
Abstract
It is very challenging to expose and remove tumors above the hard palate in the retrostyloid space using the typical cervical approach. Other approaches, such as the cervical–parotid approach, may result in prominent scars, facial paralysis, or masticatory dysfunction. Here, we report a case of a vagal neurofibroma between the internal carotid artery and internal jugular vein in the retrostyloid space. We used a 3D model to design a surgical approach that reduced the risk to the surrounding vessels and nerves. We performed an endoscope-assisted resection of the tumor using a posterior styloid approach. Following surgery, there were no obvious scars on the face or neck, facial paralysis, or dysphagia, but mild hoarseness.
Introduction
The selection of surgical method and approach for tumor resection is based on tumor location, size, adjacent anatomical structures, and a risk assessment. 1 The parapharyngeal space (PPS) is divided by the styloid diaphragm 2 (the stylopharyngeal septum) into the prestyloid and retrostyloid spaces. Surgery in the prestyloid space is relatively safe. However, cranial nerves IX to XII, the internal carotid artery (ICA), and the internal jugular vein (IJV) run through the retrostyloid space, making surgery challenging.
Some tumors in the prestyloid space can be resected using a minimally invasive oral approach. However, for tumors in the retrostyloid space, this approach risks injuring the ICA and the posterior group of cranial nerves. As operating across major blood vessels or nerves is not recommended, a cervical or cervical–parotid approach is usually applied to remove tumors in the retrostyloid space. However, it is difficult to clearly expose and completely remove tumors above the level of the hard palate when using a cervical approach, while it is difficult to retain intact the parotid gland, facial nerve, and ascending ramus of the mandible when using a cervical–parotid approach.
In this case, a vagal neurofibroma was located between the ICA and the IJV. The ICA was displaced anteriorly and the IJV was compressed behind the tumor. The surgical approach was designed with the help of a 3D model. An endoscope-assisted posterior styloid approach was selected to avoid injuring the ICA. In surgery, the tumor was exposed and removed within its capsule. The vital blood vessels and nerves were well protected.
Case Report
In September 2019, a 53-year-old male patient was admitted to the Department of Otolaryngology in the First Affiliated Hospital of China Medical University, presenting with a tumor in the right PPS that had been incidentally detected 3 months prior. He had initially consulted a doctor about “a cold” and complained of numbness of the right hand. Brain computed tomography had revealed the presence of a tumor. He had experienced no symptoms of nasal obstruction, hyposmia, headache, coughing after drinking, epistaxis, or facial numbness. He had no smoking or alcohol drinking habits.
Physical examination indicated that the nasal septum was not deviated, and both nasal passages were unobstructed. There were no obvious abnormalities in acoustic conduction and electric response audiometry.
Skull base imaging revealed that the tumor was located in the right PPS, with clear boundaries and dimensions of 4.2 × 2.3 × 5.9 cm. The lesion displayed heterogenous contrast enhancement, with a distinct central region. The upper boundary of the lesion extended to the jugular foramen, causing displacement and compression of the ICA (Figure 1).
