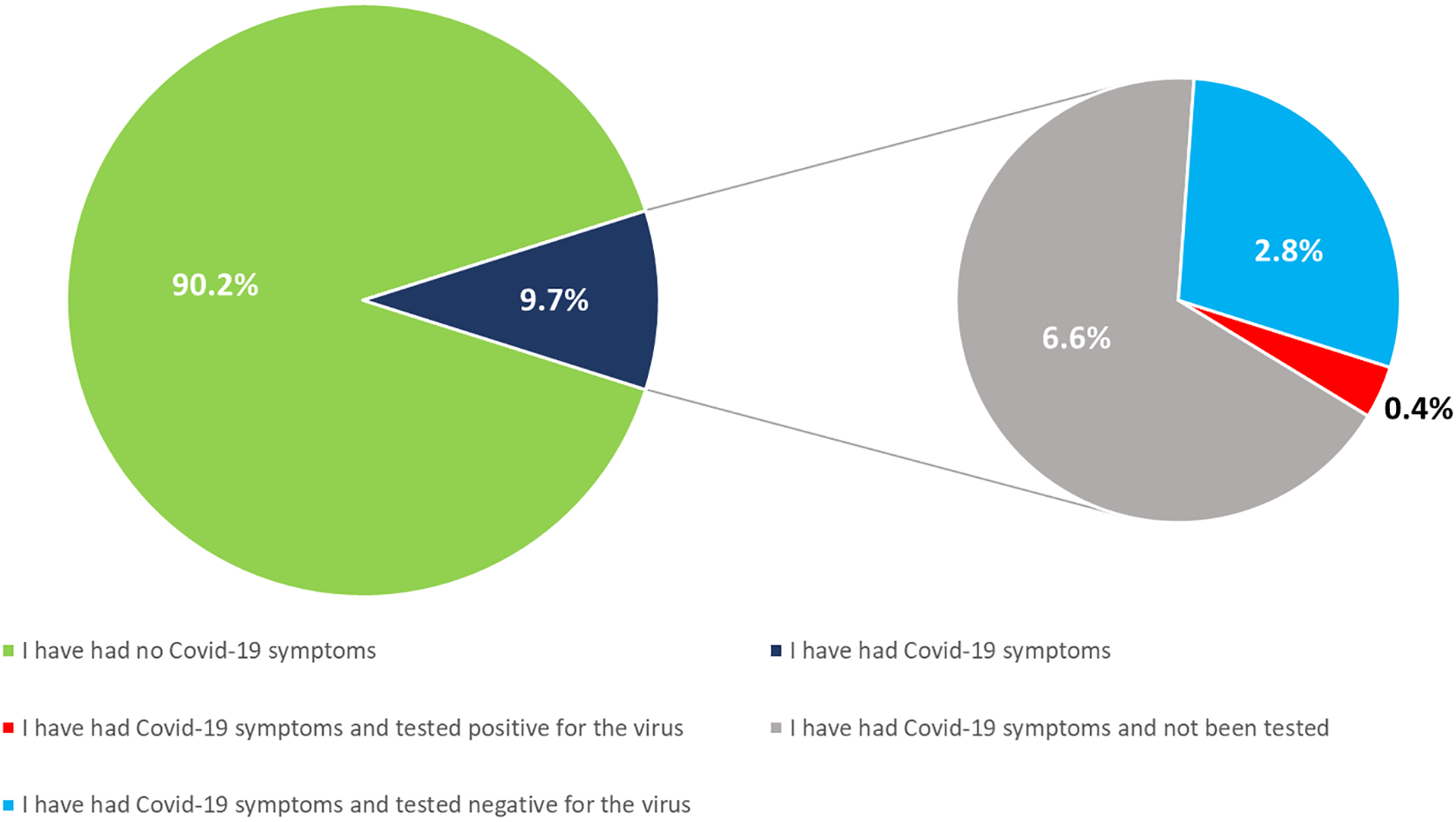
COVID-19 in iSGS patient group. Question: “How have you fared during the COVID-19 pandemic so far?” (total number of responses = 533). COVID-19 indicates coronavirus disease 2019; iSGS, idiopathic subglottic stenosis.
