
Abstract
Background:
An outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 infection occurred in Wuhan, China, in December 2019. To date, the analysis of fatal cases and the risk factors for death have rarely been reported.
Methods:
In this study, 220 adult patients with confirmed and suspected COVID-19 were enrolled. Clinical characteristics, laboratory data, treatments, and complications were compared between 168 survivors and 52 nonsurvivors. Univariable analysis and multivariable logistic regression were used to investigate the risk factors for mortality.
Results:
A total of 220 patients (168 were discharged and 52 died in the hospital) were enrolled in the study. The median age of all patients was 59.5 (47.0-69.0) years, and the median age of patients who died was significantly older than that of patients who survived (70.5 vs 56.0 years, respectively; P < .001). According to multivariate logistic regression, older age (odds ratio: 1.09, 95% CI: 1.03-1.15; P = .001), initial Sequential Organ Failure Assessment (SOFA) score >2 (37.4, 9.4-148.0; P = .011), and respiratory rate >24 per minute (10.89, 1.47-80.67; P = .019) were independent risk factors for mortality.
Conclusion:
Clinical and laboratory parameters predicting poor prognosis including older age, baseline SOFA score >2, and respiratory rate >24 per minute were identified.
Introduction
In December 2019, a new coronavirus that causes acute pneumonia was isolated from patients in Wuhan, China. The virus was subsequently named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The disease has a high fatality rate and has several clinical features that resemble the disease caused by infection with severe acute respiratory syndrome coronavirus (SARS-CoV). As such, there has been concern that the virus has the potential to cause a pandemic. Researchers around the world have been studying this virus. The epidemiological and clinical characteristics of the disease have been reported, and the overall mortality rate of this disease is high, especially in critically ill patients. 1 -6 The risk factors for death in patients with this disease remain to be elucidated. We aimed to compare the clinical characteristics between survivors and nonsurvivors, and to explore the risk factors predicting death.
Method
Study Design
We retrospectively studied 220 patients including 52 nonsurvivors and 168 discharged patients between January 11, 2019, and February 18, 2020, from Wuhan No.7 Hospital, which was temporarily taken over by Wuhan University Zhongnan Hospital during the coronavirus disease 2019 (COVID-19) outbreak. All patients were diagnosed with COVID-19 according to the Novel Coronavirus Pneumonia Diagnosis and Treatment Programme (seventh edition) published by the National Health Commission of China. The results of tests for SARS-CoV-2 RNA from throat-swab specimens were not available in the hospital information system in early January, 2020. Eleven of 52 nonsurvivors and 52 of 168 survivors in this study had no nucleic acid results or negative nucleic acid results. These suspected patients were diagnosed based on epidemiology, symptoms, and computed tomography according to the Chinese management guidelines (trial version 7).
This research was approved by the research ethics commission of Wuhan University Zhongnan Hospital (No. 2020042). The ethics commission approved the application for exemption from the requirement to attain informed consent.
Data Collection
The data collected included demographics, clinical symptoms, comorbid conditions, laboratory findings, arterial blood gas values, clinical classification, SARS-CoV-2 RNA detection results, respiratory rate on admission, treatment (including antiviral therapy, antibiotics, corticosteroid therapy, and oxygen support), and time course of the illness. Laboratory results including the white blood cell counts, lymphocyte counts, platelet counts, prothrombin time,
Statistical Analysis
Continuous and categorical variables are presented as the median (interquartile range) and n (%), respectively. We used the Mann-Whitney U test, χ2 test, or independent sample t test to compare differences between survivors and nonsurvivors. Univariable and multivariable logistic regression analyses were used to explore risk factors for mortality. Given the limited sample size (52 deaths) and the need to ensure the stability of the multivariable logistic regression model, 5 variables were included in the analysis. Our model included age, comorbidity, SOFA score, respiratory rate, and lymphocyte count based on previous studies and the availability of data. A P value less than .05 was considered statistically significant. SPSS (version 26) was used for all statistical analyses.
Definitions
Fever was defined as an axillary temperature over 37.3 °C. The clinical classification of COVID-19 was defined according to the Chinese management guidelines (trial version 7). 7 Septic shock was defined according to the 2016 Third International Consensus Definition for Sepsis and Septic Shock. 8 Acute respiratory distress syndrome (ARDS) was defined according to the Berlin definition. 9 Acute cardiac injury was defined as a cTnT level above the upper limit of normal. Acute myocardial infarction (AMI) was diagnosed according to the 2017 ESC guidelines for AMI. 10 Acute kidney injury was defined according to the KDIGO clinical practice guidelines. 11 Arrhythmia included bradycardia, tachycardia, premature contraction, atrial fibrillation, and supraventricular tachycardia. Abnormal liver function was diagnosed if the liver enzyme levels were above the upper limits of normal. Gastrointestinal hemorrhage was defined as positivity for occult blood in gastric juice and the exclusion of other causes of a reduction in the level of hemoglobin.
Results
Demographic and Clinical Characteristics
This study population included 220 adult patients with COVID-19 who were admitted to Wuhan No. 7 Hospital from January 11, 2020, to February 18, 2020. A total of 168 patients were discharged and 52 patients died during hospitalization.
