
Abstract
Immunoglobulin G4-related disease (IgG4-RD) is a chronic inflammatory disease involving multiple organs. Some studies have reported otological manifestations of IgG4-RD, although most studies describe involvement of the middle ear, and reports on inner ear manifestations are limited. Here, we describe a case of a 30-year-old man with IgG4-RD involving the inner ear. This case demonstrated that IgG4-RD affected the inner ear and caused cochlear ossification. Cochlear implants may be considered for milder cases, and hormone and immunosuppressive therapy may control disease progression.
Introduction
Immunoglobulin G4-RD (IgG4-RD) is a systemic disease that involves many tissues such as the pancreas, lacrimal glands, and salivary glands. However, otological manifestations of IgG4-RD are rare and clinical features of IgG4-RD with ear involvement remain relatively unknown, especially those concerning the inner ear. Diagnostic criteria of IgG4-RD are as follows: elevated serum IgG4 level, IgG4+ in >40% of IgG+ plasma cells, and >10 cells per high powered field (HPF) in biopsies, presence of 1 or more characteristic lesions, and the exclusion of other diseases. 1 However, most patients with IgG4-RD are atypical and it remains a challenge to correctly diagnose IgG4-RD with rare organ involvement. Here, we reported a case of otological IgG4-RD and conducted a literature review to discuss the clinical features of IgG4-RD with ear involvement.
Case Report
A 30-year-old patient was admitted to the local hospital and presented with 7 months of continuous otorrhea and progressive hearing loss in both ears. Earache, bleeding, and itching were not found after further inquiry. Routine blood tests including erythrocyte sedimentation rate and C-reactive protein showed no abnormalities. An otoscopic examination revealed that the external auditory meatus on both sides was moist with an obscured tympanic membrane and full of granuloma. The pure tone average (PTA) of the left ear from 500 Hz to 2 kHz frequencies was 43.3 dB with a bone conduction of 10 dB, and the PTA of the right ear was 51.7 dB with a bone conduction of 11.7 dB. Computer tomography (CT) examination of the temporal bone revealed tympanic cavities on both sides and a soft tissue density shadow in the mastoid process, indicative of chronic suppurative otitis media. A right mastoidectomy and type III tympanoplasty were subsequently performed. Microscopic examination during the operation revealed a dark red papillary neoplasm deep within the external auditory canal and tympanic cavity. Concurrently, cholesterol granulomas were detected in the tympanic antrum and the surrounding air chambers. We subsequently removed the lesions from the tympanic cavity and the external auditory canal. Clinical pathology determined a chronic inflammation of the squamous and columnar mucosa with papillomatous hyperplasia and revealed elevated proportions of IgG4+ plasma cells. Immunohistochemical analyses indicated >50 CD138+ IgG4+ plasma cells per HPF and an IgG4+/IgG+ ratio of >40%, confirming the diagnosis of IgG4-RD. Postoperative facial nerve function was normal, although the patient’s hearing did not improve.