The most common symptoms experienced include fatigue (84.6%), myalgia (63.5%), headache (55.8%), dry cough (53.8%), and fever (50.0%). However, new onset dyspnea, not typical of the patient’s usual breathlessness, was only reported in 34.6% of patients (Figure 2). Just 3.8% (n = 2) of patients went to hospital for their symptoms, the others recovered at home. The majority of patients felt better within 3 weeks (86.5%).
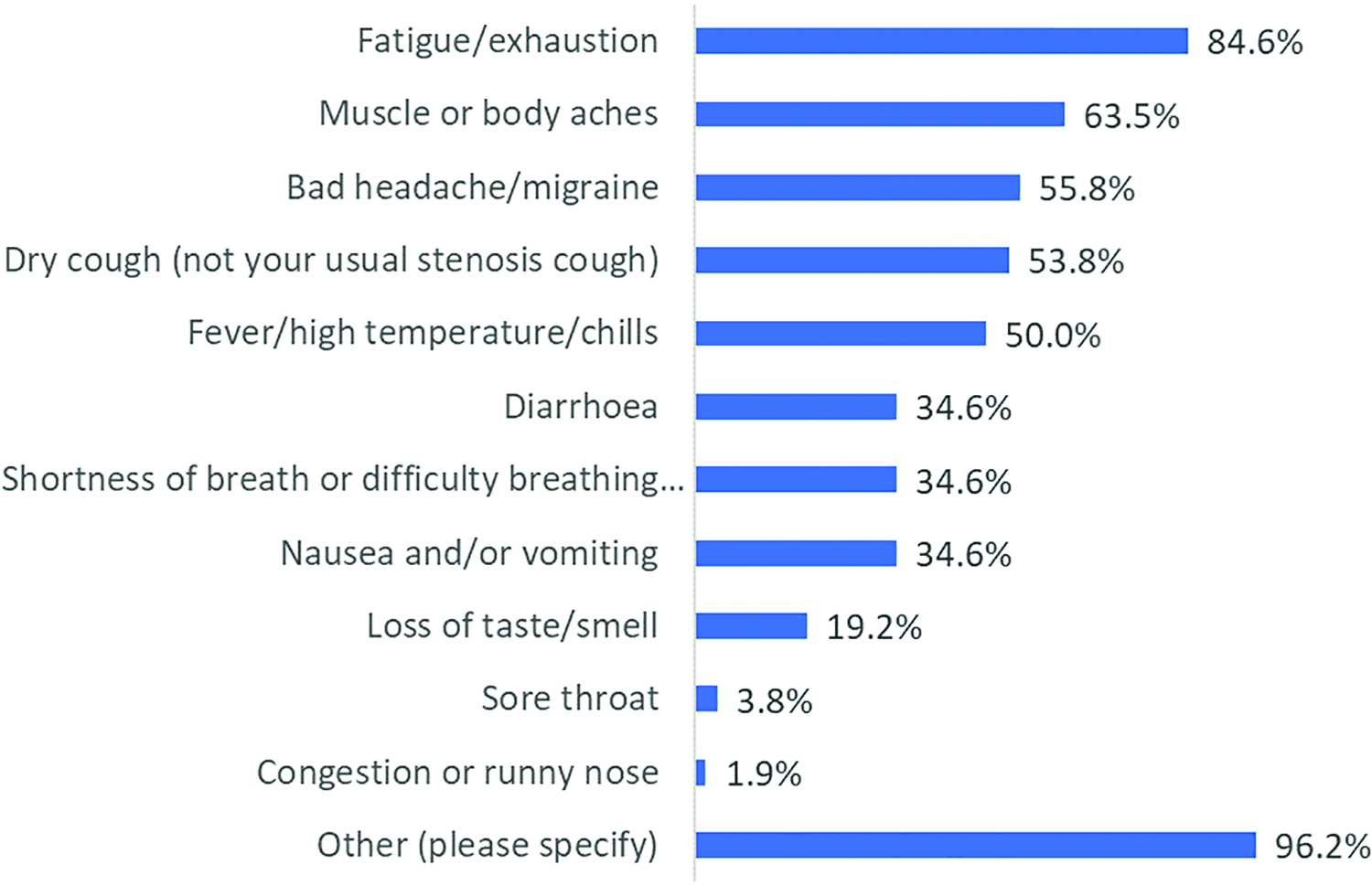
Symptoms of COVID-19. Question: “Which of the following symptoms did you experience?” (total number of responses = 52). COVID-19 indicates coronavirus disease 2019.