The median age of the patients who died was significantly older than that of the surviving patients (70.5 vs 56.0 years, respectively; P < .001; Table 1). There was significant difference in the sex distribution between survivors and nonsurvivors (P < .001) and most nonsurvivors were male. The smoking prevalence was higher among nonsurvivors than among survivors (19.2% vs 6.0%, respectively; P = .04). However, there were no differences in alcohol consumption, time from illness onset to admission, or time from symptom onset to viral shedding. A total of 54.1% of patients had comorbidities with hypertension, diabetes, and cardiovascular disease being the most common comorbidities. Hypertension, diabetes, cardiovascular disease, cerebrovascular disease, chronic obstructive pulmonary disease, carcinoma or chemotherapy, and chronic renal failure were more common in the nonsurviving group than in the surviving group (P < .05).
Clinical Characteristics, Classification, Time Course of Illness of Patients With COVID-19.a
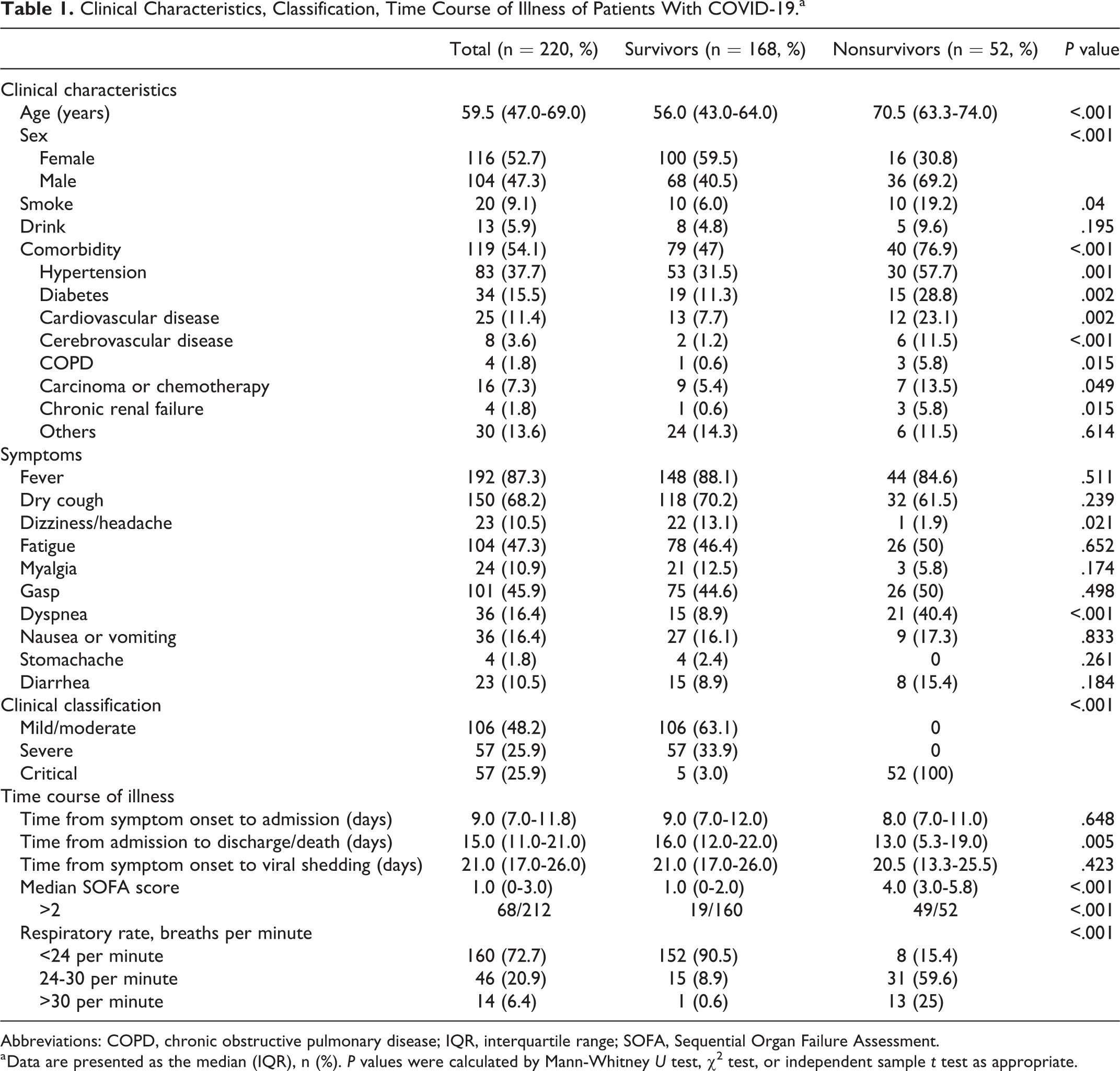
Abbreviations: COPD, chronic obstructive pulmonary disease; IQR, interquartile range; SOFA, Sequential Organ Failure Assessment.
a Data are presented as the median (IQR), n (%). P values were calculated by Mann-Whitney U test, χ2 test, or independent sample t test as appropriate.
