
Abstract
Objectives:
Many studies on the relationship between gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux (LPR) were based on symptoms, but there are few research on it using reflux monitoring. This study was designed to investigate the relationship between GERD and LPR based on pH monitoring.
Methods:
All patients were scheduled for esophageal manometry and pH monitoring sequentially. They were stratified into 4 groups as no reflux disease, isolated GERD, isolated LPR (iLPR), and GERD combined with LPR (GERD&LPR) according to pH monitoring.
Results:
The incidence of LPR in GERD was 46.3%, while the probability of combining GERD in LPR was 52.7%. The reflux profile in the laryngopharynx showed a significant difference in the total reflux time (17.82 ± 18.4 vs 9.62 ± 9.58, P = .023) and the percentage of total reflux time (1.31% ± 1.37% vs 0.71% ± .0.73%, P = .023) between the GERD&LPR and iLPR groups.
Conclusion:
Laryngopharyngeal reflux can be combined with GERD or it can exist as an independent diagnosis. In patients with GERD&LPR, the total reflux time and the percentage of reflux time in the laryngopharynx are higher than those in the iLPR group. Reflux episodes in the laryngopharynx of patients with GERD&LPR may be derived from GERD.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is pathogenically defined as a series of clinical symptoms such as regurgitation and heartburn, resulting from esophageal mucosal break due to gastroesophageal reflux (GER). 1 It has a high global prevalence with a significant burden in many countries. 2
Laryngopharyngeal reflux (LPR) was conceptualized with the backflow of gastric contents into the laryngopharynx and the upper aerodigestive tract. In the ENT department, an estimated 4% to 10% of patients with LPR may be pathogenically associated with other coexisting diseases, such as chronic pharyngitis, laryngitis, carcinoma, asthma, sleep apnea syndrome, and so on. This can significantly impact the quality of life. 3
Many studies on the relationship between them evidenced that the prevalence of LPR is high in patients with GERD based on symptoms. 4,5 Our previous investigation found that GERD combined with LPR (GERD&LPR) was 47.9% in patients with GERD, while LPR combined with GERD was 71% in patients with LPR. Thus, LPR may occur more commonly with GERD. 6 But there are few research on their relationship using reflux monitoring. Therefore, we designed this study by using pH monitoring to investigate the relationship between LPR and GERD with more objective measurement, which enabled this distinction.
Patients and Methods
Patient Recruitment
Patients who went to the Gastrointestinal Motility Department of our hospital were recruited for this prospective study; participation was voluntary. All the patients provided informed consent. They were recruited only after fulfilling the inclusion and exclusion criteria.
The inclusion criteria were: (1) complain of at least 1 symptom noted in reflux symptom index (RSI) or reflux disease questionnaire, (2) age group of 18 to 70 years, (3) proton pump inhibitor, and histamine 2 receptor (H2R) not taken within 1 month of the beginning of this study, and (4) normal communicative and cognitive capacities.
The exclusion criteria were: (1) subjective inability to collaborate such as patients with mental illness or those presenting with loss of consciousness; (2) patients having severe conditions and cannot tolerate esophageal manometry or reflux monitoring such as acute coronary syndrome and so on; (3) endoscopy results reveal either peptic ulcer or upper gastrointestinal tumor, or other diseases affecting the outcome; and (4) conditions against inclusion criteria.
All patients signed the written informed consent at the hospital. The Ethics Committee of our hospital approved the study.
Esophageal Manometry
The purpose of esophageal manometry is to identify the anatomic positions of the upper esophageal sphincter (UES) and lower esophageal sphincter (LES) as well as to exclude esophageal motility disorders. Medical Measurement Systems was used. The water perfusion manometric system included an electrical pump (Mui Scientific) along with a 6-channel (E6-1-1-5-5-5) esophageal water perfused catheter. Following fasting (≥8 hours) of the patient, the catheter was inserted through the nose to record the position of the upper UES and LES, the changes in the esophageal body and sphincter pressure as a result of the swallowed water were also analyzed. The length from the upper edge of UES and LES to the nostril was routinely recorded, and the distance between them was calculated and was named DBULES.
Ambulatory 24-Hour pH Monitoring
Once esophageal manometry was completed, the patients further underwent ambulatory laryngopharyngeal and esophageal pH monitoring. Digitraper MK III recorder (CTD SYNECTICS Medical) was used. The dual-channel pH monitoring probe (Synetics Medical) contained laryngopharyngeal and distal esophageal sensors. The distance between 2 sensors varies from 15 to 21 cm with 2 cm gradient. The interspacing of probe was decided according to the following formula:
pH probes’ spacing (cm) = DBULES (cm) − 4 (or 3) (cm); when DBULES is even, subtract 3, while when it is odd, subtract 4.