Hypertension, obesity, diabetes, respiratory, and cardiovascular diseases increase the risk of developing severe COVID-19, 6,7 however, the impact of airway stenosis on the course of this disease remains unknown. Medical advice to be placed in the high risk group varied considerably in our cohort, with just 20.0% (n = 106) reporting to have been categorized as high risk patients. Over a third of these patients (37.1%, n = 39) have an associated high risk comorbidity. However, other reasons for being labelled high risk include a history of rapid airway deterioration following infections (28.6%, n = 30), delayed airway surgery (18.1%, n = 19), and immunosuppressant therapy (12.4%, n = 13). Simply being a patient with iSGS was cited as the main criteria for inclusion in the high risk group in 10.5% (n = 11) of respondents.
Obesity has been highlighted as significant risk factor for respiratory complications in patients infected with COVID-19. Obesity is often associated with respiratory diseases, diabetes, cardiovascular diseases, and nonalcoholic fatty liver disease. Occasionally presenting simultaneously, this array of potential disorders and diseases could exacerbate the prognosis of patients with COVID-19. 8,9 In addition, a recent study found that postdilatation recurrence of stenosis is more rapid in patients with a BMI of 30 to 34.9. 10 Our survey revealed that 36.5% (n = 186) of patients with iSGS have a BMI of 30 or above, but only 22.8% (n = 42) of these have been informed by their doctor they are higher risk for COVID-19. Most patients having iSGS with a BMI of 30+ are socially isolating (74.9%, n = 135), and a small minority (1.6%, n = 3) are shielding (staying at home, having minimal contact with anyone, including their family). The proportions of patients self-isolating and shielding were the same in those with a BMI below 30.
Delays to Treatment
Of patients receiving interval treatments for their iSGS, 40.1% (n = 153) have experienced delays. A larger proportion of patients who are normally scheduled for in-office procedures (eg, steroid injections, bronchoscopy, check-ups) report delays (71.2%, n = 109).
Just under half of patients who had delayed appointments or delayed procedures remained symptom free with their airway (53.3%, n = 81). Of the 56.6% (n = 86) reporting worsening airway symptoms, around 3 in 5 (68.6%, n = 59) are starting to struggle, while others have noticed only mild dyspnea (5.8%, n = 5). Delayed treatment has led to increased stress levels and/or panic attacks in 4.7% of respondents (n = 4; Figure 3).
