
Abstract
Significance Statement
Extranasopharyngeal angiofibromas (ENA) are rare vascular tumors that do not conform to the clinical characteristics of typical nasopharyngeal angiofibromas. We present the management of an angiofibroma in a rare site, within the frontal sinus with a concomitant orbital pyocele, which was completely excised via an endoscopic approach. ENAs should be considered as a differential diagnosis in patients with sinonasal mass and epistaxis. Awareness of this rare entity will avoid radical surgery thus decreasing postoperative morbidity.
A 22-year-old man presented with headache for one month and right-sided eye swelling and double vision for 4 days. Nasal endoscopy showed a smooth polypoidal lesion within the right middle meatus. Ophthalmological examination showed right nonaxial proptosis with a cystic swelling below the eyebrow causing restricted elevation. Vision and fundus examination were normal.
Computerized tomography scan of the paranasal sinus (CT PNS) with contrast showed heterogeneous opacification along with an enhancing mass filling the right frontal and ethmoid sinuses and dehiscence in the lamina papyracea, roof and floor of the frontal sinus. A 34 × 32 × 16 mm fluid collection was noted in the superolateral aspect of extraconal space with inferomedial displacement of the globe (Figure 1A).
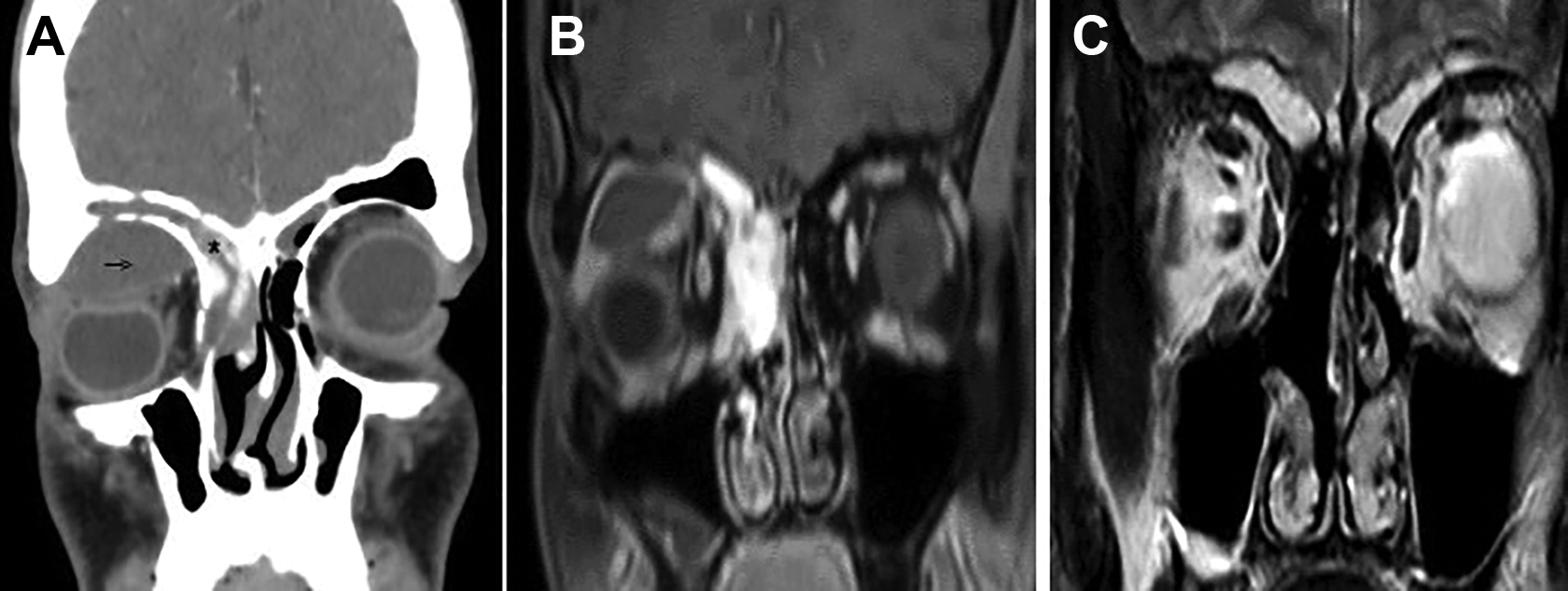
A, Computed tomography (CT) of the paranasal sinus with contrast showing a heterogeneous mass filling the right frontal (asterisk) and ethmoid sinuses with erosion in orbital roof and collection of fluid in the superolateral extraconal space of the orbit (arrow). B, Magnetic resonance imaging (MRI) of the paranasal sinus with contrast showing an enhancing mass in the right frontal and ethmoid sinus with an associated pyocele in the right superolateral extraconal orbital space. C, Postoperative MRI scan showing no evidence of recurrence.
