
Abstract
We describe the case of a 51-year-old woman with immunoglobulin G4-related disease (IgG4-RD) diagnosed using lip biopsy. She reported having bilateral submandibular nodules for a month. Magnetic resonance imaging showed diffuse swelling in the bilateral submandibular glands (SMGs), suggesting inflammatory changes. Laboratory data revealed an elevated level of serum IgG4. Fine needle aspiration cytology of the SMG showed a considerable number of lymphocytes with degeneration but did not demonstrate specific findings for a definitive diagnosis of IgG4-RD. Lip biopsy was performed, and a biopsy specimen from the labial salivary gland showed abundant lymphoplasmacytic infiltration with a large number of IgG4-positive cells. The patient was diagnosed with IgG4-RD based on histological and laboratory findings. Findings of further examinations revealed that the patient had autoimmune pancreatitis, confirming our diagnosis. Four months after prednisolone administration, improvement of the submandibular and pancreatic lesions was observed. One year after the initial presentation, the serum IgG4 level was normalized. In cases of IgG4-RD with salivary gland involvement, lip biopsy might be one of the options for the histological diagnosis of IgG4-RD.
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is a novel clinical disease characterized by elevated serum IgG4 levels and tumefaction or tissue infiltration by IgG4-positive cells. The condition may occur in some patients with a wide variety of diseases, including Mikulicz disease, autoimmune pancreatitis, hypophysitis, Riedel thyroiditis, interstitial pneumonitis, interstitial nephritis, prostatitis, lymphadenopathy, retroperitoneal fibrosis, inflammatory aortic aneurysm, and inflammatory pseudotumor. 1 Chronic sclerosing sialadenitis, known as Küttner tumor, is characterized by a marked infiltration of IgG4-positive cells and a high IgG4/IgG-positive cell ratio (>40%). Contrastingly, sialolithiasis and Sjögren syndrome show a variable number of IgG4-positive cell infiltrates and a low IgG4/IgG-positive cell ratio (<5%). 2 The most important difference between IgG4-RD and Sjögren syndrome is that the former is characterized by a marked infiltration of IgG4-positive cells with a ratio of IgG4-positive to IgG-positive cells of >40%, a finding almost never seen in patients with Sjögren syndrome. 1
Although the diagnostic criteria for IgG4-RD of each organ and the comprehensive diagnostic criteria for IgG4-RD have been developed, one of the biggest challenges in the field is distinguishing between IgG4-RD and mimickers because some non-IgG4-RDs may meet the diagnostic criteria for IgG4-RD and can be misdiagnosed as IgG4-RD. 3 Histological examination is essential for the definitive diagnosis of IgG4-RD, as other pathological conditions can also present with serum IgG4 elevation. 4 The diagnosis of IgG4-RD relies on the combined presence of the characteristic histopathological findings and the increased number of IgG4-positive cells. The tissue IgG4 counts and the IgG4:IgG ratios are of secondary importance. 5 In cases of IgG4-RD presenting with swelling of the submandibular gland (SMG), SMG biopsy is useful and appropriate for a definitive diagnosis of IgG4-RD.4,6 On the other hand, lip biopsy is generally performed for the histological diagnosis of Sjögren syndrome. However, considering postoperative complications or from an esthetic perspective, it is preferable if lip biopsy could be applied for the diagnosis of IgG4-RD in place of SMG biopsy. There have been only a few reports to date in which the histological diagnosis of IgG4-RD has been established with lip biopsy.4,6-12 Herein, we describe a case of IgG4-RD diagnosed histologically using lip biopsy.
Case Report
A 51-year-old Japanese woman presented to our hospital with complaints of SMG swelling for a month. The patient had a history of bronchial asthma and no history of recurrent sialadenitis or sialolithiasis. She did not suffer from xerostomia (dry eyes). Although the bilateral SMGs were swollen with no tenderness, the labial salivary gland (LSG) in her lower lip appeared normal. On ultrasonography, the bilateral SMGs appeared grossly swollen with diffuse hypoechoic changes. Magnetic resonance imaging (MRI) showed diffuse swelling of the bilateral SMGs, which appeared as hypointense regions on T1-weighted imaging (T1WI) and as hyperintense regions on T2-weighted imaging (T2WI). This suggested nonspecific inflammatory changes rather than tumorous changes (Figure 1A and B). No abnormalities were detected in the other laryngopharyngeal regions. Fine needle aspiration cytology of the right SMG showed a considerable number of lymphocytes with degeneration but did not demonstrate specific findings for a definitive diagnosis.
