
Abstract
The surgical treatment of oropharyngeal squamous cell carcinoma (OSCC) has undergone a considerable evolution, with, among others, transoral robotic surgery (TORS). However, TORS is rarely used for the surgery of soft palate. A 73-year-old man presented a human papilloma virus OSCC of the posterior soft palate. The tumor was resected using TORS. This report describes the surgical technique step by step of the tumor resection. The resection of early stage OSCC of the posterior surface of soft palate is possible through TORS. The procedure is noninvasive, rapid, and seems to be associated with excellent functional outcomes.
Introduction
Oropharyngeal squamous cell carcinoma (OSCC) is one of the most important head and neck cancer in United States. Oropharyngeal squamous cell carcinoma usually developed from the lateral wall of oropharynx (tonsillar fossa or glossotonsillar sulci) or the base of tongue. 1 Oropharyngeal squamous cell carcinomas of the soft palate are fewer and mainly develop from the anterior surface or uvula. 2 The surgical treatment of early and advanced stages of OSCC has undergone a considerable evolution over the past decades with a shift toward minimally invasive strategies including transoral laser surgery, or more recently, transoral robotic surgery (TORS). The objective of minimally invasive surgical approaches is to reduce both morbidity and mortality related to postoperative complications while maintaining adequate overall and recurrence-free survival as well as good quality of life of patients with OSCC.
Transoral robotic surgery improves both the visualization of the operating field and the tumor manipulation through a 3D, 30° angled vision endoscopic camera. The camera of Da Vinci system (Intuitive Surgical) is introduced transorally through a mouthgag, which allows a magnified view of the laryngopharyngeal structures. Transoral robotic surgery is particularly used for OSCC located on the lateral or posterior walls of the oropharyngeal cavity and for tumor of the base of tongue. 2 To date, the usefulness of TORS for lesion of the posterior surface of soft palate is still lacking. To our knowledge, this report represents the first reported case of TORS for lesion of the posterior surface of soft palate.
Case Report
A 73-year-old man was referred to the department of otolaryngology–head and neck surgery for a lesion of the posterior soft palate. The tumor has been discovered during a positron emission tomography (PET) computed tomography, which was realized for the follow-up of a lung cancer. The PET-scanner revealed a 1-cm hypermetabolic nodule of the posterior surface of the soft palate. Otolaryngological examination and complementary examination found no other lesion and no metastasis. The tumor appeared to be superficial. The endoscopy revealed a well-limited tumor without deep infiltration. The histopathological analysis showed an invasive human papilloma virus–induced OSCC. Patient accepted the TORS resection of the tumor. Institutional review board approval was not required.
Results
Surgical Approach
Transoral robotic surgery was performed with the da Vinci X 4 arms System. Only 3 arms were used (camera arm and 2 instrument arms). The surgical approach was divided in 4 steps.
Patient installation
Patient was operated in supine position under general anesthesia with orotracheal intubation. The robot was placed at the head of the patient. The intubation tube was fixed on the middle of the inferior lip. The patient eyes were protected. A Boyle-Davis mouth retractor was used for opening the oral cavity and then fixed to a chest press in order to place the patient head in hyperextension.
Robot setting
The 3D, 30° angled vision endoscopic camera and 2 articulated robotic arm instruments were positioned transorally. The lateral robotic arms consisted of a Maryland forceps for manipulating anatomical structures and the 5-mm monopolar spatula, which was used for tissue resection and coagulation.
Exposition of the posterior surface of the soft palate
We used 2 rubber catheters for lifting the posterior surface of the soft palate. The uvula was attached to the anterior side of the soft palate with a suture thread (Figure 1). Then, the inverse introduction of the 30° up endoscope into the oropharyngeal cavity led to the visualization of the posterior surface of the soft palate (Figure 2).