The patient was referred to the Department of Rheumatology for further treatment and the patient’s serum IgG4 concentration was elevated (378 mg/dL, normal range: 8-140 mg/dL). Therefore, the patient received glucocorticoids and immunosuppressive treatment consisting of 40 mg prednisone and 100 mg cyclophosphamide daily. Serum IgG4 concentration gradually decreased to normal levels, but hearing impairment continued to persist. After 6 months, the patient suddenly exhibited complete deafness in both ears. The CT examination established bilateral tympanic cavities as before paired with a soft tissue density shadow in the mastoid process and external acoustic meatus (Figure 1A). Auditory brainstem response showed that neither ear achieved the maximum evoked potential. Magnetic resonance imaging of the temporal bone revealed complete ossification of the left cochlea (Figure 1B). According to previous literature, cochlear ossification is primarily caused by trauma, inflammation, and immune disorders. However, the patient’s medical history and examinations excluded previous diseases capable of causing cochlear ossification. Thus, the final diagnosis was otological IgG4-RD involving the inner ear and we recommended cochlear implantation as the treatment strategy. Preoperative temporal bone CT scan indicated opacification of the mastoid air cells and the middle ear cavities on both sides as well as extensive bony erosion of the ossicular chain. Furthermore, the modiolus of the left cochlea was missing and we observed complete ossification of the left cochlea while the right cochlea was normal (Figure 2). We implanted a MED-EL CONCERTO with a standard electrode in the right cochlea using a retrofacial recess approach, and the patient was given postoperative antibiotic therapy. However, the patient returned with otalgia of the right ear 4 days after surgery. The iodoform yarn was removed and a swab was taken from the deep part of the ear for culture, which revealed the presence of Pseudomonas aeruginosa, a multidrug-resistant bacterium that is sensitive to imipenem (minimal inhibitory concentration: 19 µg/mL). Imipenem treatment significantly relieved the patient’s discomfort and a CT scan 5 days after surgery showed successful implantation. The implant continued to function normally 1 month after surgery and improved the patient’s hearing. A 3-month postoperative CT scan showed stabilization of the lesions.
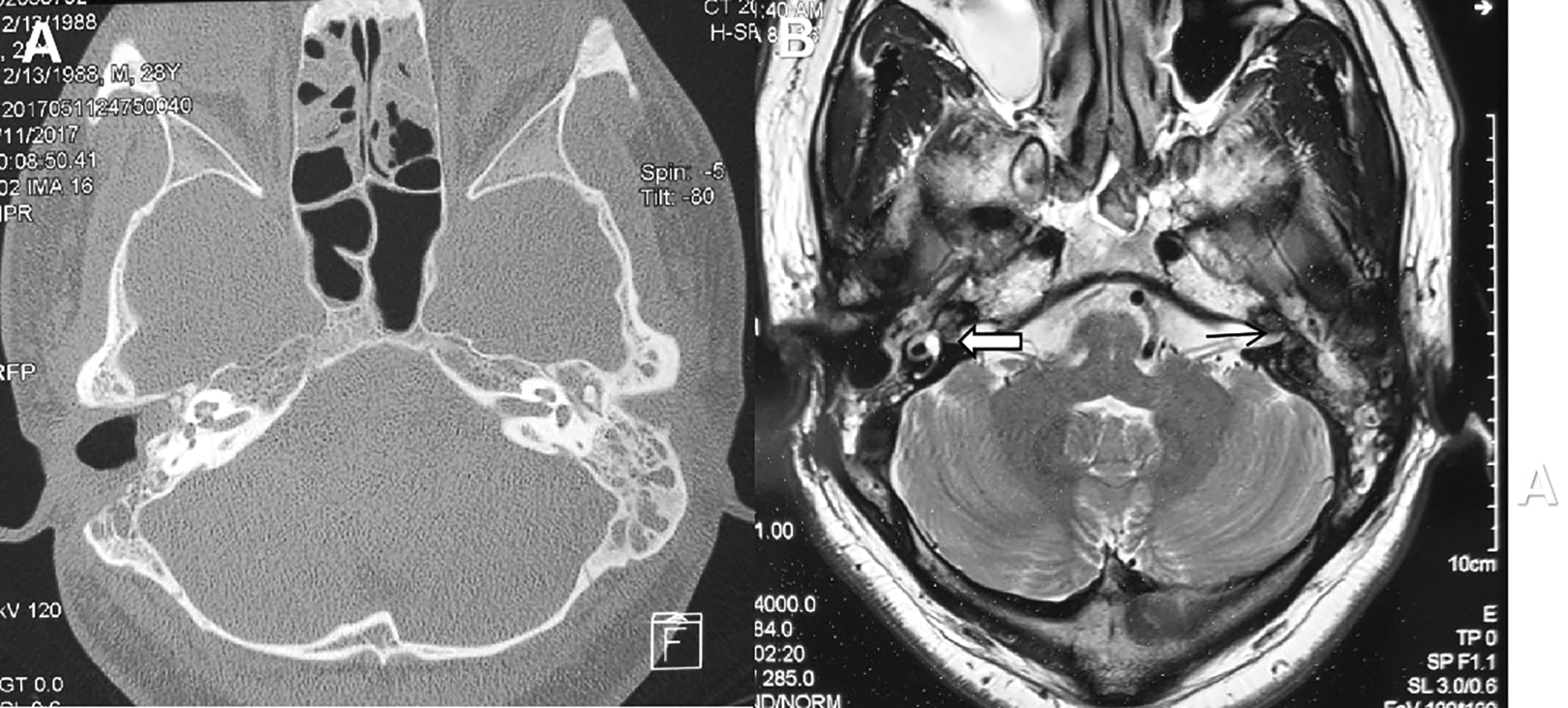
A, Computed tomography scan of the temporal bone after mastoidectomy and before cochlear implantation. B, T2-weighted MRI of the temporal bone before cochlear implantation. The thin black line indicates the left membranous labyrinth, which cannot be imaged by MRI, and the thick white arrow shows the right membranous labyrinth. MRI indicates magnetic resonance imaging.
