
Abstract
Prostate cancer (PC) is prone to bone metastases, but very rarely it can spread to soft tissues. In the head and neck region, PC can metastasize to the orbital soft tissue, causing various symptoms such as vision loss. In this report, we describe the case of a 79-year-old man with PC metastasis in the orbital apex. He presented to an ophthalmologist at our hospital with progressively worsening vision in his left eye over 3 to 4 months. He complained of a drooping eyelid in the same eye; thus, intracranial disease was suspected. Closer inspection with head computed tomography revealed a space-occupying lesion from the orbit to the posterior ethmoid sinus, and he was referred to our department. He had a history of PC, and we performed endoscopic sinus surgery for the diagnosis of malignancy, including metastasis of PC. As a result, the mass was diagnosed as PC metastasis by pathological examination. The patient began androgen blockade therapy and 3 months postoperatively, magnetic resonance imaging revealed that the extraconal orbital mass had decreased significantly. It is important to determine the metastases of PC in the paranasal region when the patient has a preexisting medical history.
Introduction
Prostate cancer (PC) is a common cancer in men. In most patients with PC, the cancer spreads slowly; however, it can sometimes be fatal due to rapid progression. 1 The most common treatments include surgical prostatectomy, radiation therapy, chemotherapy, and androgen blockade therapy. 2 Prostate cancer often metastasizes to bone, but there are some reported cases of metastasis in soft tissues such as the liver and lungs with prolonged survival with treatment.3,4 We recently encountered a rare case of a 79-year-old man with PC that metastasized within the orbit and then invaded the sinus cavity; therefore, we report this case along with a review of the literature.
Case Report
A 79-year-old man presented to the ophthalmology department of our hospital with progressively worsening vision in his left eye over 3 to 4 months. He also complained of drooping eyelid in the same eye. The ophthalmologist performed a comprehensive eye examination and revealed that he had decreased visual acuity but no apparent oculomotor disturbance or elevated intraocular pressure (critical fusion frequency score: right = 38 Hz, left = not measurable). Considering these results, he was referred to an internist due to suspicion of intracranial disease, and computed tomography (CT) of the head showed a hypointense, soft tissue mass lesion in the left orbit. This mass was observed to extend and break through the lamina papyracea into the posterior sinus. The superior rectus muscle was deviated to the left, and opacification of the optic nerve at the orbital apex was observed. The intraorbital mass effect was enhanced with contrast material-enhanced CT (Figure 1A and B). Subsequently, the patient was referred to our department.