The most common presenting symptoms were fever (87.3%), dry cough (68.2%), fatigue (47.3%), and gasping (45.9%). The prevalence of dyspnea on admission in the nonsurviving group was higher than that in the surviving group (P < .001). Nearly half of the patients had mild/moderate COVID-19. The surviving patient group mainly consisted of mild/ moderate and severe patients, while the nonsurviving patient group was composed of all critically ill patients (Table 1).
Sepsis, acute liver injury, acute cardiac injury, and ARDS were the most common complications. The incidence of complications was higher in nonsurviving patients than in surviving patients (Table 2) with sepsis (100%) and acute cardiac injury (96.2%) being the most common complications in nonsurvivors. The incidence of arrhythmia in nonsurvivors was also higher than that in survivors. A few nonsurviving patients developed severe complications such as AMI and pneumothorax. Furthermore, 8 of the 52 nonsurvivors experienced gastrointestinal hemorrhage.
Complication and Treatment of Patients.a
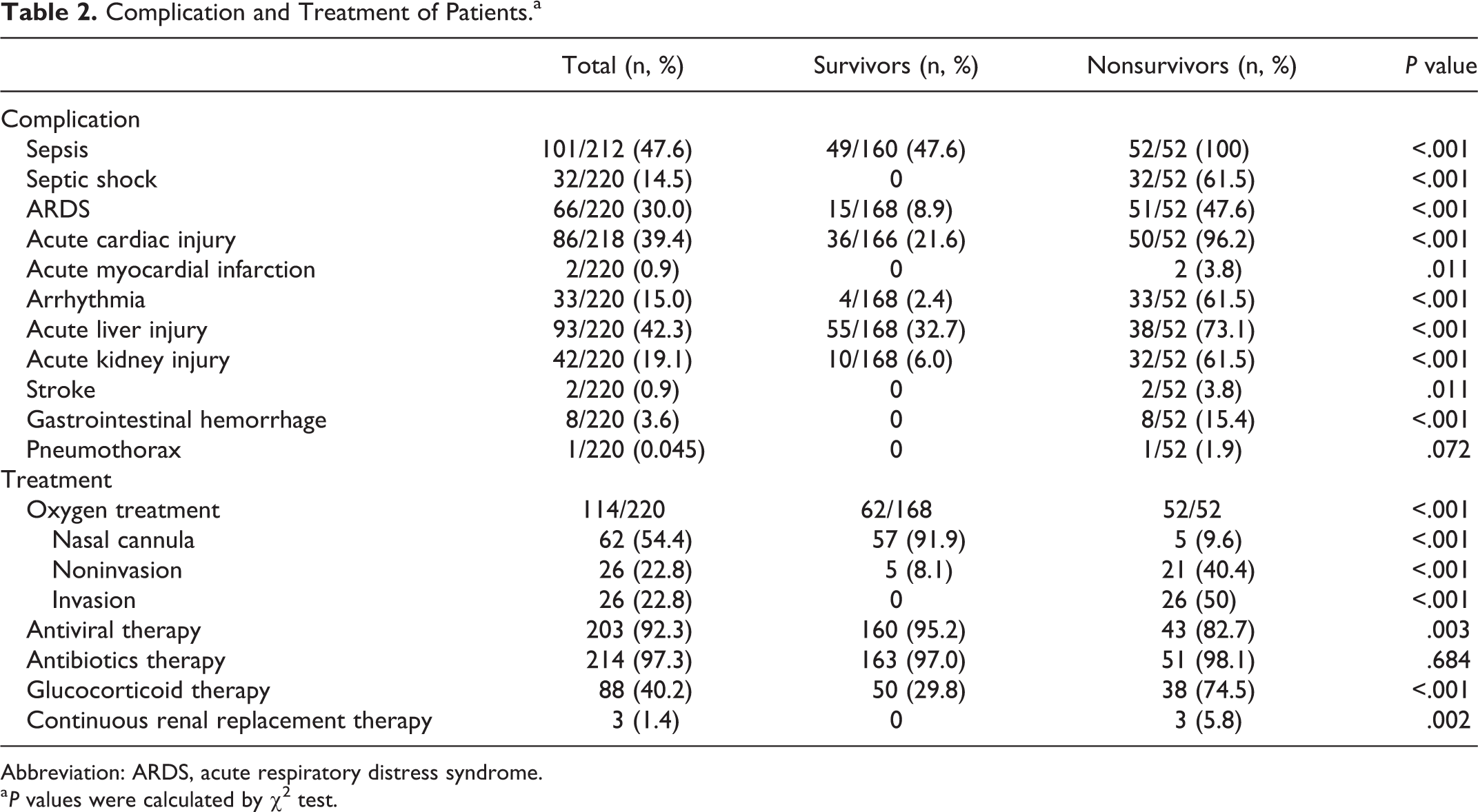
Abbreviation: ARDS, acute respiratory distress syndrome.
a P values were calculated by χ2 test.
Twenty-six patients underwent noninvasive mechanical ventilation, 21 of whom died. None of the survivors required invasion mechanical ventilation and 26 (50%) nonsurvivors received invasive mechanical ventilation. A total of 203 (92.3%) patients received antivirals and 214 (97.3%) received antibiotic therapy. The use of systemic corticosteroid therapy and continuous renal replacement therapy differed significantly between nonsurvivors and survivors (Table 2).