Following this, the electrode was calibrated and inserted into the esophagus with the distal esophageal sensor at a height of 5 cm above the upper edge of LES. After 24 hours, the monitoring was terminated, and polygram for Windows release 2.04 was used to analyze these data.
Laryngopharyngeal reflux is confirmed when the number of reflux (pH < 4.0 in the laryngopharynx) is ≥7, or the reflux area index is ≥6.3. 7 The criterion for GERD is having a DeMeester score of ≥14.72 (see Figure 1). 8
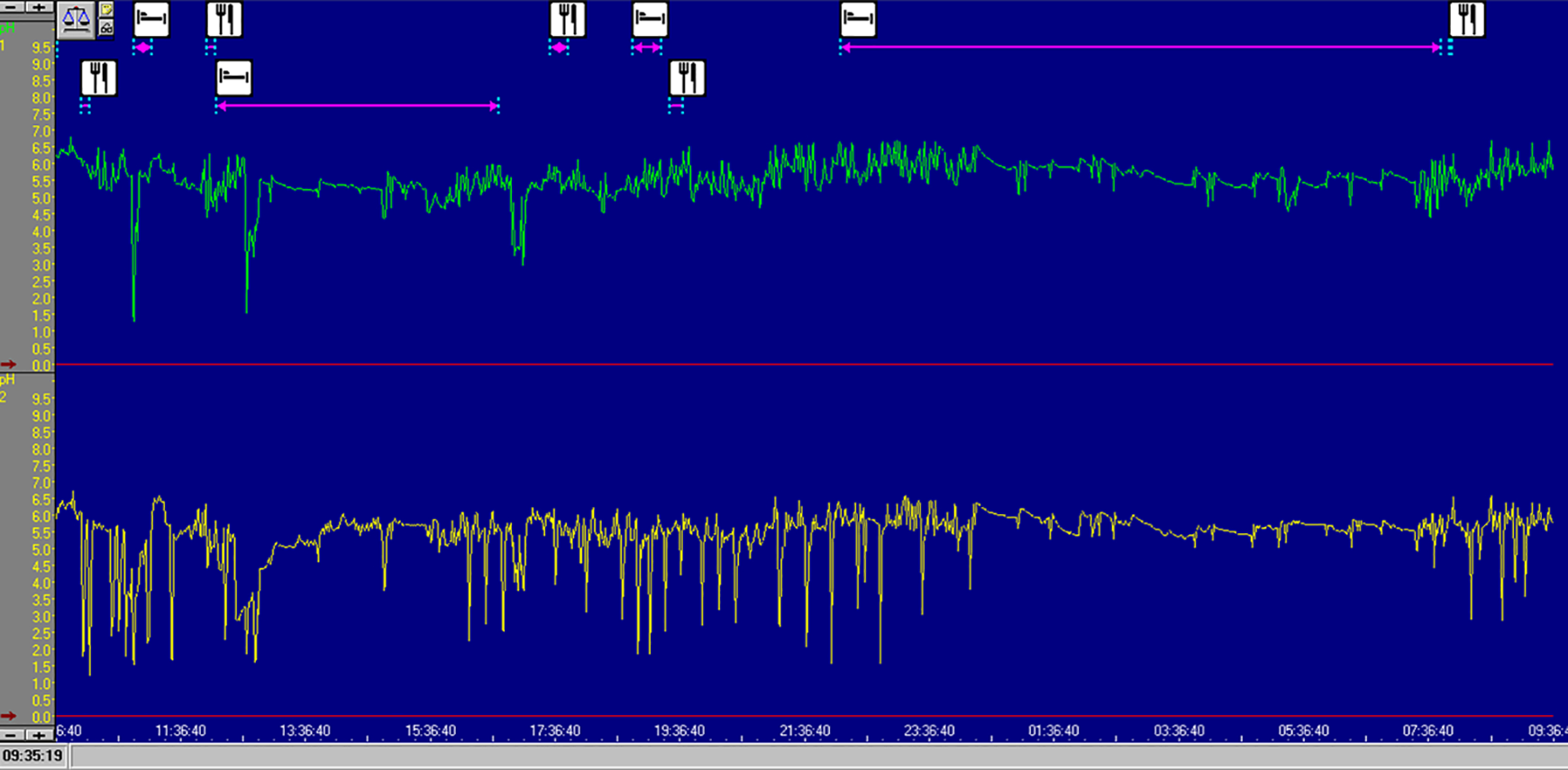
pH monitoring in laryngopharynx and distal esophagus simultaneously. In the upper part of the picture, the green curve represented pH profile in laryngopharynx. It records a total of 13 times of reflux, and its reflux area index is 37.3, which met the diagnostic criteria for laryngopharyngeal reflux. In the lower part, the yellow curve represented pH profile in distal esophagus. The DeMesster score was 13.9, which failed to meet the diagnostic criteria for gastroesophageal reflux disease.