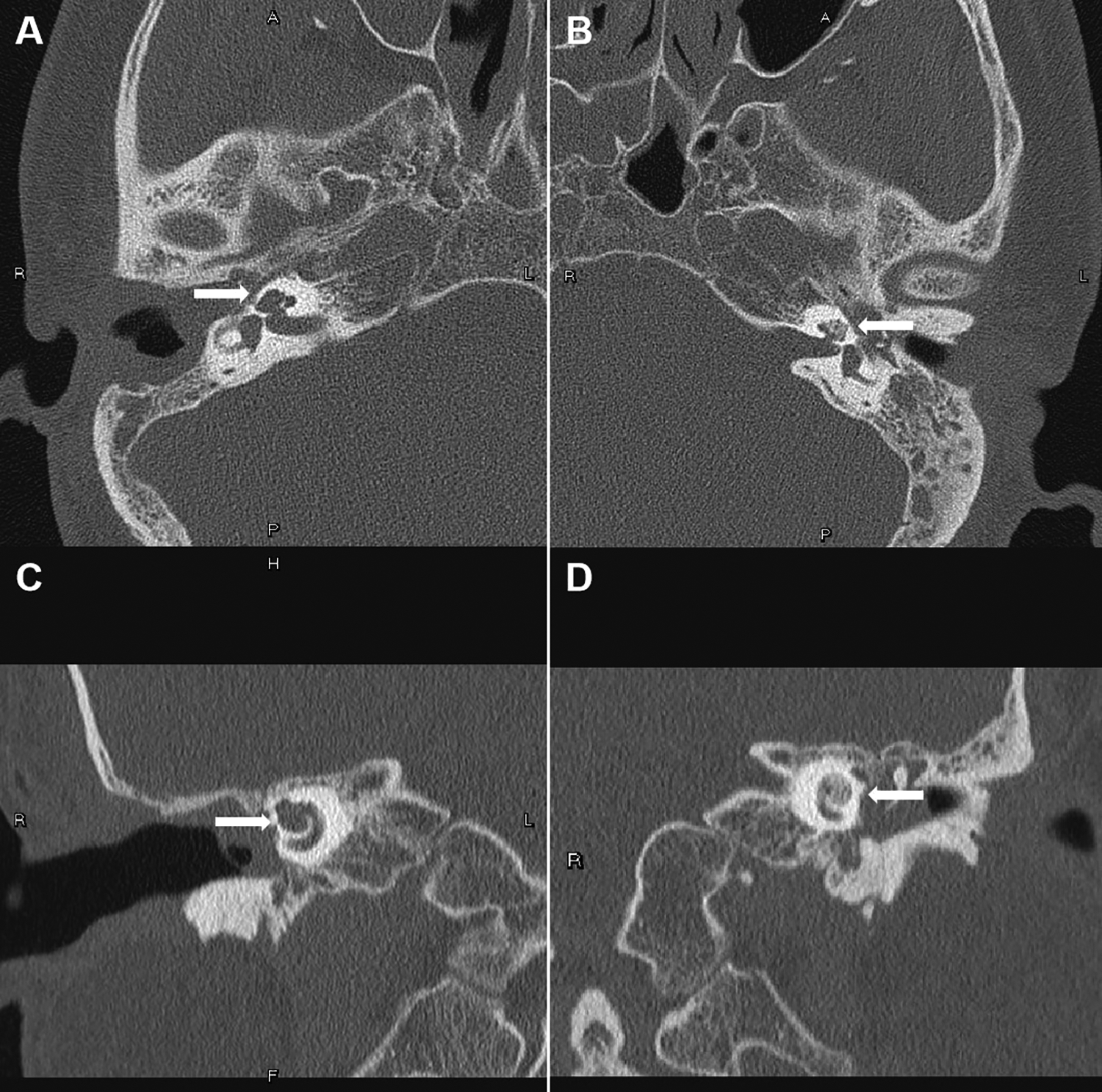
Computed tomography scan of the temporal bone before cochlear implantation. Axial CT scan of the (A) right ear and (B) left ear. Coronal CT scan of the (C) right ear and (D) left ear. The arrow indicates a high-density area in the left cochlea, which was evidence of cochlear ossification and was absent in the right cochlea. CT indicates computed tomography.
Discussion
Masterson et al 2 reported the first case of otologic manifestations of IgG4-RD in 2010, and an increasing number of reports have appeared since. Takagi et al described a prevalence of 12.8% (5/39) for otological IgG4-RD, of which 4 cases had associated sinus symptoms and middle ear exudation without granuloma and all cases presented with elevated serum IgG4. We reviewed the literature on otological IgG4-RD and found 22 reported cases.2-15 According to these case studies, otological IgG4-RD consists of progressive hearing loss, otalgia, tinnitus, and vertigo. Recurrent mastoiditis, 7 secretory otitis media, 1 otorrhea, 10 and facial numbness 11 are the main clinical symptoms. If the lesion is confined to the middle ear, which consists of the tympanum, eustachian tube, and mastoid cavity, it typically only causes conductive hearing loss. Once the lesion expands to the inner ear or intracranial tissue, it often leads to profound sensorineural deafness with symptoms such as vertigo, tinnitus, and headache. Of these 22 cases, only 4 cases had involvement of the inner ear, including 3 affecting the lateral semicircular canal and 1 involving the cochlea. Moreover, cases of exclusive otological IgG4-RD without affecting other organs are rare. Treatments in most cases include surgery, steroids, and immunosuppressive therapy, although some patients require targeted therapy, antibiotics, or radiotherapy to alleviate the symptoms.
Unlike cochlear spiral plate ossification, 11 the complete cochlear ossification in our patient has not previously been reported for IgG4-RD. The relationship between cochlear ossification and IgG4-RD is unclear. The current theory is that infection leads to the activation of pattern recognition receptors on the surface of antigen-presenting cells, which in turn activate CD4+ T cells to differentiate into Th1, Th2, Treg, and Tfh cells. These subsequently secrete their respective cytokines and promote B cell activation and transformation into plasma cells to produce IgG4. Formation of fibrosis is promoted by transforming growth factor β and platelet-derived growth factor produced by macrophages and Treg cells. 16 Development of fibrosis in the inner ear may lead to cochlear ossification, resulting in sensorineural hearing loss.
Our patient’s symptoms were relieved after hormone and immunosuppressive therapy. However, the patient was infected by P aeruginosa after surgery, which indicated that postoperative antibiotic therapy was necessary.
Conclusion
Immunoglobulin G4-RD may exclusively affect the ear, in which the middle ear is involved in most cases and the inner ear is rarely affected. The cochlear ossification discovered in our case study revealed that the cochlea may be a target organ in IgG4-RD. Antibiotic therapy may be necessary after surgery due to hormone and immunosuppressive treatments.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.