Laboratory Parameters
There were numerous differences in initial laboratory findings between survivors and nonsurvivors (Table 3) on admission, including longer prothrombin time and higher levels of
Laboratory Findings of Patients on Admission.a
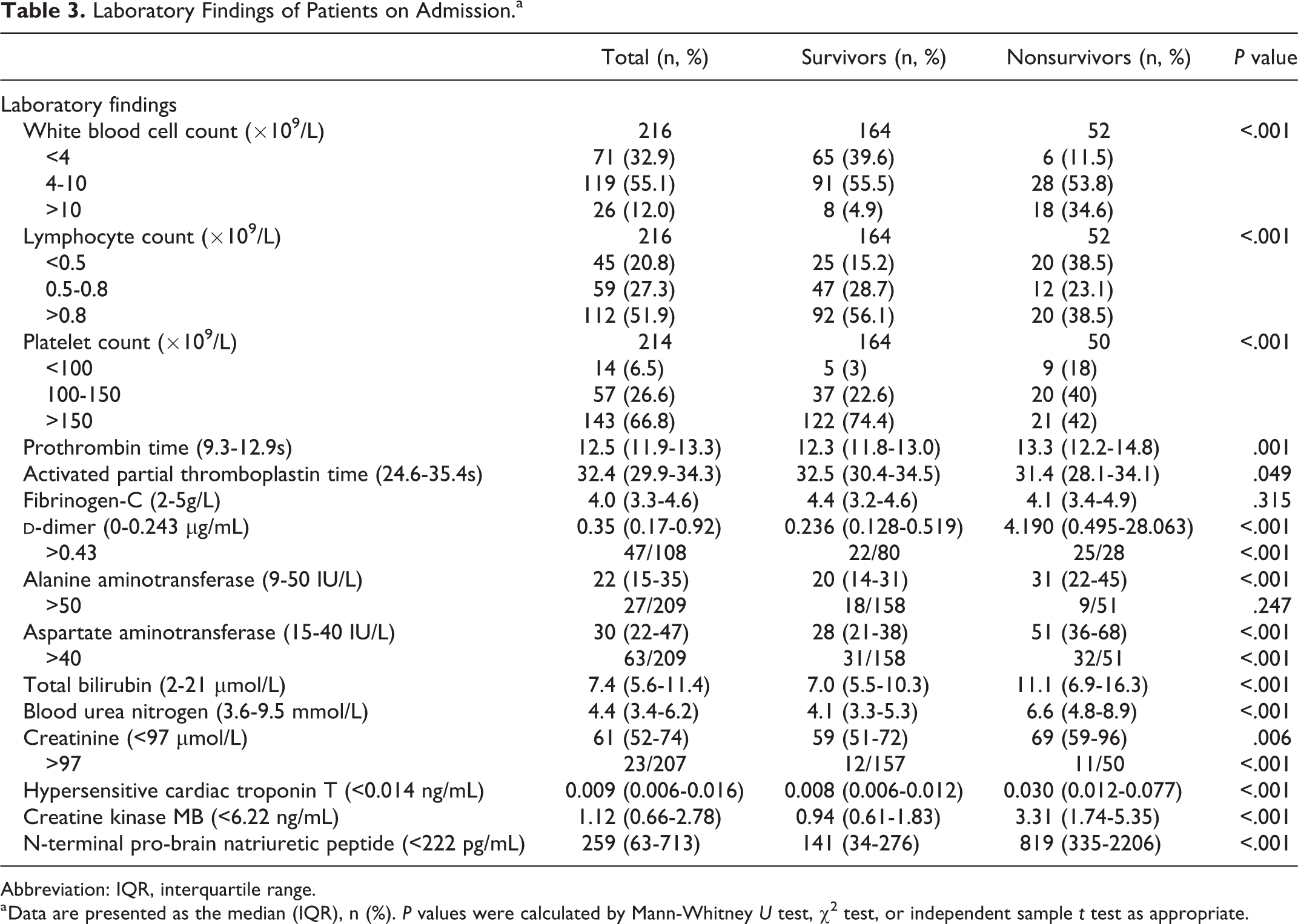
Abbreviation: IQR, interquartile range.
a Data are presented as the median (IQR), n (%). P values were calculated by Mann-Whitney U test, χ2 test, or independent sample t test as appropriate.