Statistical Analysis
IBM SPSS Statistics (IBM SPSS Statistics 22) was used to analyze the data from the experiments. We used a one-way analysis of variance for the comparison of means in multiple groups studied here. We expressed the measurement data of normal distribution based on mean ± standard deviation. A difference was considered significant when its P value was lesser than .05.
Results
Between August 2013 and January 2015, 216 patients were eligible for the study and underwent routine esophageal manometry and pharyngeal and distal esophageal pH monitoring. Of the total participants, 98 were males, and 118 were females. In males, the average age was 54 ± 14 years, while in females, it was 54 ± 12 years.
Reflux Disease Distribution
Based on the pH monitoring of the laryngopharynx and the distal esophagus, 100 of 216 patients did not meet the total diagnostic criteria of LPR or GERD. A total of 116 patients fulfilled at least 1 diagnostic criterion. Among these, 34 patients satisfied the criteria for isolated LPR (iLPR), 44 for GERD, and 38 for GERD&LPR. Overall, 82 among these 216 patients had GERD, and 72 patients had LPR. Further, 46.3% (38/38 + 44) of patients with GERD had LPR, while 52.7% (38/38 + 34) presenting with LPR had GERD as encountered in clinical settings.
Thus, the patients were divided into 4 groups: no reflux disease (NRD), iLPR, isolated GERD (iGERD), and GERD&LPR. The mean RSI score of each groups is 9.92 ± 6.70, 14.21 ± 8.89, 13.39 ± 7.35, 13.32 ± 8.20, respectively. There was no difference in their age (P = .934; see Table 1).
Reflux Disease Distribution.
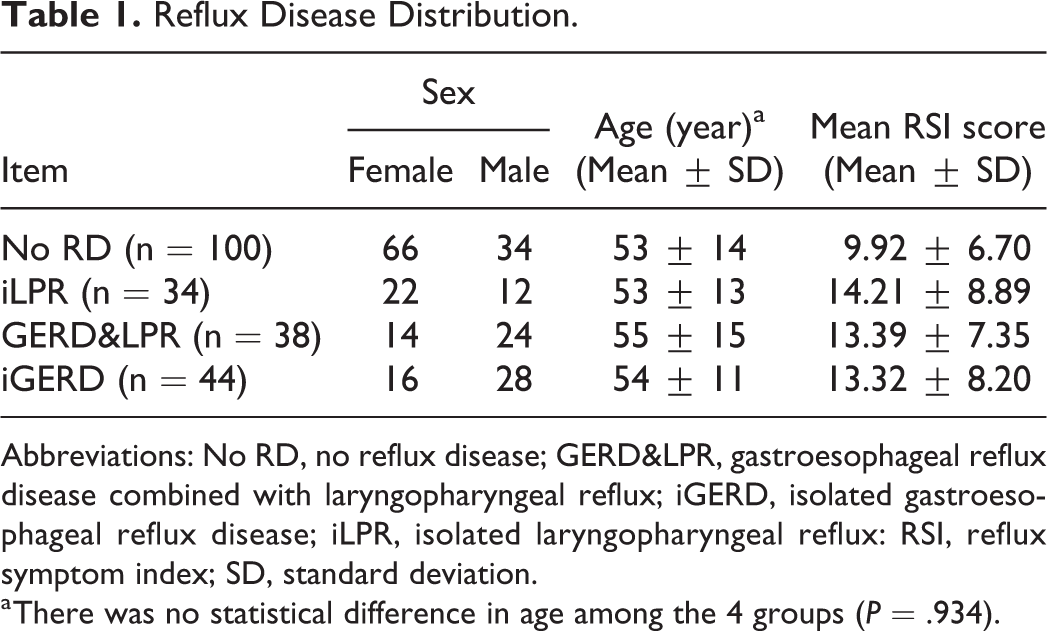
Abbreviations: No RD, no reflux disease; GERD&LPR, gastroesophageal reflux disease combined with laryngopharyngeal reflux; iGERD, isolated gastroesophageal reflux disease; iLPR, isolated laryngopharyngeal reflux: RSI, reflux symptom index; SD, standard deviation.
a There was no statistical difference in age among the 4 groups (P = .934).