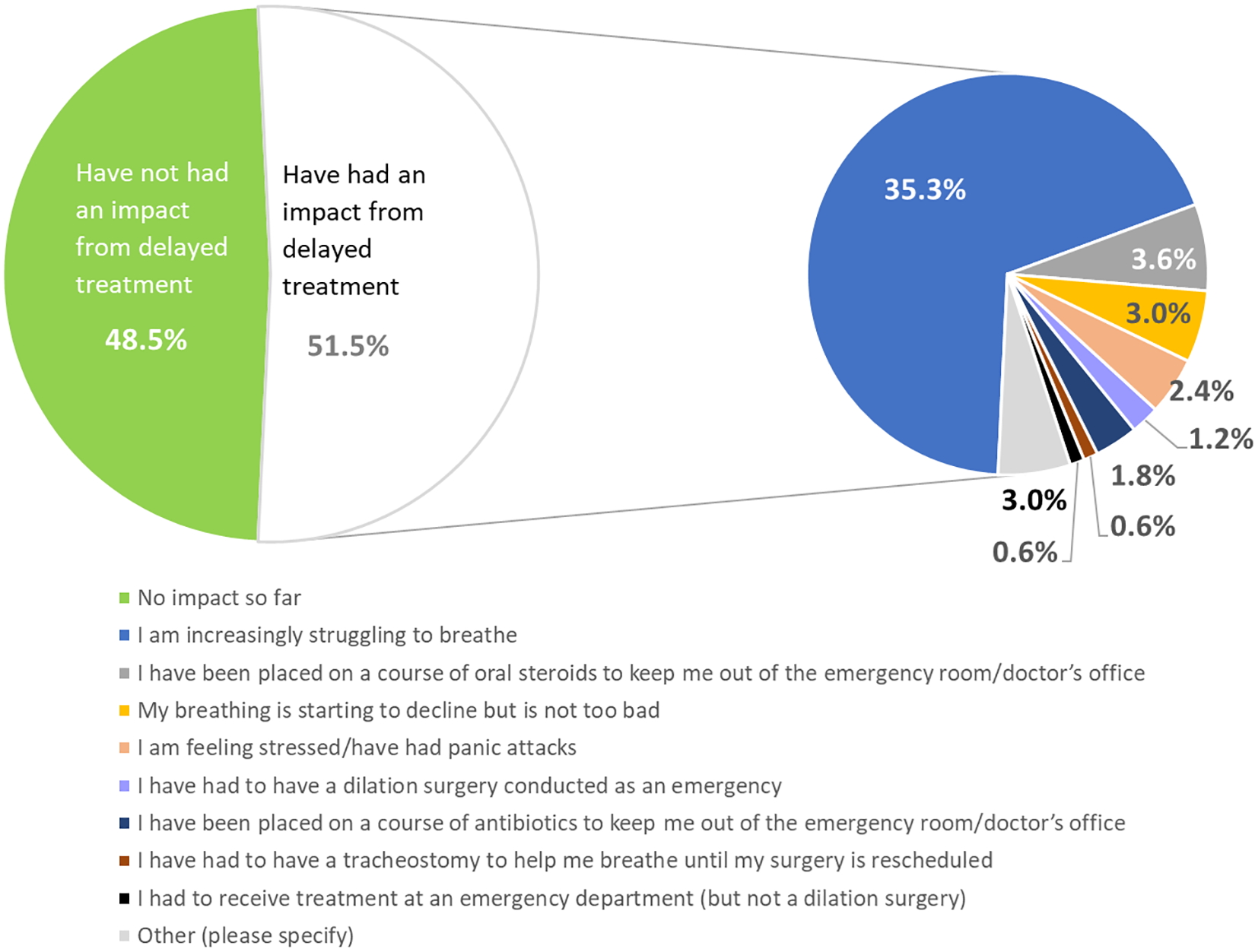
Impact of delays in treatment during COVID-19 pandemic. Question: “How has the delay in your airway treatment impacted you?” (total number of responses = 167). COVID-19 indicates coronavirus disease 2019.
Changes in Patient Attitudes
Examining the patients’ attitudes to attending doctor appointments, hospitals, and travelling by public transport in particular revealed high levels of anxiety within our cohort.
The risk of contracting the virus in hospital was a significant concern to 69.2% of our sample, while the concern of passing the virus on to loved ones was expressed by 71.6% (Figure 4).
