
Abstract
Hurthle cell tumors are rare follicular-derived thyroid neoplasms. Hurthle cell tumors may be benign or malignant. Workup includes imaging, fine needle aspiration, and treatment usually consists of observation versus thyroidectomy. We describe a case of Hurthle cell adenoma in an adolescent; to the best of our knowledge, this represents only the third case described in the English literature of adolescent Hurthle cell adenoma.
Introduction
Hurthle cell tumors (HCTs) are rare follicular-derived thyroid neoplasms. They may be characterized as an adenoma or carcinoma. The majority of HCTs are benign. First described in 1907, Langhans described a series of 5 patients with thyroid masses that were mainly composed of oncocytes. Using the surveillance, epidemiology, and end results database, Bhattacharyya 1 reports that HCTs are more common in women (68%) and commonly occur in the 6th decade of life. Male sex, increasing age at presentation, and tumor size were all associated with poor survival. 1 Imaging and fine needle aspiration (FNA) are usually obtained and treatment usually consists of removal by thyroidectomy. We describe a case of Hurthle cell adenoma (HCA) in an adolescent; to the best of our knowledge, this represents only the third case described in the English literature of adolescent HCA.
Case
A previously healthy, 18-year-old female presented to the emergency department with a new neck mass. She was in no acute distress and the neck mass had been incidentally noted by her mother. She denied any neck or throat pain, fevers, trouble swallowing or trouble breathing, or upper respiratory symptoms. The patient did report “hot flashes,” sudden episodes in which she felt very hot and sweaty, and heat intolerance that started a couple of years ago. She also reported that she often felt comfortable or hot when others were feeling cold.
On examination, she had visible swelling and symmetry of the left side of her neck. There were no bruits and she had no stridor or shortness of breath. She had a magnetic resonance imaging (MRI) and representative pictures are shown in Figure 1. The MRI demonstrated a 5.9 × 4.4 × 3.7 cm mass as measured in the craniocaudal, transverse, and Antero-posterior (AP) dimensions, in the region of the left thyroid lobe that is predominantly T2 hyperintense with diffuse internal contrast enhancement. The mass was heterogeneous on T2-weighted images.
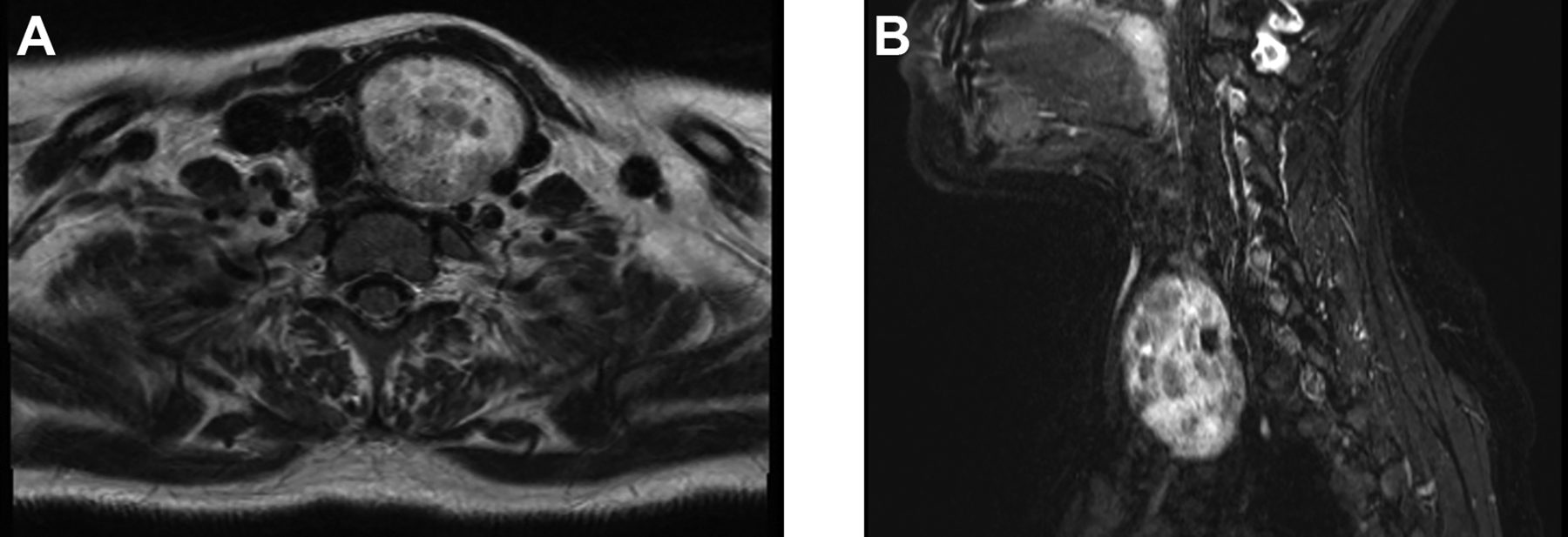
A, Axial magnetic resonance imaging (MRI) of the neck. B, Sagittal MRI of the neck.