Arterial Blood Gas Analysis of Patients on Admission.a
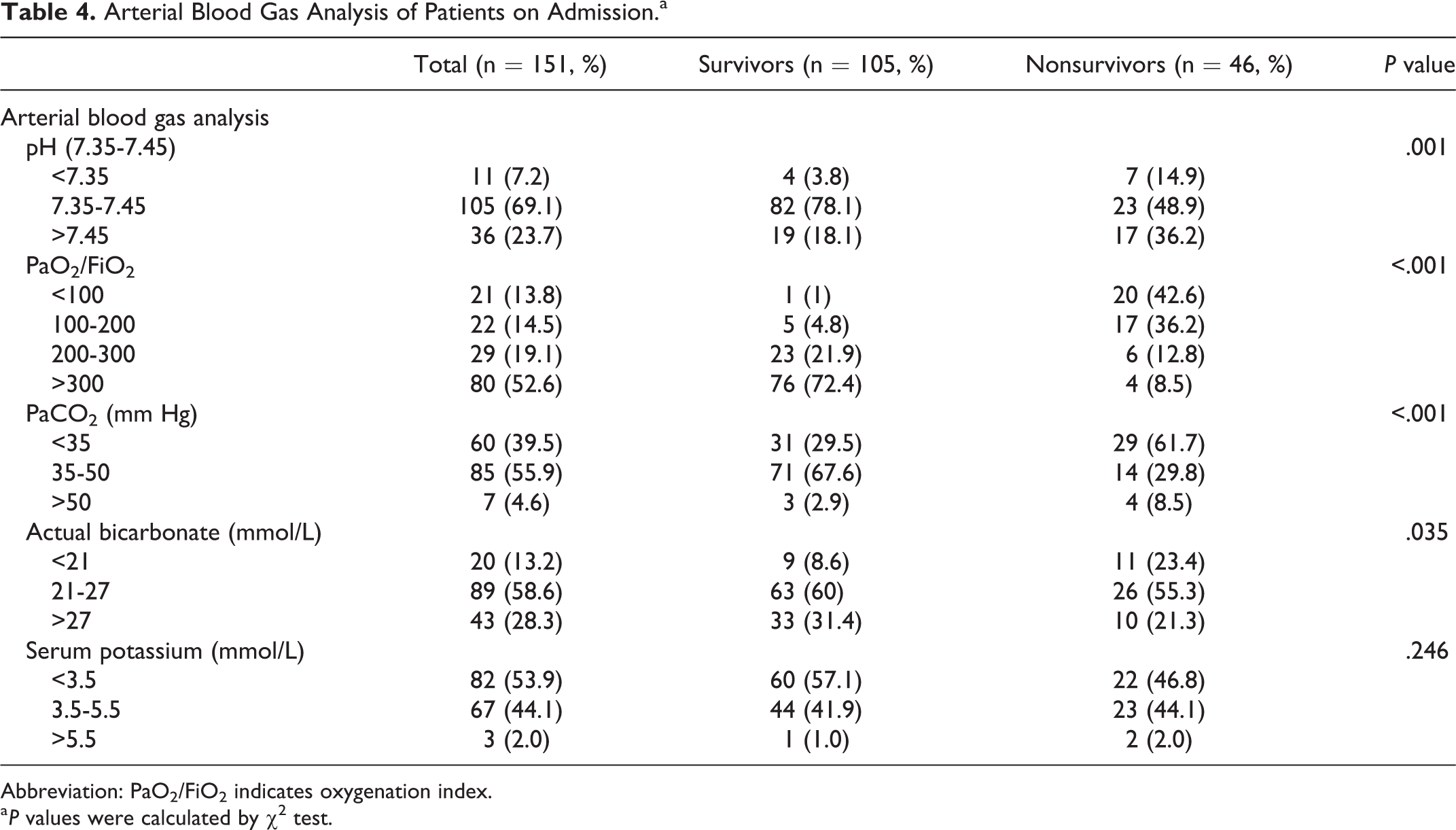
Abbreviation: PaO2/FiO2 indicates oxygenation index.
a P values were calculated by χ2 test.
Dynamic Changes in Laboratory Findings
Dynamic changes in clinical and laboratory parameters were tracked from day 1 to day 21 after admission (Figure 1). During hospitalization, nonsurvivors had higher white blood cell counts and levels of
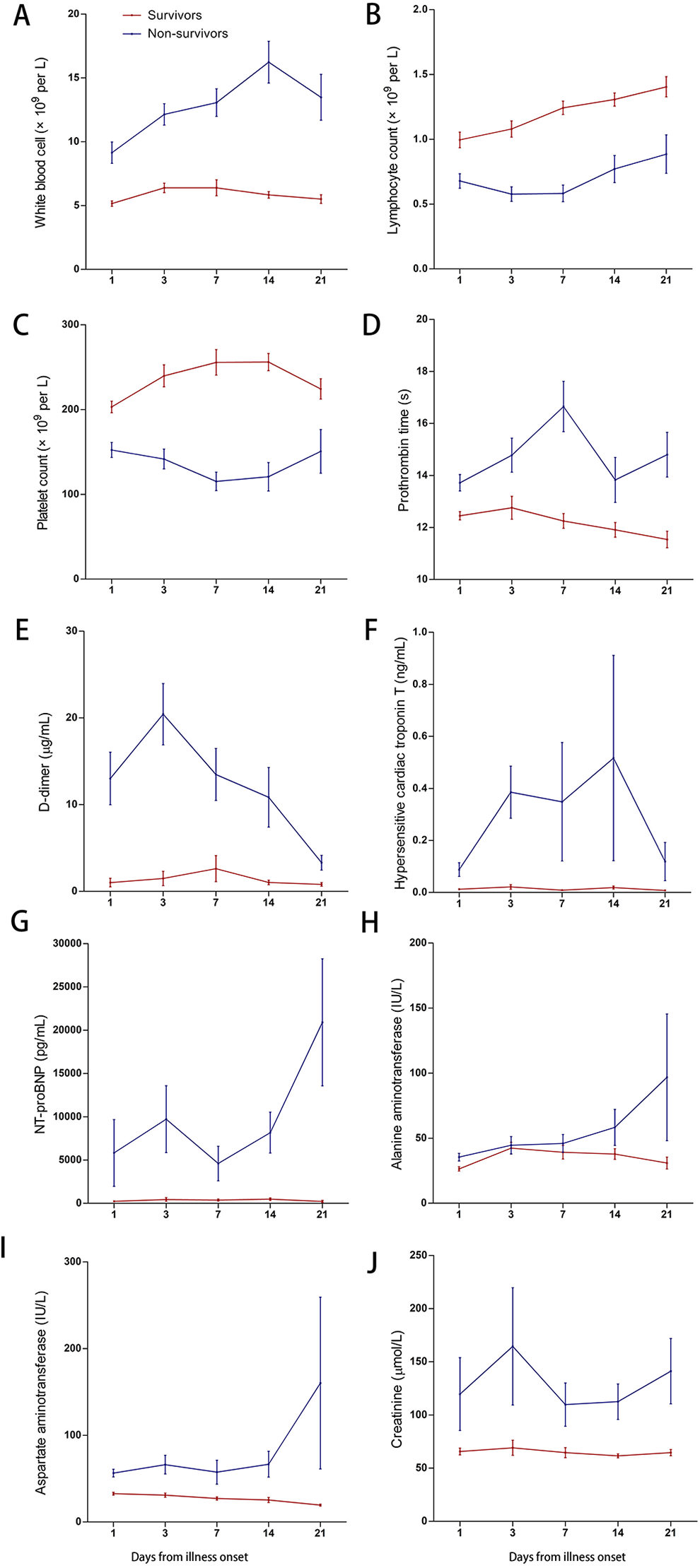
Dynamic changes in laboratory findings. Figure shows temporal changes in the white blood cell count (A), lymphocyte count (B), platelet count (C), prothrombin time (D), and levels of