Contrast-enhanced magnetic resonance imaging (MRI) scan showed an ill-defined lobulated intensely enhancing mass in the right frontal and ethmoid sinuses. A separate collection, hypointense on T1-weighted images with peripheral enhancement, was seen in the superior and superolateral extraconal space of the right orbit, indenting and displacing the globe inferiorly (Figure 1B). Digital subtraction angiography done, considering the intense vascularity, showed major supply from the ophthalmic branch of internal carotid artery (Figure 2) which was not embolized.
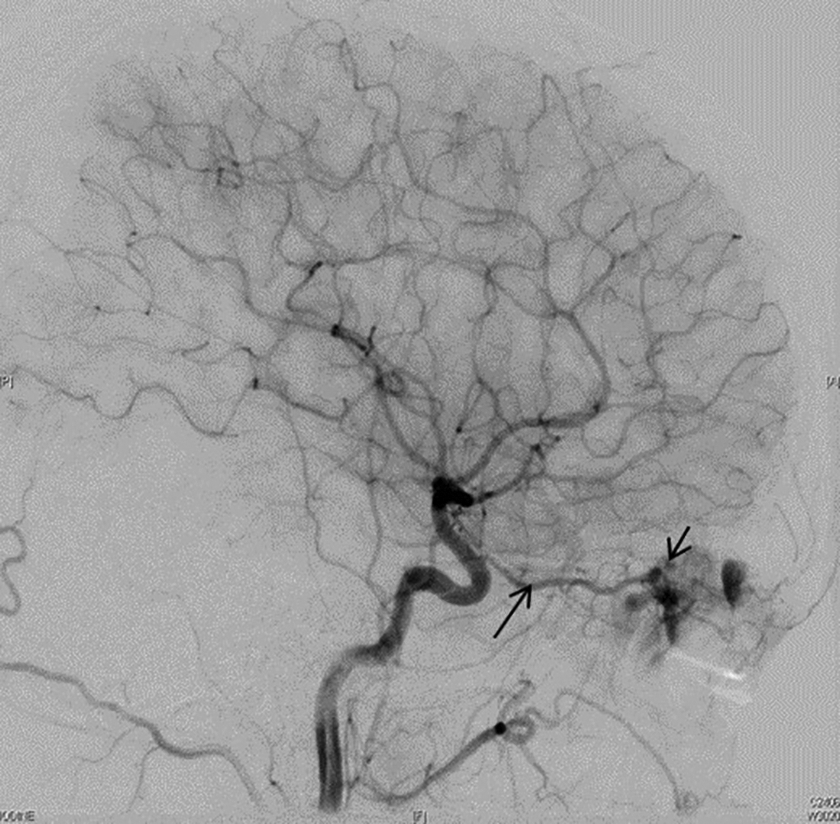
Digital subtraction angiography showing tumor blush (short arrow) with major supply from the ophthalmic artery (long arrow).
An endoscopic approach was employed for tumor excision. Intraoperatively, a firm, well-defined, vascular mass was seen involving the ethmoid and frontal sinuses with bony infiltration in the frontal sinus, which was drilled. The orbital pyocele was completely excised through a Lynch Howarth incision as access was not adequate endoscopically.
Histopathology was diagnostic of angiofibroma (Figure 3). At 2-year follow-up, patient was asymptomatic and repeat MRI scan (Figure 1C) showed no evidence of recurrence.