Comparison of the Reflux Parameter in the Laryngopharynx Between the Patients in iLPR and GERD&LPR Groups
There was no significant difference in the total number of reflux events between the groups, iLPR and GERD&LPR. Additionally, no significant difference was found in the number of upright reflux events, the upright reflux time, and the percentage of upright reflux time between the 2 groups. However, the total reflux time and the percentage of total reflux time were statistically different for the 2 groups. Overall, the total reflux time varied from 17.82 ± 18.34 (GERD&LPR group) versus 9.62 ± 9.58 (iLPR group; P = .023). The percentage of total reflux time varied from 1.318 ± 1.377 (GERD&LPR group) versus 0.70588 ± 0.72736 (iLPR group; P = .023). Overall, the GERD&LPR groups had significantly higher reflux times and percentage of total reflux time than the iLPR group (see Table 2).
Comparison of Reflux Parameter in the Laryngopharynx Between ILPR and Gerd&LPR Groups.
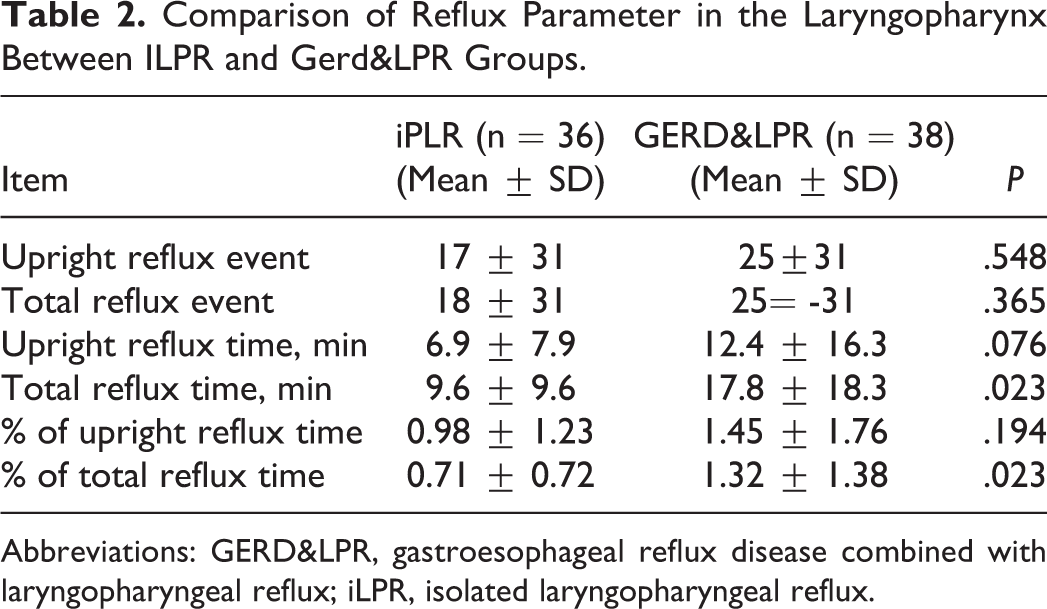
Abbreviations: GERD&LPR, gastroesophageal reflux disease combined with laryngopharyngeal reflux; iLPR, isolated laryngopharyngeal reflux.
Comparison of the Reflux Parameter in the Distal Esophagus Between the Patients in iGERD and GERD&LPR Groups
There was no statistical difference between the 2 groups, iGERD and GERD&LPR, based on the number of refluxes in the distal esophagus. In contrast with the previous comparison, there was no difference in the total reflux time, percentage of total reflux time. Number of upright reflux times, upright reflux time, and the percentage of upright reflux time were also not statistically significant (see Table 3).
Comparison of Reflux Parameter in the Distal Esophagus Between the IGERD and GERD&LPR Groups.