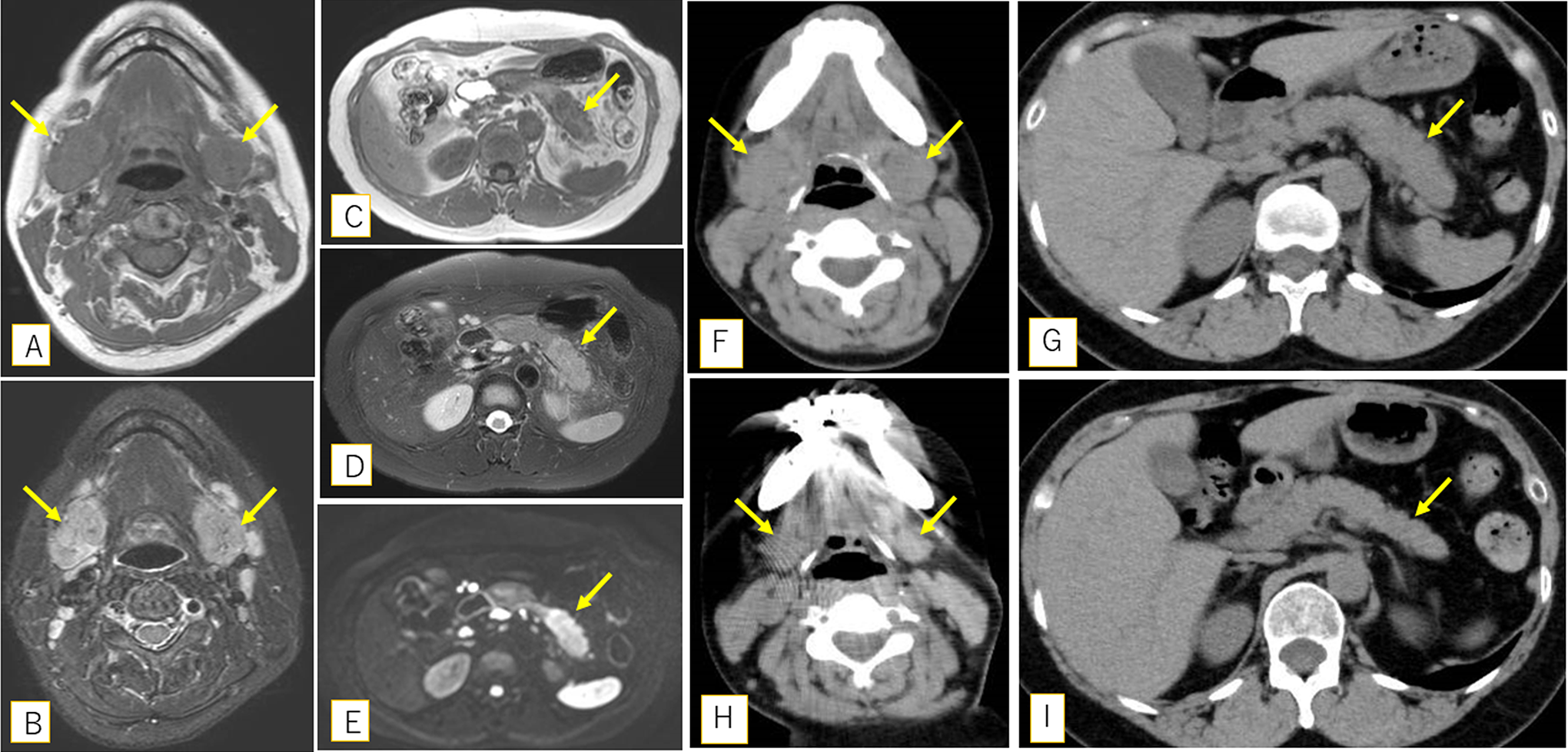
Magnetic resonance imaging (MRI) shows diffuse swelling of the bilateral submandibular glands (arrows) as hypointense regions on T1-weighted imaging (A) and hyperintense regions on T2-weighted imaging (B). Magnetic resonance imaging shows the enlargement of the pancreas tail (arrows) as a hypointense region on T1-weighted imaging (C) and a hyperintense region both on T2-weighted imaging (D) and diffusion-weighted imaging (E). Computed tomography shows remarkable improvement of the swelling of submandibular and pancreatic lesions (F and G) compared to pretreatment (H and I).