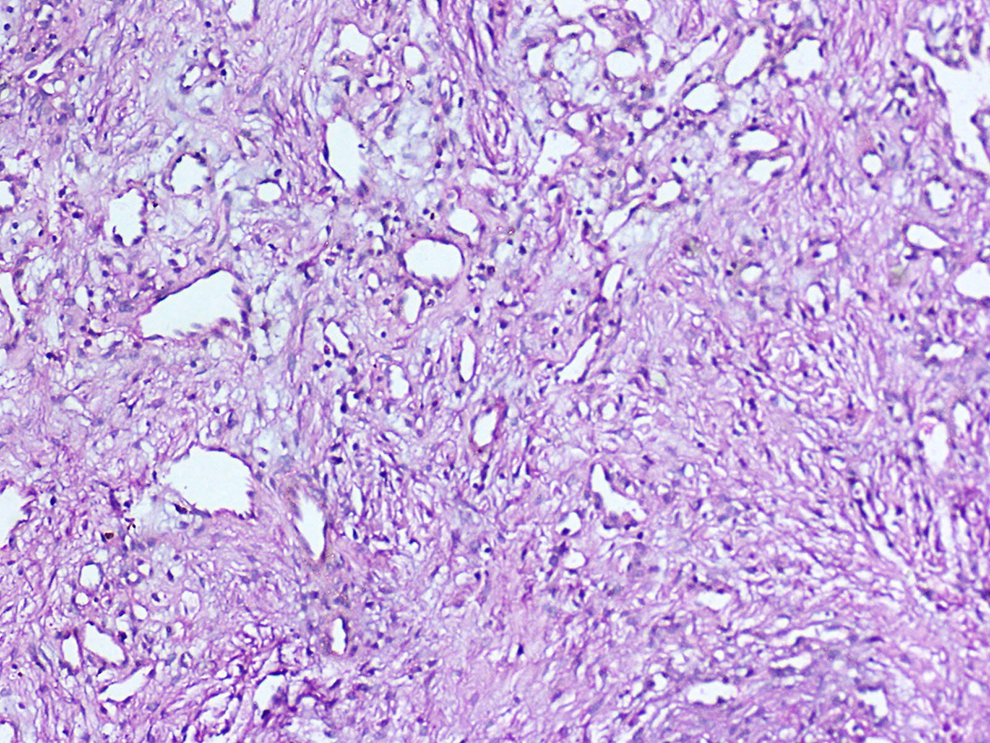
Photomicrograph showing angiofibroma with stellate and staghorn blood vessels lined by single layer of endothelial cells within the fibrous stroma (H&E × 100).
Extranasopharyngeal angiofibromas (ENA) are benign angiofibromas originating from areas other than the sphenopalatine foramen. The etiology of ENA is still unclear, although several theories exist. Migration of the fascia basalis seen in the anteroinferior sphenoid wall and atlas to distant extranasopharyngeal sites like the periosteum of the perpendicular plate of ethmoid bone during embryogenesis is a popular theory. 1 Unequal development of the skull bones is another suggested cause. In one series, the maxillary sinus was found to be the most common site of origin, 2 although Windfuhr and Vent 3 reported a higher percentage of septal involvement in his series. Involvement of other extranasopharyngeal sites such as middle and inferior turbinates,4,5 ethmoid sinus, 6 frontal sinus, 7 and base of skull 8 have also been reported. To the best of our knowledge, our patient is the only reported case of ENA arising from the frontal sinus with an associated pyocele.
Compared to juvenile nasopharyngeal angiofibromas (JNA), ENAs are seen in older age-group with a mean age of 28 years and a male to female ratio of 3:1. 3 Rare occurrence in young children 9 and infants 10 have been reported. Mild to moderate epistaxis along with nasal obstruction, headache, and facial swelling are common presenting symptoms, depending on the site of involvement. Our patient also had proptosis secondary to a coexisting pyocele which developed due to frontal sinus outflow tract occlusion by the tumor. A relatively short history of a few months in ENA could be due to early detection because of involvement of anterior sinonasal sites compared to 1 to 2 years in JNA which occurs more posteriorly. 11
Extranasopharyngeal angiofibromas present as smooth-surfaced, firm, fleshy masses which are pink and intensely vascular in appearance. Computerized tomography scan of the paranasal sinus with contrast is the imaging of choice. Magnetic resonance imaging is essential if there is suspicion of intracranial, intraorbital, or soft tissue involvement. Most reports on ENA do not mention the use of preoperative angiography to assess the vascular supply of the tumor or perform embolization as is often described for JNA. In our patient, because of the intensely enhancing mass seen on contrast MRI scanning, we performed preoperative angiography which showed a tumor blush from the right ophthalmic branch of ICA. This, however, was not embolized in view of the risk of blindness.
Complete surgical resection forms the mainstay of treatment for ENAs. The surgical approach depends on tumor extent with most cases amenable to endoscopic excision. Since our patient had an associated frontal pyocele, an additional Lynch Howarth incision was required. Intraosseous extension into the adjacent bones requires meticulous drilling to avoid microscopic remnants. Unlike JNA, ENA shows a low recurrence rate of 2.3%. 3
Differential diagnosis for a vascular frontoethmoid mass in an adult could include tumors such as hemangiopericytoma, hemangioma, and angiosarcoma and ENA is a rare possibility. 12 Awareness of this rare entity will help in better preoperative assessment ensuring complete surgical excision.
Footnotes
Authors’ Note
R.K., R.M., L.V. contributed to concepts; R.K., R.M., L.V., R.B.T., M.T., V.R. contributed to literature search, data analysis, manuscript editing, and manuscript review; R.K., R.M., L.V., R.B.T., M.T. contributed to data acquisition; R.K., R.M., L.V. contributed to manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.