She subsequently had a fine needle biopsy which showed rare clusters of cells with cytological atypia but was negative for nuclear features of papillary carcinoma, please see Figure 2. She was also noted to be hyperthyroid and treatment with methimazole was initiated by the endocrine team. Her hyperthyroidism was medically managed, and she underwent a left hemithyroidectomy. The left thyroid lobe excision showed involvement by a dominant encapsulated Hurthle cell neoplasm. The tumor shows a mixed macro and microfollicular growth pattern with oncocytic features. In the submitted sections, no invasive features were identified. The findings are most compatible with the diagnosis of a HCA.
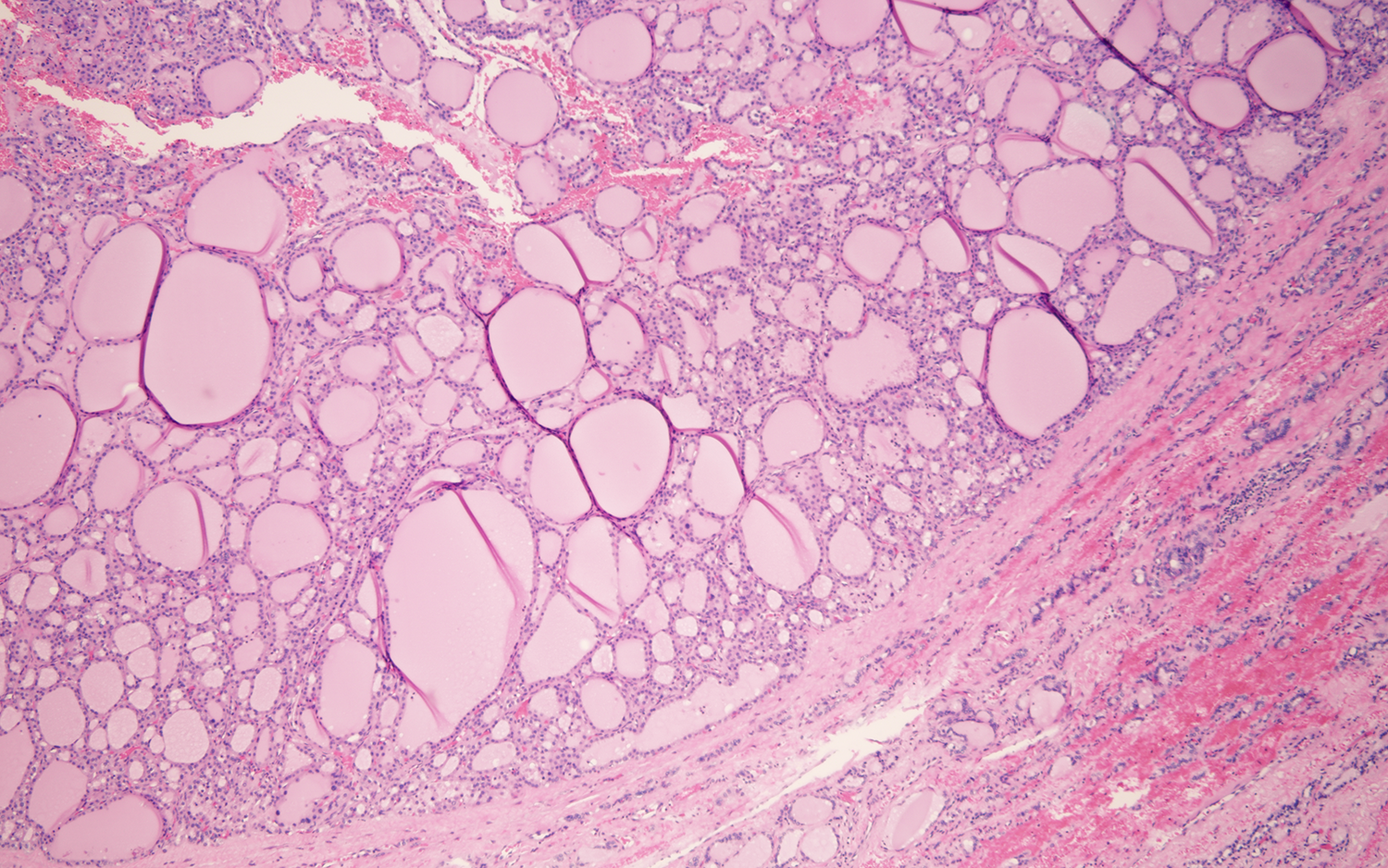
Low power pathology: H&E stain showing mixed macro and microfollicular growth pattern without invasive features.
Discussion
Hurthle cell tumors comprise less than 5% of all thyroid tumors. 2 Hurthle cells are follicular-derived, mitochondria-rich, thyroglobin-producing cells with abundant eosinophilic cytoplasm 3 and can be diagnosed using FNA.4-6 But, while FNA can direct surgical approach, it is unable to detect invasion, and therefore, cannot differentiate between HCA and Hurthle cell carcinoma (HCC).4,6 Most HCTs are benign (HCA) but up to 40% have been reported to be malignant (HCC). 7 Surgical histopathology has high diagnostic accuracy and is the gold standard for confirming HCA.5,8 Hurthle cell adenoma most commonly localizes unilaterally and is treated via hemithyroidectomy.5,6 In contrast, HCC can be bilateral and more aggressive, so it is treated by total thyroidectomy.5,6 Even though surgery is associated with increased complications in children, surgery is the most effective route of treatment due to the increased cancer risk, when compared with adults. 