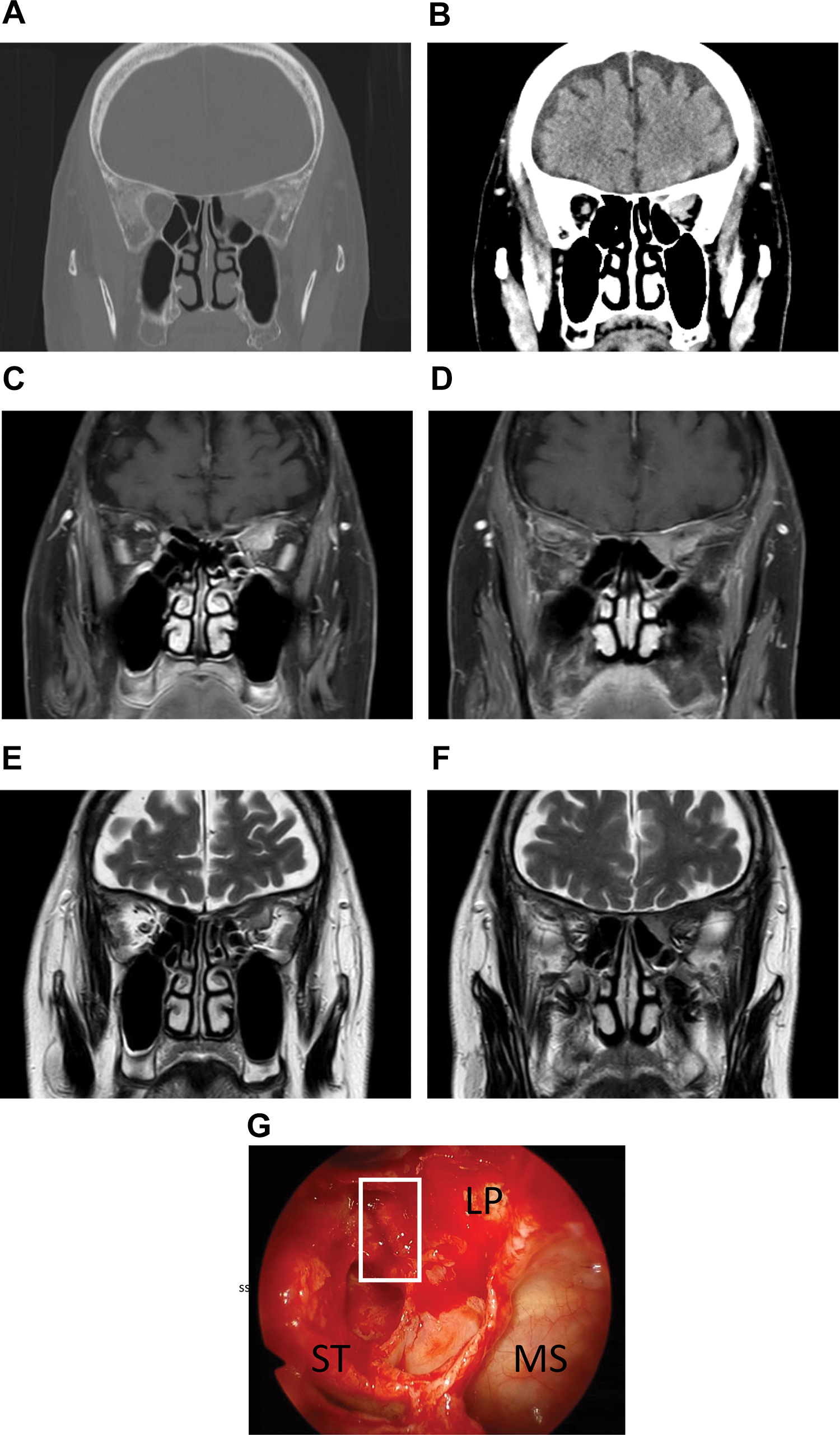
Preoperative contrast-enhanced CT image, MRI images, and surgical findings. A, The superior rectus muscle deviated to the left, and opacification of the optic nerve was seen at the orbital apex. B, The intraorbital mass effect was enhanced with contrast material-enhanced CT. C, Intraorbital soft tissue mass lesions produced high-intensity signals on T1-weighted images by contrast-enhanced MRI. D, The tumor in the posterior ethmoid sinus was less enhanced. E, T2-weighted images showed low-intensity signals produced by all parts of the tumor in the left orbit. F, Similar low intensity signals were detected in posterior ethmoid sinus. G, Within the posterior ethmoid sinus, there was a bone defect in the LP. A biopsy of the tumor (white square) was performed at the same site. CT indicates computed tomography; MRI, magnetic resonance imaging; LP, lamina papyracea; MS, maxillary sinus; ST, superior turbinate.
The patient’s general condition was good, and physical examination revealed no acute distress. He had a history of PC, and blood examination revealed the prostate-specific antigen (PSA) value was 755.43 ng/mL. No significant findings (eg, nasal discharge or nasal tumor) were observed by nasal endoscopy. Contrast-enhanced magnetic resonance imaging of the head revealed that the intraorbital soft tissue mass lesions produced a high-intensity signal on T1-weighted images and a low-intensity signal on T2-weighted images. Tumors in the posterior ethmoid sinus tended to have a weak contrast effect (Figure 1C, D, E, and F).
Based on these considerations, endoscopic sinus surgery was performed for diagnostic purposes. Upon release of the posterior ethmoid sinus, the lamina papyracea was partially destructed and there was a nodular lesion extending to the same area. An incision was made in the periosteum, and a biopsy was performed on the internal massed lesion (Figure 1G). After the intraoperative diagnosis of poorly differentiated carcinoma was obtained, a permanent specimen was collected and the surgery was completed.
The specimen showed atypical cells with clarified nucleoli and an increased nucleus to cytoplasm ratio on hematoxylin-eosin staining and was considered an adenocarcinoma. Immunohistochemical analysis revealed that the tumor tissue was stained with pan cytokeratin (AE1/AE3) (+), cytokeratin (CK) 7 (−), CK20 (−), and PSA (+); therefore, the findings were consistent with PC metastasis. The patient’s postoperative course was good, and he was discharged from the hospital on the eighth postoperative day with a partial improvement in visual acuity. The patient was treated with antiandrogens, and at 3 months postoperatively, there was a marked reduction in the size of the mass on imaging (Figure 2).