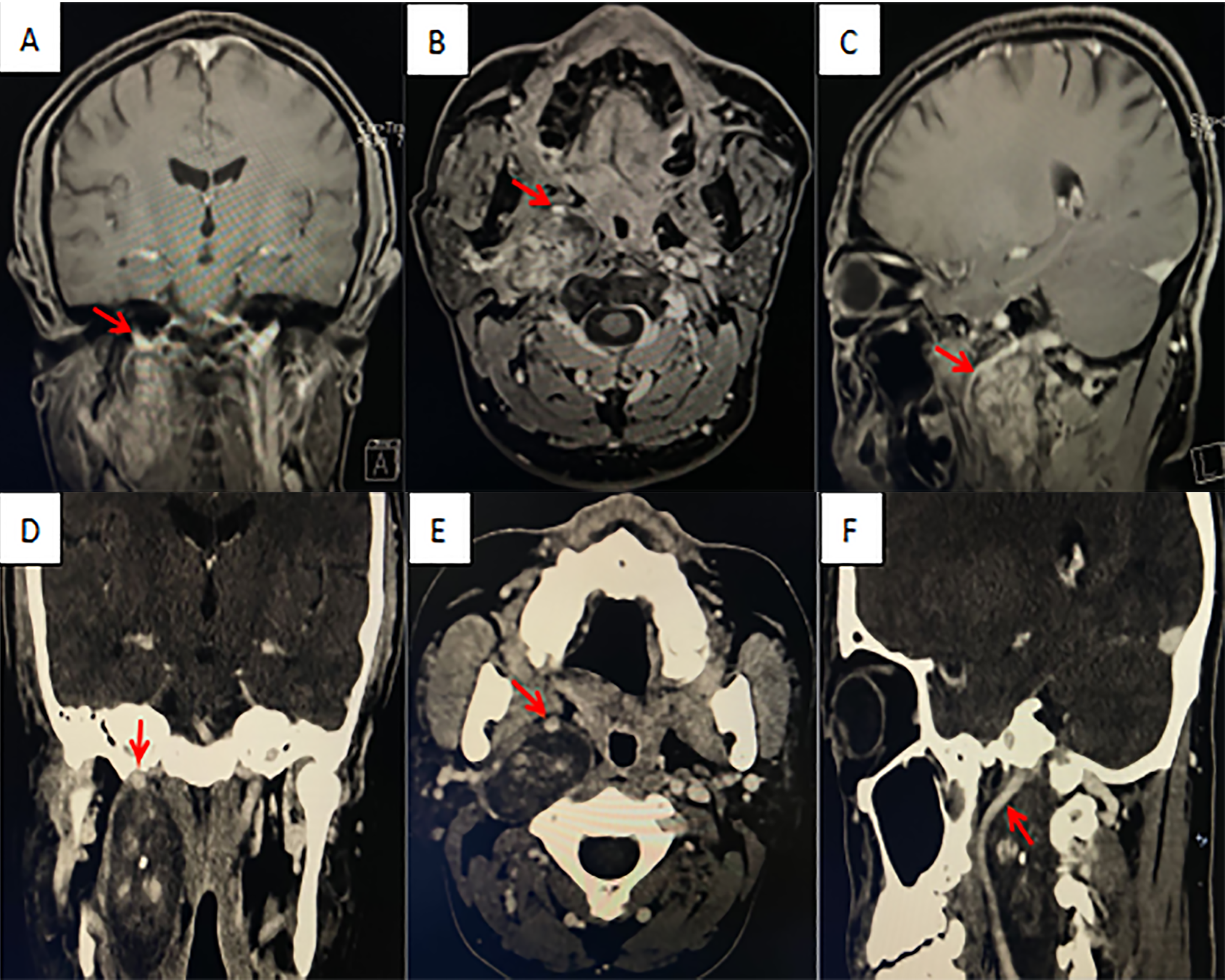
Preoperative images of the skull base of a patient with a neurofibroma. A and D, Coronal plane; B and E, Transverse plane; C and F, Sagittal plane; A-C, Contrast-enhanced magnetic resonance imaging (MRI); D-F, Contrast-enhanced 3-dimensional computed tomography (3D-CT). The red arrow indicates the internal carotid artery.
Based on the imaging findings, the patient was diagnosed with as a lesion occupying the right PPS. Due to the lesion’s deep location and the vital blood vessels and nerves around it, it was not possible to biopsy the tumor for pathological examination prior to surgery. Using a 3D model (Figure 2), we mapped out a posterior styloid approach to remove the tumor.