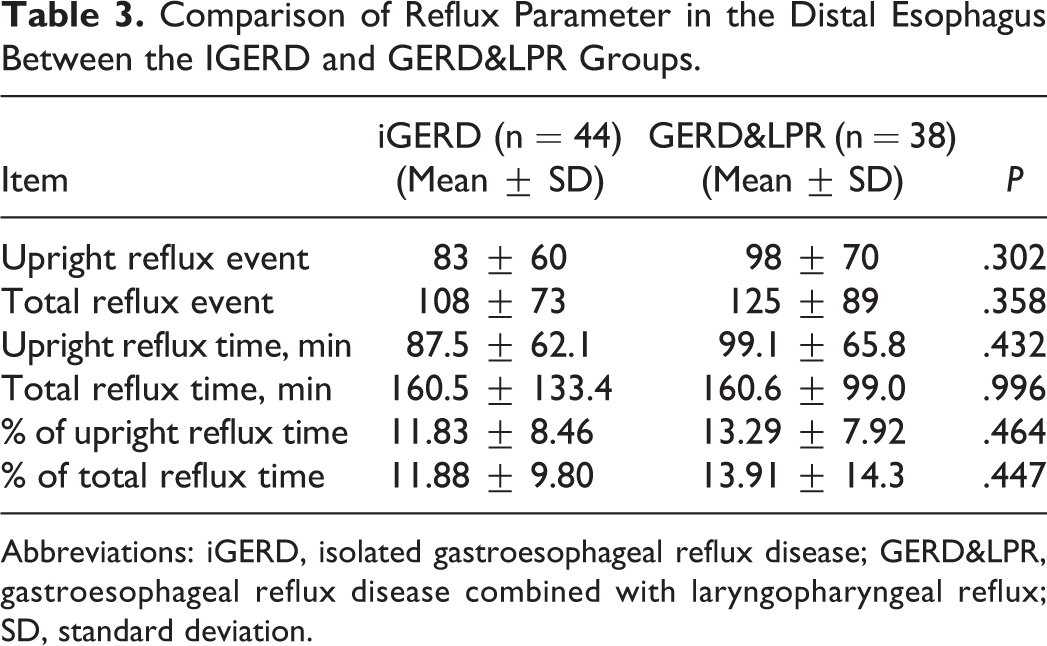
Abbreviations: iGERD, isolated gastroesophageal reflux disease; GERD&LPR, gastroesophageal reflux disease combined with laryngopharyngeal reflux; SD, standard deviation.
Discussion
From the results of the study, it is apparent that the relationship between LPR and GERD is extremely close. Some scholars describe that LPR is a part of the extraesophageal manifestations of GERD, 9 whereas others believe that LPR is a separate entity. The remaining agree that LPR is a multifactorial syndrome, and GERD is not the only cause involved in its pathogenesis. 10
A few years ago, we surveyed the relation between GERD and LPR based on the symptoms and found that GERD and LPR can coexist with each other and also independently. 6 It is widely acknowledged that the objective evidence of reflux is reflux monitoring. Therefore, it is necessary to study the relationship by adopting the reflux monitoring method. Among the methods of reflux monitoring, a specific oropharyngeal monitoring method is used for the detection of reflux in oropharynx. We had used it in previous researches. 11,12 It can avoid the possibility of drying out the probe in monitoring. However, it was expensive and could not provide another pH electrode for the distal esophagus. Regardless of the fact that the combined impedance-pH monitoring can reflect reflux more accurately, 13 its uniformity on normal value standards of LPR has minimized the use in reflux monitoring, which has not yet reached an agreement. We thereby chose a dual pH probe catheter in the laryngopharynx and esophagus.
The pH electrode of the laryngopharynx is generally placed 1 to 2 cm above the UES, and the pH electrode of the distal esophagus is placed at 5 cm above the LES. Due to the different lengths of the esophagus, the spacing between the UES and LES varies. Therefore, to diagnose LPR and GERD simultaneously, the distance between the 2 pH electrodes should vary depending on the distance from the UES to the LES. Many previous studies on LPR had not performed distal esophageal pH monitoring simultaneously, or the interelectrode distance used in the study was fixed. Unlike most researches, we adopted double-pitch electrode catheters with different spacing, which is a significant strength of this study. The pH catheter, in this study, was selected based on the results of esophageal manometry.
In this study, we found that in patients with symptoms related to LPR or GERD, it can either be iLPR, iGERD, or GERD&LPR. Some patients fail to meet any diagnostic criteria and are, thus, categorized under NRD. Approximately 46.3% of patients with GERD can be combined with LPR, and 52.7% of patients with LPR can be combined with GERD, indicating that the 2 are closely related. The results of this study are similar to our previous symptom-based study. 6 The only difference is that the ratio of GERD&LPR is higher on the basis of pH monitoring.