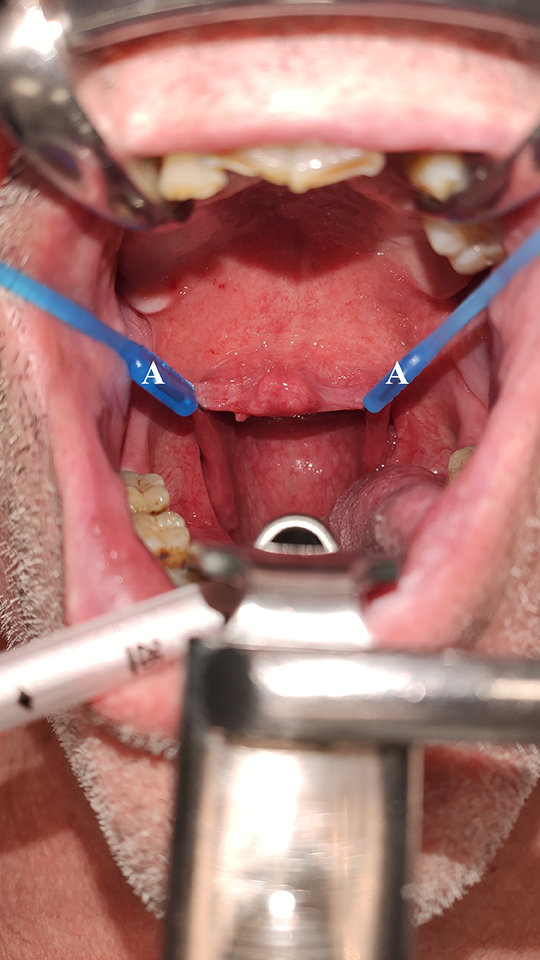
Exposition of the posterior surface of the soft palate. The soft palate was lifted anteriorly, superiorly and outside with 2 rubber catheters (A) placed on each corner of the soft palate.
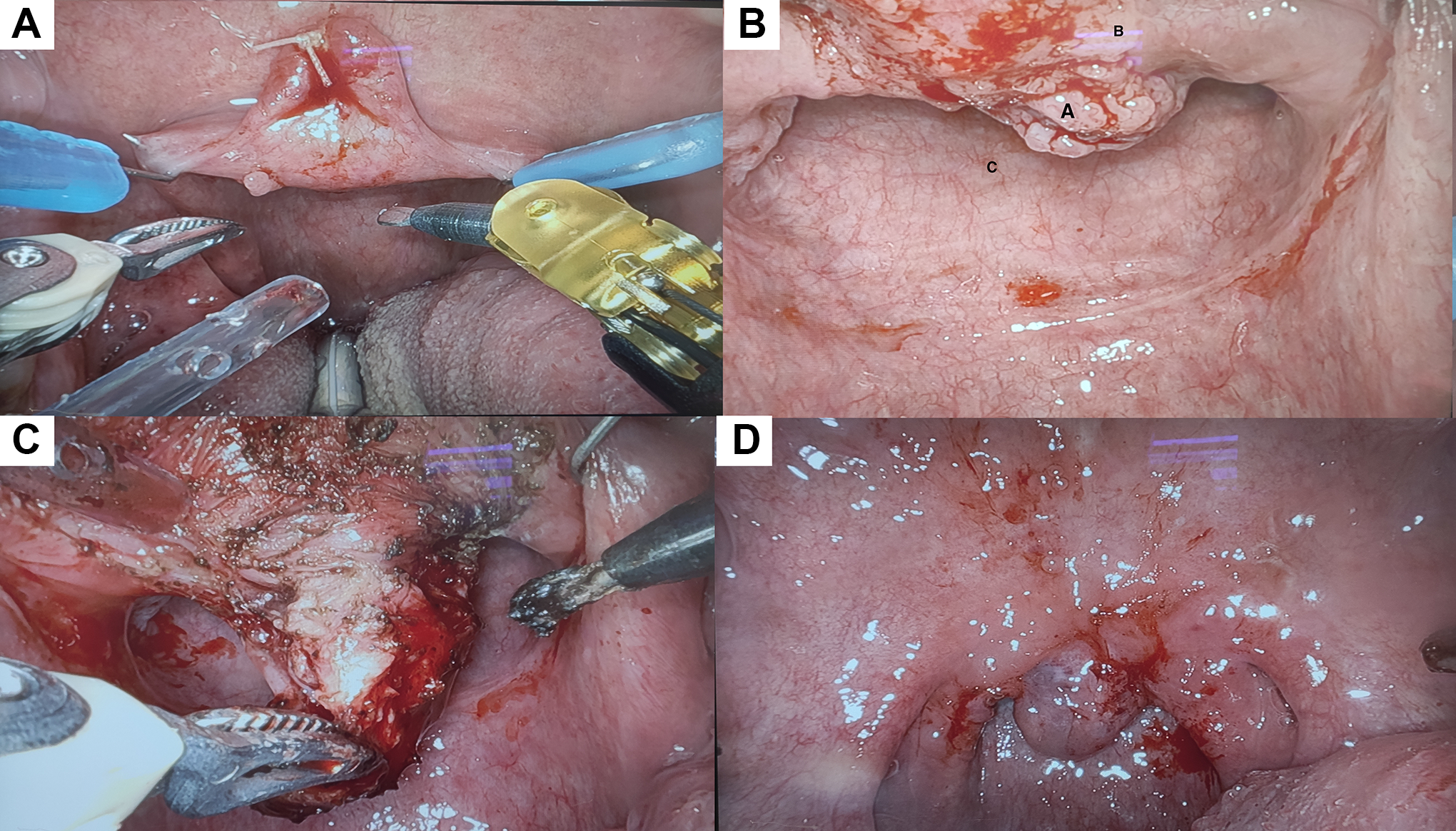
View of the operative field. Anterior side of the soft palate (A). Posterior side of the soft palate (B). A, Tumor, (B) posterior side of the soft palate, (C) posterior wall of the nasopharynx. Tumor resection (C). Anterior side of the soft palate after resection of the tumor (D). The soft palate has been preserved and the anatomy was well respected.
Tumor resection
This installation allowed the tumor resection with an adequate control of the surgical margin. Using the Maryland forceps on the left hand, the tumor was pulled out with for revealing the dissection plans and removing the tumor safely with the help of the 5-mm monopolar spatula, placed on the right hand. The tumor has been progressively pull down and en bloc resected (Figure 2). The margins were marked with ink (Figure 2). Note that the soft palate has not been cut or gotten through.
Surgical and Postoperative Outcomes
Robotic set-up time, robotic operative time, and the mean estimated blood loss were 15 minutes, 20 minutes, and 15 mL, respectively. The patient was discharged home one day after surgery and used only painkillers and nasal saline irrigation. The patient has been seen 2 weeks after the surgery and followed periodically. No postoperative complications were found. Patient had no velopharyngeal insufficiency. The margins were all negative.
Discussion