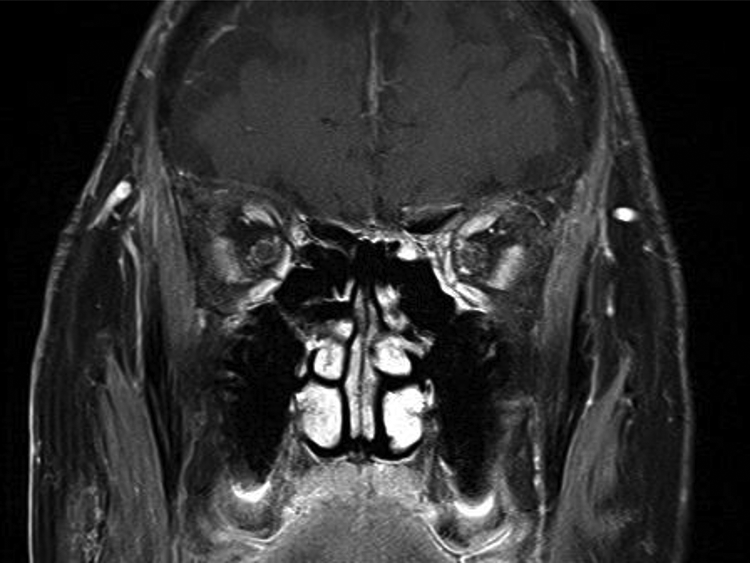
Postoperative MRI. The tumor size was smaller after hormone therapy. MRI indicates magnetic resonance imaging.
Discussion
Bone metastasis in PC is common, however, some reports on soft tissue metastasis also exist. 5 Adenocarcinoma of the prostate is implicated in 3.6% to 4% of all orbital metastases; among them, metastases to the uvea have been commonly reported.6-8 In very rare cases, metastases to the external rectus muscle and the optic nerve tract have been indicated. 9 When the disease metastasizes to the orbit, symptoms such as decreased vision, impaired eye movement, diplopia, and increased intraocular pressure are observed due to compression of the intraorbital tissue.
In the present case, the patient had significant vision loss. In contrast, eye movement disorder, blurred vision, and elevated intraocular pressure were mild; therefore, we initially attributed the loss of vision to partial tumor invasion of the optic nerve. However, vision loss was partially improved after the surgery; thus, decompression by sinus release had a certain effect. These results suggest that vision loss was not only due to nerve invasion of the tumor but also due to nerve compression. There was also some thickening of the superior rectus muscle, but the likelihood of metastasis was considered to be low based on the fact that there was no strong eye movement disorder.
In this case, the cranial base metastasis may have metastasized to the orbit, but the intraorbital lesion was the predominant locus on images, and it is more likely that intraocular soft tissue metastases invaded the posterior ethmoid sinuses. In addition, most of the intraorbital masses showed an irregular enhancement upon gadolinium-diethylenetriamine-pentaacetic acid administration, but the posterior ethmoid sinus had a slightly different image. For this reason, as a rapid assessment of the posterior ethmoid sinus tissue was not sufficient to diagnose malignancy, we planned to perform a biopsy of the intraorbital masses by excising the lamina papyracea with anterior and posterior artery clipping, as well as using external incisions. The main treatment for intraorbital metastases of PC is antiandrogen and radiation therapy.10,11 In the case of metastasis to the choroid plexus, hormone therapy may contribute to tumor regression. In this case, hormone therapy was also chosen, and at 3 months postoperatively, the tumor had markedly shrunk.
In conclusion, we encountered a case in which a nasal cavity biopsy was used to diagnose PC metastasis. Although very rare among neoplastic lesions extending into the sinuses, this case suggests that PC metastasis should also be considered.
Footnotes
Authors’ Note
K.W. contributed to concept; T.T. contributed to design; H.N. and Y.M. contributed to supervision; K.W. contributed to materials, K.M. and Y.H. contributed to analysis and interpretation. Written informed consent was obtained from the patient for using the data in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.