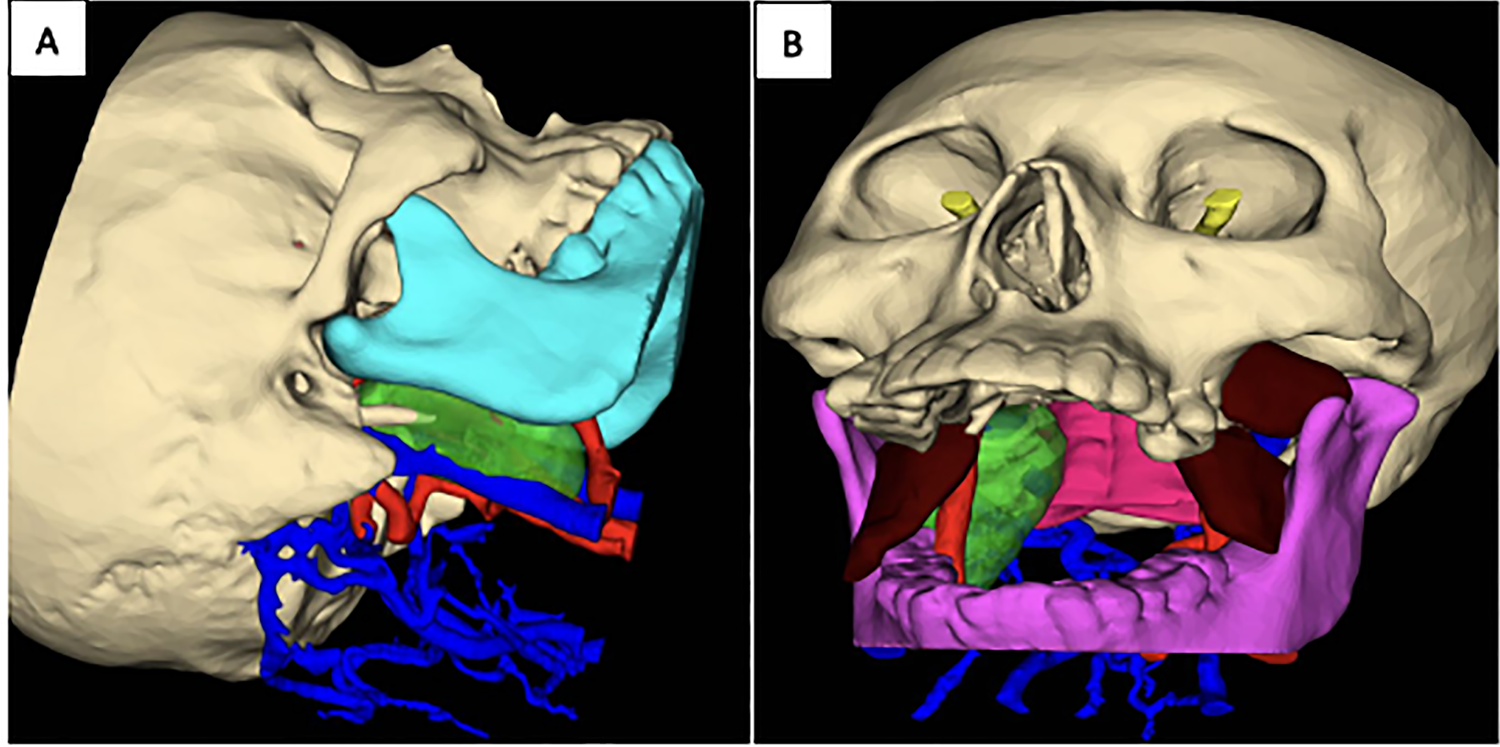
A 3D model was used to simulate the surgical approach prior to surgery. Red vessels represent arteries, blue vessels represent veins, and the green region represents the tumor. A, When simulating a cervical approach to avoid the risk areas of the internal carotid artery (ICA) and internal jugular vein (IJV), the tumor can be observed. B, When simulating an oral approach, the compressed ICA blocks the tumor from view, concealing its exact location.
On September 16, 2019, considering that the patient was found to have tumors in the retrostyloid space before surgery, and no relevant space-occupying symptoms have appeared, conservative treatment may also be considered. However, in the future, the risk of reoperation may be higher than it is now because of the enlargement of the tumor and compression of the surrounding blood vessels and nerves. After fully communicating the risks related to the operation with the patient, the patient decided to actively adopt the surgical treatment plan and sign an informed consent form at the same time. The patient underwent tumor resection under general anesthesia. A right lateral neck 3 cm incision on the right lateral neck was made and a posterior styloid approach was used. Image navigation was used to assist in locating the lesion. During the operation, the right side of the neck was incised between the mastoid process and the mandibular angle. The parotid gland and the anterior edge of the sternocleidomastoid muscle were separated by blunt dissection. The lower edge of the parotid gland was exposed and turned up, the hypoglossal nerve was protected, and the tumor was located between the posterior edge of the ascending branch of the mandible and the mastoid process. The tumor had a smooth capsule, the lower boundary of which was connected to the vagus nerve.