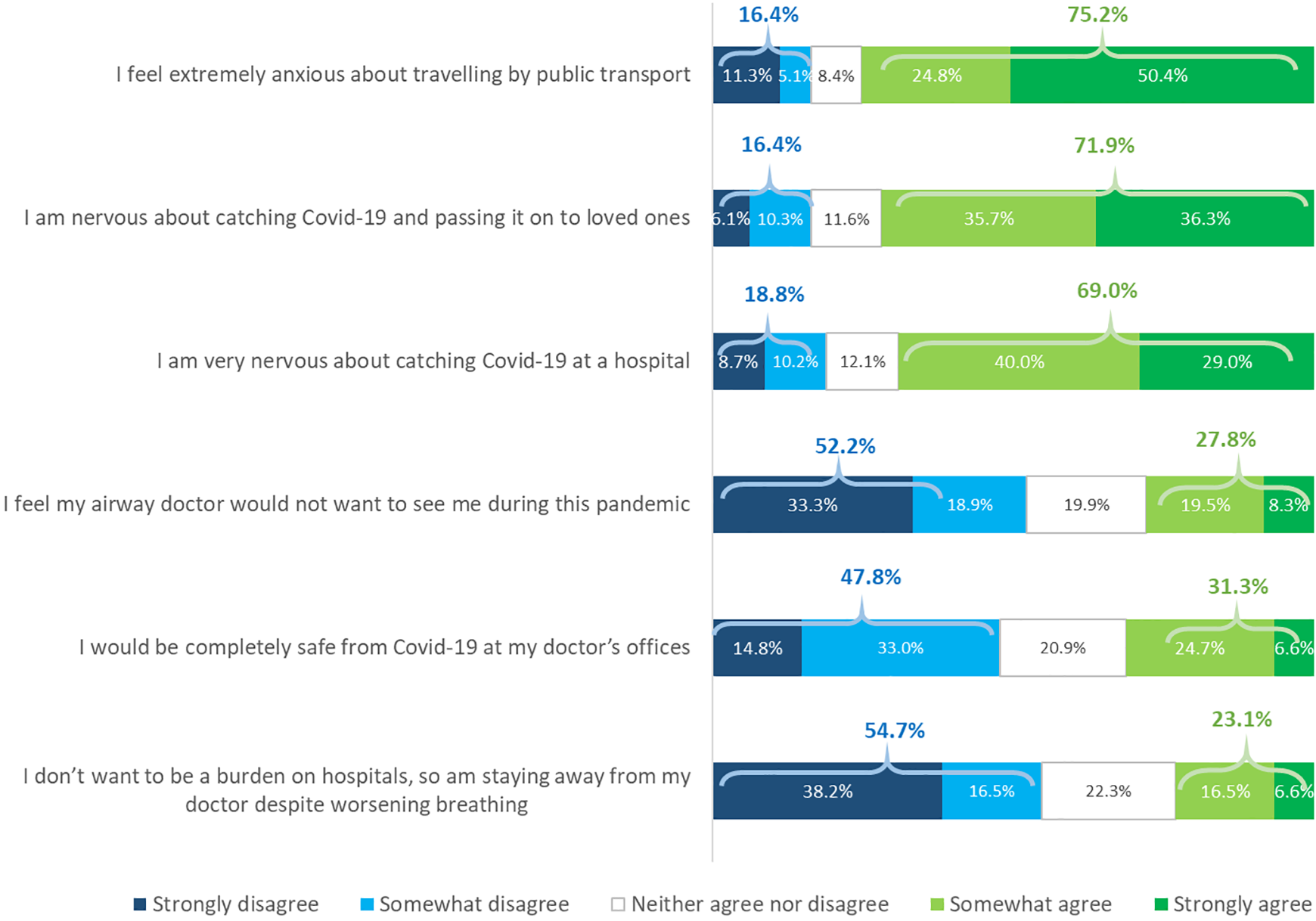
Patients’ attitudes toward seeking treatment during the pandemic. Question: “To what degree do you agree or disagree with the following statements?” (total number of responses = 364).