Since the introduction of TORS in otolaryngology, 3 the use and the indications of TORS have increased for laryngeal and pharyngeal lesions. 3 To our knowledge, this is the first report of TORS for lesion located in the posterior surface of soft palate. As described for nasopharyngeal and skull base TORS,4,5 to provide the best visualization of the lesions, the robot has to be at the patient’s head for allowing the greatest mobility of the surgical tools in the oro- and nasopharyngeal spaces. This kind of robot placement and exposition allows a great view of the nasopharyngeal cavity and of the sphenoid sinus floor.
In the high majority of cases, our patient tumor would have been treated by radiotherapy. 1 The strength of our technique is the realization of an effective surgical treatment for early stage OSCC without use of radiotherapy. The patient who benefited from TORS resection of soft palate tumor avoids the side effects of radiotherapy or the usual complication of open surgery (eg, infection, bleeding, or fistula). Compared with open surgery, our approach is associated with shorter hospital stay and a theoretical lower risk of complications.
Conclusion
The resection of early stage OSCC of the posterior surface of soft palate is possible through TORS. The procedure is noninvasive, rapid, and seems to be associated with excellent functional outcomes. Future cohorts of patients are needed to confirm the effectiveness and safety of the TORS resection of OSCC of the posterior surface of soft palate.
Footnotes
Authors’ Note
S.H., J.R.L., and E.C. contributed study concept and design; drafting of the manuscript; and administrative, technical, or material support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.