The capsule was opened, and the tumor was biopsied for pathological examination. The biopsy results, which were returned during surgery, confirmed that the tumor was a neurofibroma. The tumor was resected intracapsularly from the anterior border of the styloid diaphragm and ICA, posteriorly from the prevertebral fascia, and superiorly from the jugular foramen, along with the abundant nerve capsule (Figure 3).
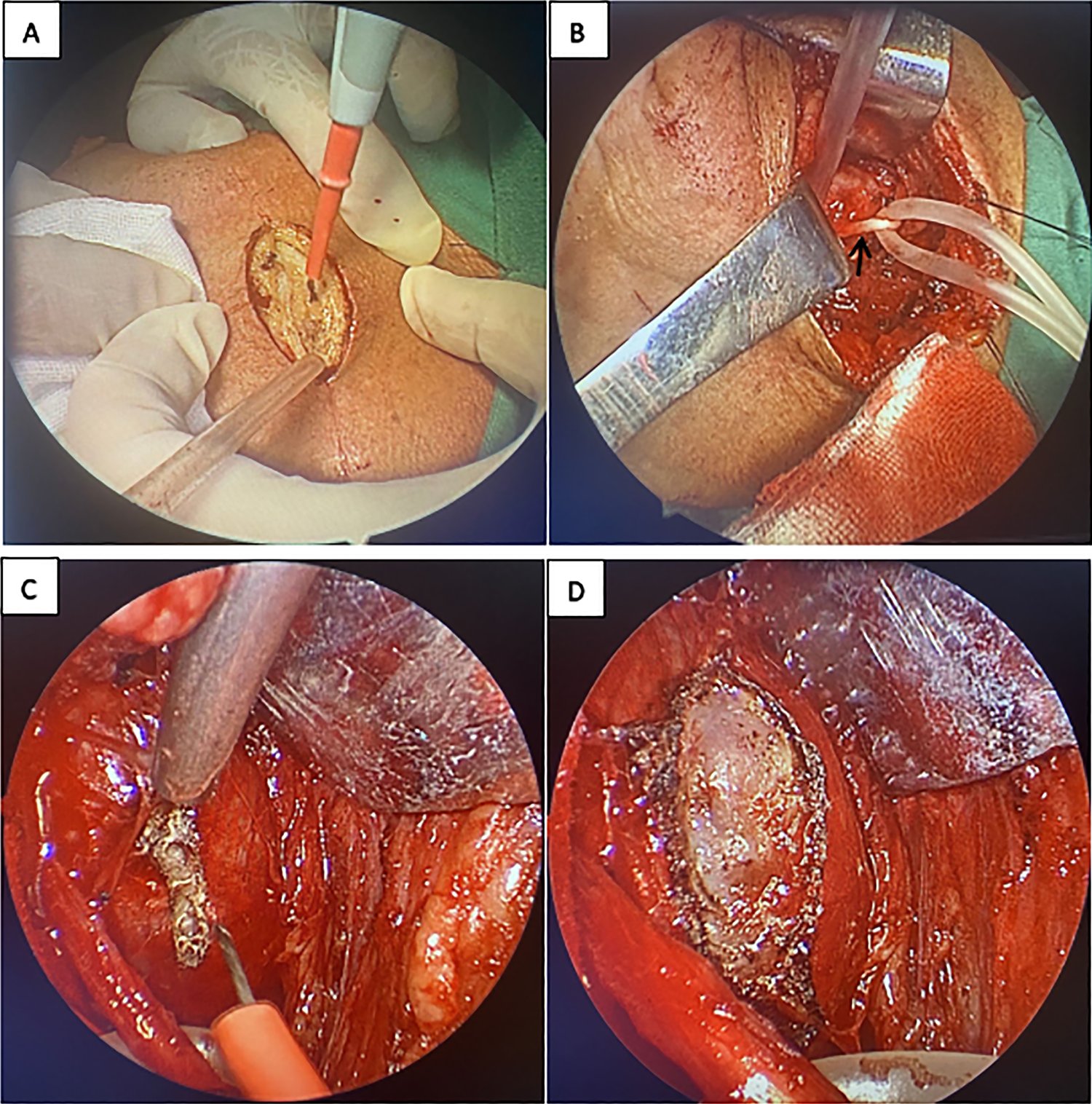
Surgical images of the resection of a neurofibroma from the retrostyloid space. A, Surgical incision; B, Exposure and protection of the sublingual nerve (black arrow); C, Freeing of the surrounding tissue and incision of the tumor capsule; D, The condition of the tumor after incision of the capsule.