The reflux parameters in the distal esophagus were compared between patients with iGERD and GERD&LPR. There was no significant difference in the upright reflux events, upright reflux time, the percentage of upright reflux time, total reflux event, total reflux time, and percentage of total reflux time. This study did not clarify the exact reasons for this findings. Benjamin eta l 14 found that patients with GERD had more esophageal dysmotility than iLPR or GERD&LPR, which further perplexed the findings of our research. Frieling et al 15 found that there was no causal link between symptoms suspicious of extraesophageal reflux and esophageal motility disorders. In short, the impact of esophageal motility on the occurrence of LPR requires more in-depth research to reach a common agreement.
Recently, it was reported there were no significant differences in the pharyngeal reflux-related indexes between the pure LPRD group and the LPRD + GERD group. 16 However, the methods to ensure the distal esophageal electrode 5 cm above LES and the pharyngeal pH probe were not the same as in the esophagus. Another report had divided the patients into 4 groups similar to our research, but the literature has the same defect. 17 The results obtained in our study are significantly different from previous research. 16,17 The total reflux time and the percentage of reflux time in patients with GERD&LPR were significantly higher than those in patients with iLPR, but there was no significant difference in the upright reflux time and the percentage of upright reflux time in these patients. Overall, the reflux events in the laryngopharynx of iLPR group occur more frequently in the upright position, while in the GERD&LPR group, they are relatively higher in the supine position. This suggests that reflux episodes in the laryngopharynx occur in patients with GERD&LPR may be derived from GER rather than existing independently. As clinical therapy, iLPR may be more difficult to manage than GERD&LPR, of course, it should be researched in the future.
The independent existence of LPR in the absence of GERD can be understood through several possible situations. Foremost, there is an independent LPR condition in which the reflux originates from the heterotopic gastric mucosa of the cervical esophagus rather than the stomach itself. 18,19 Secondly, reflux events detected in laryngopharynx just are secondary to GER. Patients met both of diagnostic criteria and named as GERD&LPR. Thirdly, reflux events detected in laryngopharynx just are secondary to GER and meet the diagnostic criteria for LPR but reflux in distal esophagus did not meet the criteria for GERD. The LPR contents have originated from the stomach. These patients whose reflux in laryngopharynx secondary to GER should actually be diagnosed as GERD because of the reflux of origin (see Figure 1). In order to solve the contradiction, it is necessary to redefine abnormal acid exposure. In the past, we defined abnormal acid exposure only to define the percentage of time with pH <4.0 at a specific location (5 cm above LES), there was no definition of reflux height, reflux intensity, reflux nature, or other parameters. Combined impedance pH monitoring 13,20 can effectively distinguish the height, intensity, and content of reflux. It is expected that more studies in the area would make it possible to comprehensively define the reflux standard for GERD as well as compile the standard differentiation between LPR and GERD.
Conclusions
In summary, based on the synchronous esophageal and laryngopharyngeal pH monitoring, LPR can be manifested in combination with GERD or it can exist alone. Reflux episodes in laryngopharynx in patients with GERD&LPR may be derived from GER rather than exist independently. Regarding the relationship between GERD and LPR, it is necessary to redefine the abnormal reflux parameters, which can be determined by further research in the area. In addition, we have developed a new formula that can help us to select different spacing options of dual pH probe catheters.
Footnotes
Authors’ Note
Guijian Feng and Yulan Liu contributed to conception and design and administrative support. Yun WU, Junyao Wang, Qing Huang, Tao Peng, and Guijian Feng contributed to provision of study materials or patients. Yun WU, Junyao Wang, Qing Huang, Tao Peng, and Lili Zhao contributed to collection and assembly of data. Yun WU, Junyao Wang, Qing Huang, and Guijian Feng contributed to data analysis and interpretation. All authors contributed to manuscript writing and final approval of the manuscript. We declare that we have no financial and personal relationships with other people or organizations that can inappropriately influence our work, there is no professional or other personal interest of any nature or kind in any product, service and/or company. The Ethics Committee of Peking University People’s Hospital approved and supervised this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Capital Clinical Characteristics Application Research Project [Grant number: Z131107002213069] from the Beijing Municipal Science & Technology Commission, PRC.