Risk Factors for Mortality
Age, sex, comorbidity status, initial SOFA score, respiratory rate on admission, and baseline laboratory examinations including lymphocyte count, platelet count, and levels of
Risk Factors for Mortality by Univariable and Multivariable Logistic Regression Associated With in-Hospital Death.
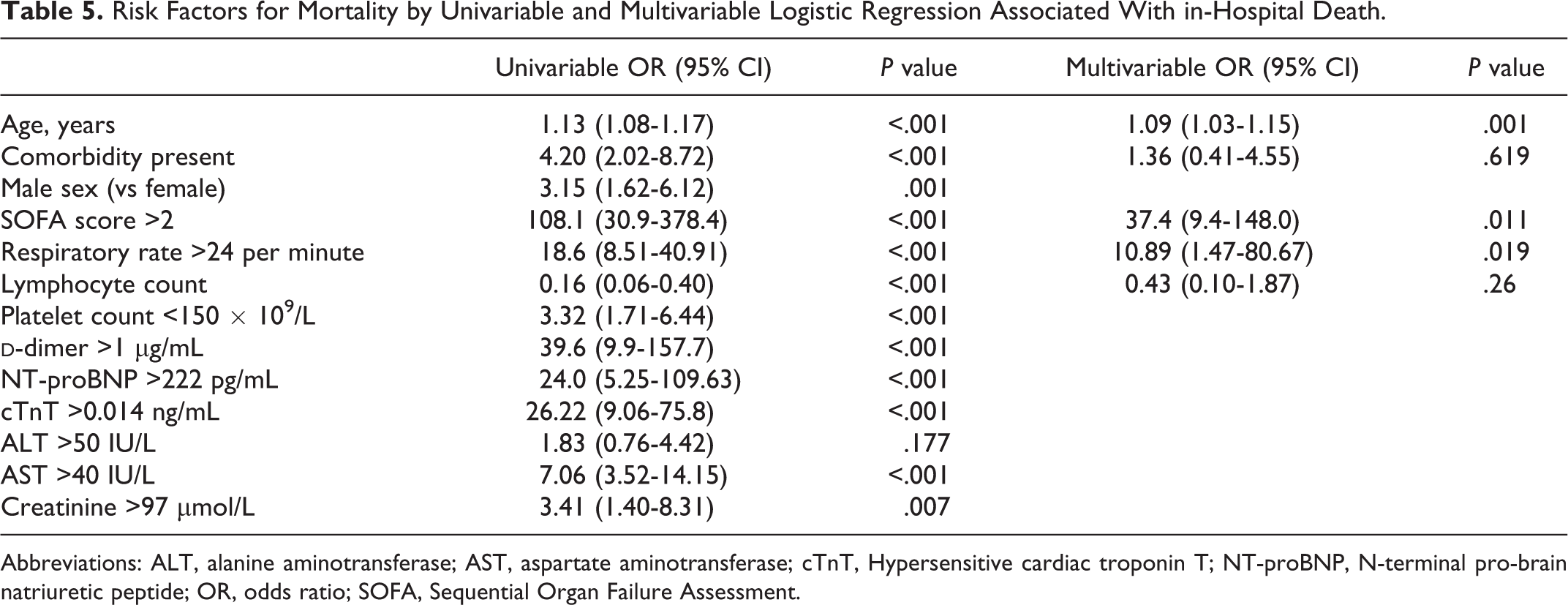
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; cTnT, Hypersensitive cardiac troponin T; NT-proBNP, N-terminal pro-brain natriuretic peptide; OR, odds ratio; SOFA, Sequential Organ Failure Assessment.