With respect to the question regarding travel using public transport, 3 of 4 patients with iSGS (75.2%) report that they are extremely anxious (Figure 4).
Other factors impacting patients’ attitudes toward seeking medical help included the perception that their treating physician would not want to see them during the pandemic (27.8%), others did not wish to increase the burden on their hospital (23.1%; Figure 4).
Discussion
We present an analysis of the patient experience of iSGS during the COVID-19 pandemic. The majority of patients with iSGS have not contracted the virus to date and those who have been unwell have had relatively mild symptoms. Only 2 patients were hospitalized, and both have returned home and fully recovered.
Delays to treatment, due to the pandemic, have resulted in some patients experiencing increased dyspnea. Treatment delays might have been completely appropriate given the initial lack of personal protective equipment (PPE), safety protocols, and unknown risk to health care workers. We would presume that a general risk benefits were weighed in these cases, however, we can’t, based on our data, exclude treatment delays due to hospital capacity reduction during the pandemic. Anecdotally, in the authors’ National Airway Centre, delays were limited to patients self-cancellations and in-office injections. However, the survey covers a large patient sample with wide geographical spread and a variety of treatment settings with different local circumstances.
Another key concern should be the change in attitude toward going to hospital and seeking medical help. Patients with chronic conditions are more likely to be anxious about contracting COVID-19 themselves or infecting members of their families. 11 Similar to our cohort, patients’ attitudes were reported to contribute to the drop in numbers of patients attending for endoscopic procedures week on week at the height of the COVID-19 outbreak in Northern Italy. 12 Similar pattern of reduced hospital attendance during the pandemic was reported in stroke 13 and acute coronary syndrome likely leading to increased out-of-hospital deaths and long-term complications of myocardial infarction. 14
Using public transportation was a major concern among our patient group. Similar concerns were expressed in a survey of pregnant women where 46.5% reported changing their mode of transportation method to receive medical care. 15 To alleviate these risks, patients who are obliged to use public transport for medical care should be offered remote appointments or have their appointments or surgeries moved to hospitals that can be reached by car. Alternatively, this medical review and treatment could be carried out in close collaboration with medical teams local to the patient, leaving travel to tertiary specialist centers only when this cannot be offered.
Stress and anxiety are eased with careful communication, education, and advice on what patients should be doing at this time—firstly to stay safe (are patients with iSGS more at risk than the average person?), but also creating and educating patients on safe pathways for attending appointments at hospital or the doctor’s offices.
Patients who have experienced symptoms of COVID-19, whether or not proven through testing, express concerns that they have not received a timely medical review. This could be avoided by proactively providing appropriate information and reassurance, but also by developing and sharing information on safe pathways to medical facilities.
The authors hope to be able to revisit this cohort of patients with another questionnaire in the future to see how attitudes and perceptions have changed.
Limitations
It was our aim to capture an accurate view of the experiences of patients with iSGS during the COVID-19 pandemic by polling a large international iSGS support group. Our findings may be affected by the inherent nature of a survey study, as there must be some participation and recall bias. Question stems and answer choices were sensitively crafted and thoroughly reviewed prior to distribution, however, the misinterpretation of questions and answers is still possible. The inclusion of all patients who experienced symptoms commonly seen with COVID-19 infection, regardless of a positive test, could open these results to errors, by capturing patients who may have had other respiratory tract infections. Finally, a 1-week period where the survey was open only captures a snapshot of a long drawn out process responding to COVID. As the pandemic and our psychological interaction with the disease evolves, responses are likely to continue to change. Despite these weaknesses, we feel that this study provides an important insight into the impact of COVID-19 on patients with iSGS.
Footnotes
Appendix: Questionnaire
Acknowledgments
The authors would like to thank Professors Martin Birchall, Reza Nouraei, Marshall Smith, and Daniel Novakovic for their invaluable contribution to the design of the survey.
Author’s Note
Catherine Anderson is now an Independent Researcher.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.