
Abstract
Significance Statement
Unilateral Eagle Syndrome is relatively rare and highlights important concepts in anatomy and pathophysiology. Bilateral Eagle Syndrome is exponentially more rare and has only been mentioned several times in the literature. Understanding the impact this can have on the human body and the severity of symptoms and sequelae is valuable for several types of specialists that treat this disorder.
Pathology Clinic
A 40-year-old female presented to her general practitioner complaining of pain on chewing, swallowing, and painful left lateral head and neck movement. On palpation, the tonsillar fossae revealed longer than average styloid processes. Lateral X-rays of the neck confirmed bilaterally elongated styloid processes (Figure 1). Bilateral elongation of styloid processes, or Eagle Syndrome, is exceedingly rare. The patient was referred to the Oral and Maxillofacial Surgery clinic for treatment. She elected to have her left styloid process removed. Surgery was performed with disarticulation from the tympanic plate and excision from the hyoid cartilage. Surgical pathology received a specimen measuring 4.0 × 3.7 × 0.2 cm that had a globular proximal articular surface, and a serrated distal end (Figure 2).

Lateral neck X-ray. The elongated styloid process extends from the tympanic plate of the temporal bone to the hyoid cartilage.

A whole mount, nonmagnified slide of the elongated styloid process.
Following decalcification, microscopic findings revealed an elongated microscopically benign styloid process that was bony, except for the cartilaginous proximal end and central hematopoietic area (Figure 3). The patient recovered well from surgery, but 7 months later still complained of left-sided jaw pain. At the time, she was found to have 3 herniated discs between C2-3, C5-6, and C6-7 and left-sided thoracic outlet syndrome, attributed to muscle tension.
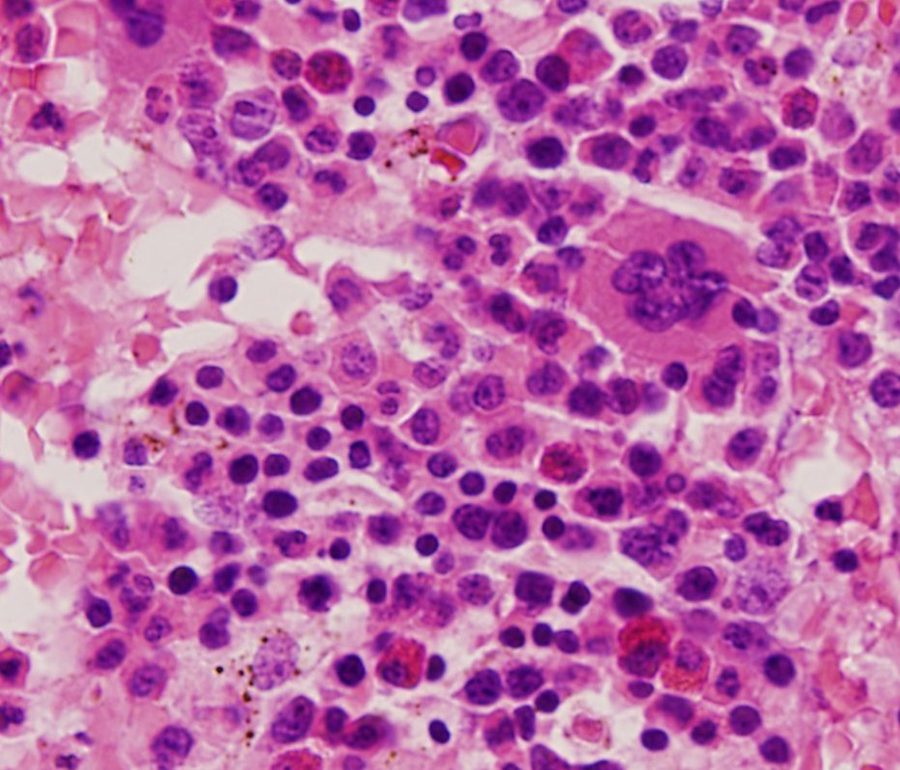
The bone marrow has unremarkable trilineage hematopoiesis, ×400 magnification.
According to Gray’s Anatomy, 1 the normal styloid process is 2.5 cm in length and may manifest distally as a ligamentous structure, the stylohyoid ligament. As exemplified in this case, this structure may undergo ossification. Pathological elongation has been designated as the Eagle syndrome (ES) and may result in pain or discomfort on chewing, swallowing, or movement of the neck. Symptoms tend to manifest after the process exceeds 3.0 cm.
The incidence of symptomatic ES in the general population is 0.16%, and only rare bilateral examples have been observed.2,3 It is of additional interest that ES has recently been associated with hepatolineal (liver and spleen) fusion.4,5 Because of the compact space in which the styloid presides, ES can present with a variety of manifestation. The 2 most common are classical Eagle (Stylohyoid) syndrome and stylocarotid syndrome. The former presents with what has been termed “stylalgia.” This is from compression of cranial nerves V, VII, IX, and/or X as well as its branches, and results in pain over the face as well as with swallowing, and a foreign body sensation in the throat. Alternatively, Stylocarotid syndrome may result from compression of the carotid artery, leading to visual disturbances, facial pain, and possibly syncope. 6
Due to its rarity, ES must be carefully distinguished from glossopharyngeal neuralgia, which may also present with pain at the angle of the jaw. This pain is usually paroxysmal rather than movement related. Imaging and physical examination can be used to distinguish tumors in this region from ES. 7
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.