Discussion
We describe a cohort of 220 adult patients who were hospitalized with COVID-19 in Wuhan No. 7 Hospital, which is one of the designated hospitals for COVID-19. This study aimed to determine the risk factors for mortality in COVID-19 patients. Older age, SOFA score >2 and respiratory rate >24 per minute on admission were associated with a higher rate of mortality. Compared with surviving patients, nonsurviving patients had lower lymphocyte and platelet counts. Nonsurvivors also had greater increases in
Advanced age has been reported as a predictor of mortality in patients with SARS, Middle East respiratory syndrome (MERS), and COVID-19. 3 -5,12 -14 The SOFA score is a well-known and simple scoring system that is a valid tool used to predict sepsis in critical care units. A SOFA score of 2 or more indicates organ dysfunction in the clinical setting. 8 Previously, the initial SOFA score was identified as a good indicator of prognosis. 15 Although bacterial infection is commonly the cause of sepsis, viral infections also induce direct tissue or cell damage (eg, pulmonary epithelial damage) which leads to viral sepsis. 16 Based on the pathological examinations of patients with COVID-19, researchers found diffuse alveolar damage with cellular fibromyxoid exudates and evident desquamation of pneumocytes and hyaline membrane formation in lung samples of patients with ARDS. 17 In our study, sepsis was observed in all deceased patients, and 47.6% of survivors. Sepsis was the most common complication in all patients especially in nonsurviving patients (100%). In particular, among nonsurvivors, 61.5% experienced septic shock and 98.1% experienced ARDS. We concluded that sepsis (including hypoxemia and organ dysfunction) caused by SARS-CoV-2 infection was the main cause of death.
The respiratory rate is a valid and important tool for assessing the severity of acute respiratory disease and has already been included in prognostic tools (such as the CRB 65 index: confusion, respiratory, blood pressure, age >65 years). The respiratory rate on admission is an independent risk factor for in-hospital mortality associated with community acquired pneumonia and other conditions. 18 In particular, respiratory rate is one of the evaluation indicators for the clinical classification and decision to perform endotracheal intubation in patients with COVID-19. 7,19 In our study, we found that a respiratory rate above 24 per minute was correlated with poor prognosis in patients with COVID-19. The measurement of respiratory rate on admission in patients with COVID-19 should be routinely performed in the clinical setting.
There is currently no effective antiviral therapy for COVID-19. However, the duration of viral shedding may supply some information to guide clinicians in determining the duration of antiviral therapy. 3 In this study, there was no significant difference in the duration of viral shedding between survivors and nonsurvivors. Surprisingly, SARS-CoV-2 RNA was detected in respiratory specimens until death in 30 (77%) of 39 nonsurvivors who were confirmed to have COVID-19. The median time from symptom onset to viral shedding in this study was 21 days. We found that nucleic acids tests were negative 2 consecutive times and then positive again (Figure 2). We should not relax our vigilance as a result of negative nucleic acid results. It is necessary to also consider the improvement in clinical symptoms to assess the change in a patient’s condition. We hope this finding can serve as a reference for the duration of home or hospital isolation and may supply information useful for epidemic control.