Laboratory data revealed elevated levels of serum IgG (2205 mg/dL; normal range: 861-1747 mg/dL), IgG4 (630 mg/dL; normal range: 5-117 mg/dL), soluble interleukin-2 receptor (sIL-2R; 1077 U/mL; normal range: 127-582 U/mL), and amylase (323 U/L; normal range: 44-132 U/L). The white blood cell count was within normal limits (6200/µL; normal range: 3300-8600/μL) and the differential white blood cell count was neutrophils, 55.8% (normal range: 39.8%-70.5%); basophils, 1.0% (normal range: 0.3%-1.4%); eosinophils, 7.8% (normal range: 0.6%-5.4%); lymphocytes, 29.0% (normal range: 23.1%-49.9%); and monocytes, 6.4% (normal range: 4.3%-10%). The patient tested negative for both anti-Sjögren syndrome A and B antibodies.
The patient did not consent to SMG biopsy for fear of surgical risk. Therefore, we performed lip biopsy, which is less invasive, in an attempt to obtain pathological data with patient agreement. The lip biopsy revealed considerable lymphoplasmacytic infiltration with mild fibrosis (Figure 2A and B). The number of IgG4- or IgG-positive cells was immunohistochemically estimated in the areas with the highest density of these cells. Three high-power fields (HPFs; eyepiece, 10×; lens, 40×) were examined, and the average number of IgG4- or IgG-positive cells per HPF was calculated. We found that the plasma cells predominantly expressed IgG4 (>100/HPF), and the IgG4/IgG ratio was >40% (Figure 2C and D). According to the international pathological diagnostic criteria, 5 these pathological findings were consistent with those indicating IgG4-RD. An abdominal MRI showed enlargement of the pancreatic tail as a hypointense region on T1WI and a hyperintense region both on T2WI and diffusion-weighted imaging (Figure 1C-E). Histological findings revealed that the patient had autoimmune pancreatitis. Referencing the exclusion criteria for IgG4-RD proposed by the Research Program for Intractable Disease of the Ministry of Health, Labor, and Welfare of Japan, all Japanese IgG4 team, 5 we checked the serum levels of C-reactive protein (normal range: 0-0.14 mg/dL), IgA (normal range: 93-393 mg/dL), and IgM (normal range: 50-269 mg/dL), which were 0.03 mg/dL, 168 mg/dL, and 88 mg/dL, respectively. As these parameters were within the normal range, we reached a definitive diagnosis of IgG4-RD.