4 A 2007 case report by Bremer et al reported a 12-year-old female as the youngest known case of HCA. 2 The patient presented with a 2 × 2 cm smooth, firm nodule in the inferior region of the right thyroid gland. The remainder of the patient’s physical examination was normal, and she presented with no known risk factors. The patient underwent right thyroid lobectomy and isthmusectomy. Her postoperative period was uneventful and has since remained euthyroid and normocalcemic. 2 A 2016 case report by Kochummen et al recorded a 14-year-old female as the first reported pediatric case of bilateral HCA. 5 At initial presentation, the patient’s only symptom was a palpable thyroid. After being lost to follow-up for 14 months, the patient returned with euthyroid function and symptoms of neck swelling, dysphagia, diaphoresis, palpitations, and weight loss. Repeat ultrasound showed that 1 of the 3 nodules in the right lobe had increased by 0.2 cm, but all other nodules had remained stable. Computed tomography (CT) scan then showed a heterogeneously enhancing 3.2 × 2.2 cm mass in the left and an unremarkable right lobe. The final recommendation was left hemithyroidectomy. One year later, at follow-up, repeat ultrasound showed the right-sided nodule had doubled in size to 1.6 cm and a right hemithyroidectomy was performed. Histopathologic analysis after both surgeries confirmed HCA. The patient is currently biochemically euthyroid with medication-controlled hypoparathyroidism and hypothyroidism. 5
Although MRIs, CTs, ultrasounds, and FNAs can aid in the diagnosis of neck masses and thyroid nodules, surgical histopathology remains the gold standard for confirming the diagnosis of HCA. As seen in the 3 patients mentioned, patients can initially present with a benign physical examination; therefore, while rare, HCA should be considered during a differential. Further, benign-appearing thyroid nodules in adolescents should be monitored over time, as the course of HCA can be unpredictable and even present bilaterally.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.