There were no complications other than mild hoarseness after operation. Laryngoscopy showed that the right lateral walls of the nasopharynx, oropharynx, and hypopharynx were slightly swollen. Submucosal congestion was observed in the right vocal cord, along with significantly limited adduction and abduction, while movement of the left vocal cord was normal.
The patient underwent reexamination at 14 days and 1 month after surgery. At 1 month, the hoarseness had improved. Reexamination using dynamic laryngoscopy showed that the right vocal cord was fixed in the central position, while the left vocal cord was normal. No other abnormalities were found. The incision healed well, without swelling or infection. Three months after surgery, enhanced magnetic resonance imaging of the skull base showed no apparent residual tumor or signs of recurrence (Figure 4).

Contrast-enhanced magnetic resonance imaging (MRI) of the skull base, 3 months after surgery. A, Coronal plane; B, Transverse plane; C, Sagittal plane. The red arrow indicates the surgical site.
Discussion
The PPS is divided into a narrow prestyloid space and a large retrostyloid space by the styloid diaphragm: a thin fibrous layer that is attached to the stylohyoid, styloglossus, and stylopharyngeus muscles. 2 In this case, a vagal neurofibroma was located in the retrostyloid space. There are 3 commonly used surgical approaches for the resection of a tumor in this area: cervical, cervical–parotid, or transoral approach. However, the first 2 of these approaches were considered to have a high risk of causing facial nerve injury and possibly requiring removal of part of the ascending ramus of the mandible, due to the deep location of the tumor. This would have resulted in a long recovery time and a poor life quality.
As shown in Figure 2, when the ICA is anteriorly displaced by a tumor, it can easily be injured and cause massive bleeding during surgery. In addition, the adjacent glossopharyngeal nerve 3 may be affected, resulting in dysphagia. To avoid injury to the ICA, IJV, and other important nerves, as well as to obtain deeper and better surgical vision up to the Jugular foramen and the skull base, an endoscope-assisted posterior styloid approach was selected in this case. This required only a small incision (approximately 3 cm) and did not affect the mandible, 3 greatly improving the patient’s quality of life after surgery.
A total of 80% of tumors in the PPS are benign, 4 and most of the malignant tumors are metastatic tumors. Due to the slow growth of parapharyngeal neurilemmomas and neurofibromas, intracapsular resection can be used as an alternative to complete resection. Compared with complete resection, intracapsular resection can reduce unnecessary nerve function defects and reduce the incidence of complications unrelated to the involved nerves. Although some paralysis is inevitable, intracapsular resection can greatly reduce its severity, which may improve patient outcomes. 5 In this case, 3 months after surgery, the patient’s soft palate motor function (vagal innervation) was good (Figure 5).

Postoperative observation of soft palate movement. Following the right-side neck endoscopic approach, bilateral soft palate lifting was improved. The black arrow indicates the right soft palate, and the red arrow indicates the left soft palate.
In this case, prior to surgery, a 3D model was used to simulate the surgical approach. The possible risks of various surgical approaches were thoroughly evaluated, based on the location of the tumor and the peripheral blood vessels and nerves involved. We opted for a minimally invasive intracapsular resection using a posterior styloid approach, which resulted in good patient outcomes.
Supplemental material
Supplemental Material, Certificate_of_editing-HAIUJ_1 - Endoscope-Assisted Resection of a Vagal Neurofibroma Using a Posterior Styloid Approach
Supplemental Material, Certificate_of_editing-HAIUJ_1 for Endoscope-Assisted Resection of a Vagal Neurofibroma Using a Posterior Styloid Approach by Qiu-Ju Han, Yan Wang and Hong-Quan Wei in Ear, Nose & Throat Journal
Footnotes
Authors’ Note
This is the first submission on this topic, and this research has not been presented at a scientific meeting. The patient was informed of the intent to publish this case report and the accompanying images, which do not invade his privacy or infringe on any of his interests. The patient agreed to publish his images and provided signed informed consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Hong-Quan Wei received funding from the Natural Science Foundation of Liaoning program, grant number 20170540985, for the project “Application of 3D printing technology in the clinical practice and teaching of nasal skull base surgery.”
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.