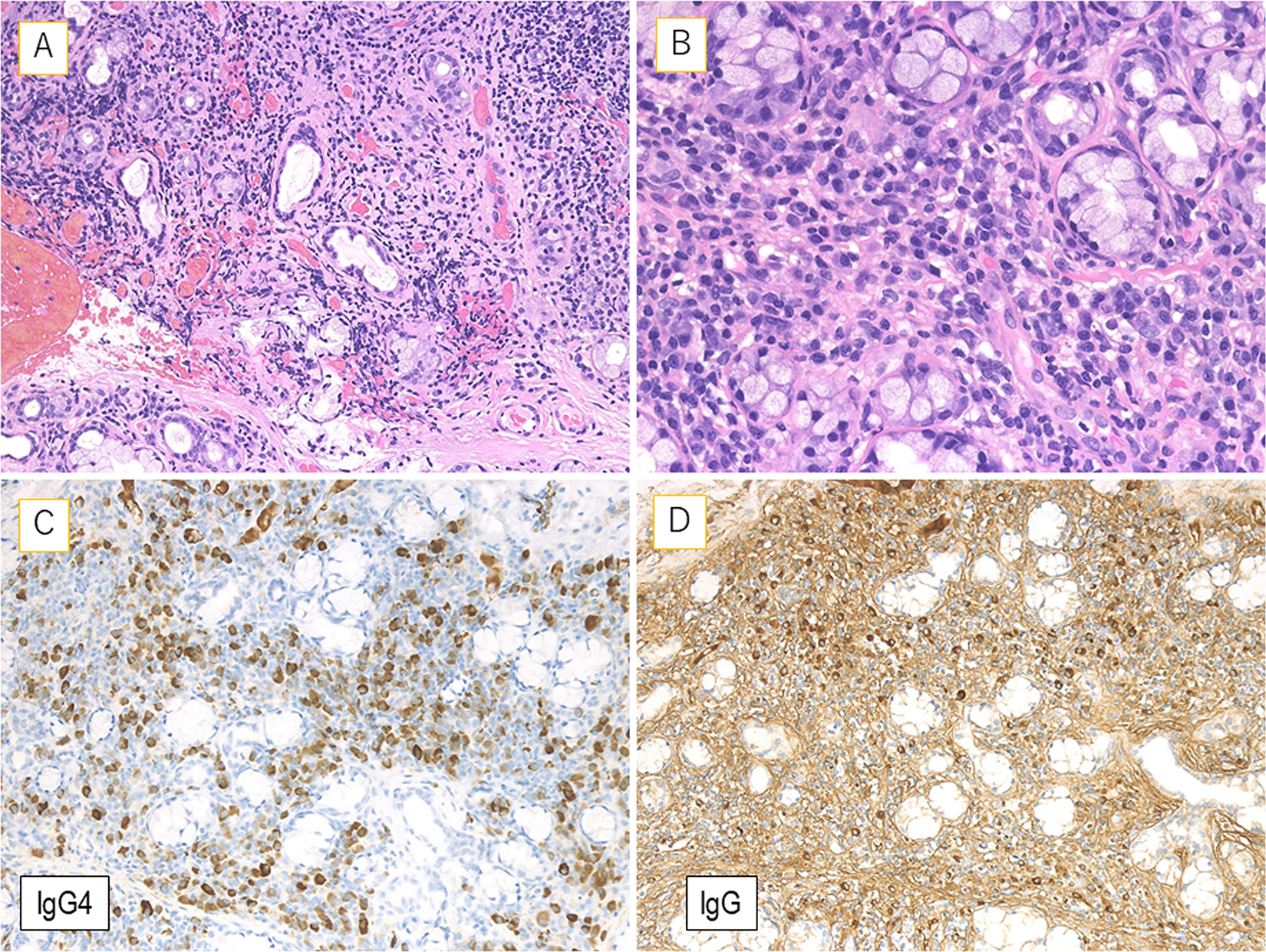
The lip biopsy specimen shows abundant lymphoplasmacytic infiltration with mild fibrosis (A and B). The plasma cells predominantly express immunoglobulin G4 (IgG4; >100/high-power field), and the IgG4/IgG ratio is > 40% (C and D).
Oral prednisolone (30 mg/d) administration was initiated. Four months after prednisolone administration, remarkable improvement in the swelling of the submandibular and pancreatic lesions was observed on CT findings (Figure 1F-I), and the serum level of IgG4 decreased to 422 mg/dL. The level of IgG4 normalized (108 mg/dL) 1 year after the initial presentation. The dose of prednisolone was gradually tapered, and the patient was administered a dose of 5 mg daily without recurrence for 2 years.