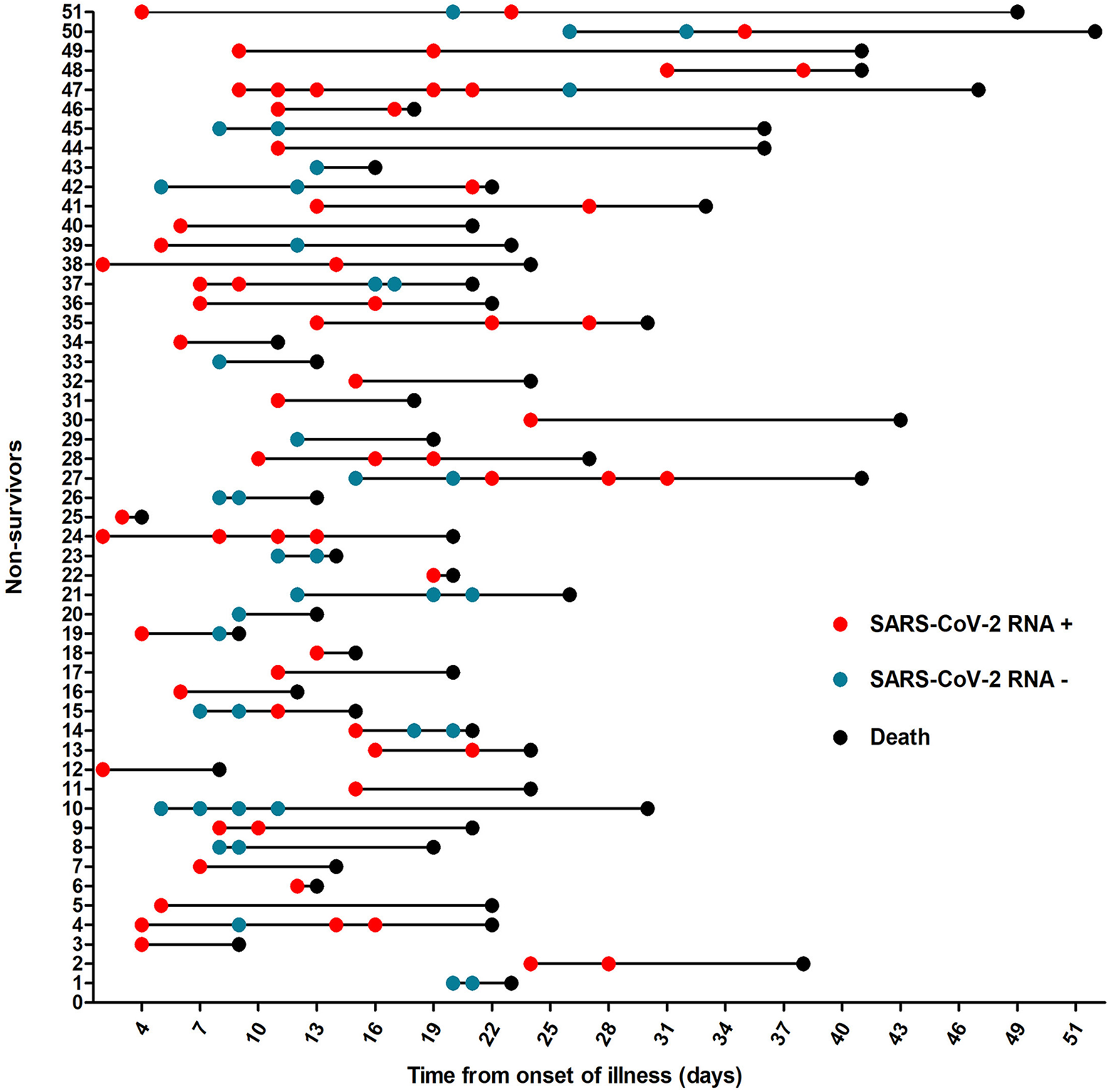
Time course of SARS-CoV-2 RNA results. Figure shows the time course of SARS-CoV-2 RNA results in 51 patients who died. The red circles indicate a positive result for SARS-CoV-2 RNA; green indicates a negative result; and black indicates death. SARS-CoV-2 indicates severe acute respiratory syndrome coronavirus 2.
Recent studies have described cardiovascular complications of COVID-19, including cardiac injury and heart failure. 1,2,4 Although the mechanism underlying cardiac injury caused by SARS-CoV-2 is not clear, it has strong similarities in pathological features with SARS-CoV and MERS. 20 The autopsies of patients who died from SARS revealed that systemic vasculitis included edema, localized fibrinoid necrosis, and the infiltration of monocytes, lymphocytes, and plasma cells into vessel walls in the heart, lung, liver, kidney, adrenal gland, and stroma of striated muscles. 20 -22 Researchers observed that SARS-CoV was also identified in some cardiomyocytes by electron microscopy combined with in situ hybridization. 21,22 An autopsy of a patient with COVID-19 demonstrated that there was no substantial damage to the heart tissue, but the presence of a few interstitial mononuclear inflammatory infiltrates suggested that SARS-CoV-2 infection might not directly lead to myocardial damage. 22 It has been reported that the levels of many cytokines, such as IL-6 and IL-10, are significantly increased in patients with COVID-19. 1,3,4 We speculated that the systemic inflammatory response induced by viral infection led to systemic vessel injury and vasculitis, which caused microcirculation disorder of the heart and acute myocardial injury. Further research is needed to investigate the pathogenesis of COVID-19.
Our study has several limitations. First, this is a single-center retrospective study. Our patients may not represent the entire population. Second, since this is a retrospective study, the study sample size was limited, and our data are incomplete for all laboratory indicators at all points in time. The validation of the predictive ability of these indicators in the regression analysis may have been weakened. Third, limited by early SARS-CoV-2 RNA detection conditions and technology, some patients had no SARS-CoV-2 RNA results or may have presented with false-negative results. The calculation of the duration of viral shedding may have been affected. However, all discharged patients and patients who died at this designated COVID-19 hospital were included in our study. The potential risk factors for mortality included older age, baseline SOFA score >2 and respiratory rate >24 per minute, which could help us to identify patients with a poor prognosis at an early stage. We believe our study is meaningful with regard to advancing our understanding of this disease.
Footnotes
Authors’ Note
S.Z., S.M. and S.L. contributed equally to this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Zhongnan Hospital of Wuhan University Science, Technology, and Innovation Seed Fund (znpy2018021) and the research fund from the medical Sci-Tech innovation platform of Zhongnan Hospital, Wuhan University (PTXM2020027).