Discussion
Immunoglobulin G4-related disease frequently involves vital or internal organs on which biopsies are difficult to perform. 4 Incisional biopsy of the SMG is useful and appropriate for the histological diagnosis of IgG4-RD. However, this invasive procedure often leads to postoperative complications, including paralysis of the marginal mandibular branch of the facial nerve and cosmetic problems.10,11 In the present case, the histological diagnosis of IgG4-RD was established with the observation of IgG4-positive cell infiltration in the minor LSGs. Compared to SMG biopsy, lip biopsy is not only less invasive but can be performed more quickly. Early recognition and diagnosis of this disease are clinically important to prevent irreversible organ damage, which can be avoided through glucocorticoids, to which most patients respond well. 4 The present case was successfully treated with prednisolone.
Previously, in 2 cases of suspected Sjögren syndrome or Mikulicz disease, lip biopsy coincidentally revealed IgG4-positive cell infiltration in the minor LSGs, histologically confirming IgG4-RD.7,8 Histological diagnosis of IgG4-RD was reportedly also established with lip biopsy in a case with minute lumps in the mucosa of the lower lip. 9 However, cases like the present one, where the histological diagnosis of IgG4-RD could be diagnosed from the LSG of a lower lip having a normal appearance, are extremely rare. It has also been reported that LSG tissue can be used for the pathological diagnosis of IgG4-RD, even when physical examination and imaging findings do not suggest LSG involvement. 4
Patient eligibility to undergo lip biopsy can be controversial, since detectable abnormality through physical examination or imaging of LSGs is rare. 12 Although there have been several studies on lip biopsy for the histological diagnosis of IgG4-RD,6,10-12 most of them included fewer than 20 cases. The sensitivity of LSG biopsy for the diagnosis of IgG4-RD is reportedly low (55.6%-69.2%).6,10,11 A previous study showed that a LSG biopsy can diagnose IgG4-RD in patients whose involved organs are difficult to perform a biopsy. 10 It has also been reported that LSG biopsy helps diagnose IgG4-RD in patients with a high serum IgG4 level and multiple organ involvement, especially in those with salivary gland lesions. 6 In addition, the sIL-2R level may help predict the presence of infiltrating IgG4-positive plasma cells in the LSG. 11 The present case also showed high serum levels of IgG4 and sIL-2R and multiple organ involvement. Recently, Akiyama et al 12 suggested that circulating T follicular helper 2 cells and plasmablasts reflect IgG4-positive cell infiltration in the LSGs, and that this finding could be a predictive marker for patient selection and positive pathological findings on lip biopsy in IgG4-RD. The present case involved a history of bronchial asthma. Patients having IgG4-RD with SGM lesions are reported to have a higher incidence of allergic diseases, such as bronchial asthma, atopic dermatitis, and allergic rhinitis, compared with those having IgG4-RD without salivary gland lesions. 6 In the future, further studies are needed to determine which cases can be diagnosed with the less invasive lip biopsy.
This report has some limitations. The critical histopathological features of IgG4-RD are a dense lymphoplasmacytic infiltrate, a storiform pattern of fibrosis, and obliterative phlebitis. 5 In the present case, although diffuse fibrosis of the glands with lymphoplasmacytic infiltration and IgG4-positive cell infiltration were identified, storiform fibrosis or obstructive phlebitis, which are characteristic histological findings of IgG4-RD, were not evident. This might be explained by the fact that the specimen collected in LSG biopsy is too small compared with that in SMG biopsy. It has been reported that the pathological characteristics of IgG4-positive cell infiltration accompanied by storiform or swirling fibrosis and obliterative phlebitis are inconspicuous or absent in LSG specimens. 11 In addition, biopsy of the enlarged SMG itself was not performed in the present case. A previous study indicated that the reduction in the size of the salivary glands should be confirmed after steroid therapy since malignant disease could not be excluded from the differential diagnosis although malignant cells were not detected in the LSG specimen. 11 Considering this report, we confirmed that the SMG lesions improved on steroid administration. We also followed the patient carefully and found no recurrence for 2 years.
Conclusion
We describe a 51-year-old woman with IgG4-RD, diagnosed histologically using biopsy of the LSG. In cases of IgG4-RD with salivary gland involvement, lip biopsy might be one of the options for the pathological diagnosis of IgG4-RD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.