
Abstract

A 21-year-old male with no significant past medical or family history presented to the emergency department (ED) with recurrent, acute-onset, large-volume oropharyngeal bleeding. Three days prior, he was seen in the ED for 2 days of intermittent bleeding that had acutely worsened and was associated with hematemesis, severe left-sided neck pain, mild sore throat, and hoarseness. The patient denied any preceding coughing, oral trauma, recent tonsillar infection, dysphagia, weight loss, otalgia, fevers, or chills. As an actor, he attended drama class daily and endorsed a recent increase in effortful yelling and straining. The bleeding was localized to the left palatine tonsil (Figure 1A). A computed tomography angiogram (CTA) of the neck showed no evidence of a hematoma, vascular malformation, or active extravasation. The area of concern was treated with bedside silver nitrate cauterization with a plan for close outpatient follow-up. A, This is a pseudoaneurysm of the left tonsil presenting with ecchymosis and bleeding. B, A 5 mm round focus of arterial contrast extravasation (yellow arrow) is seen on computed tomography angiogram. C, Carotid angiography reveals a 4 mm × 3 mm × 4 mm pseudoaneurysm (yellow asterisk) of the tonsillar branch of the left facial artery. Branches shown here include facial (FA), lingual (LG), occipital (OC), superficial temporal (STA), and internal maxillary (IMAX) arteries.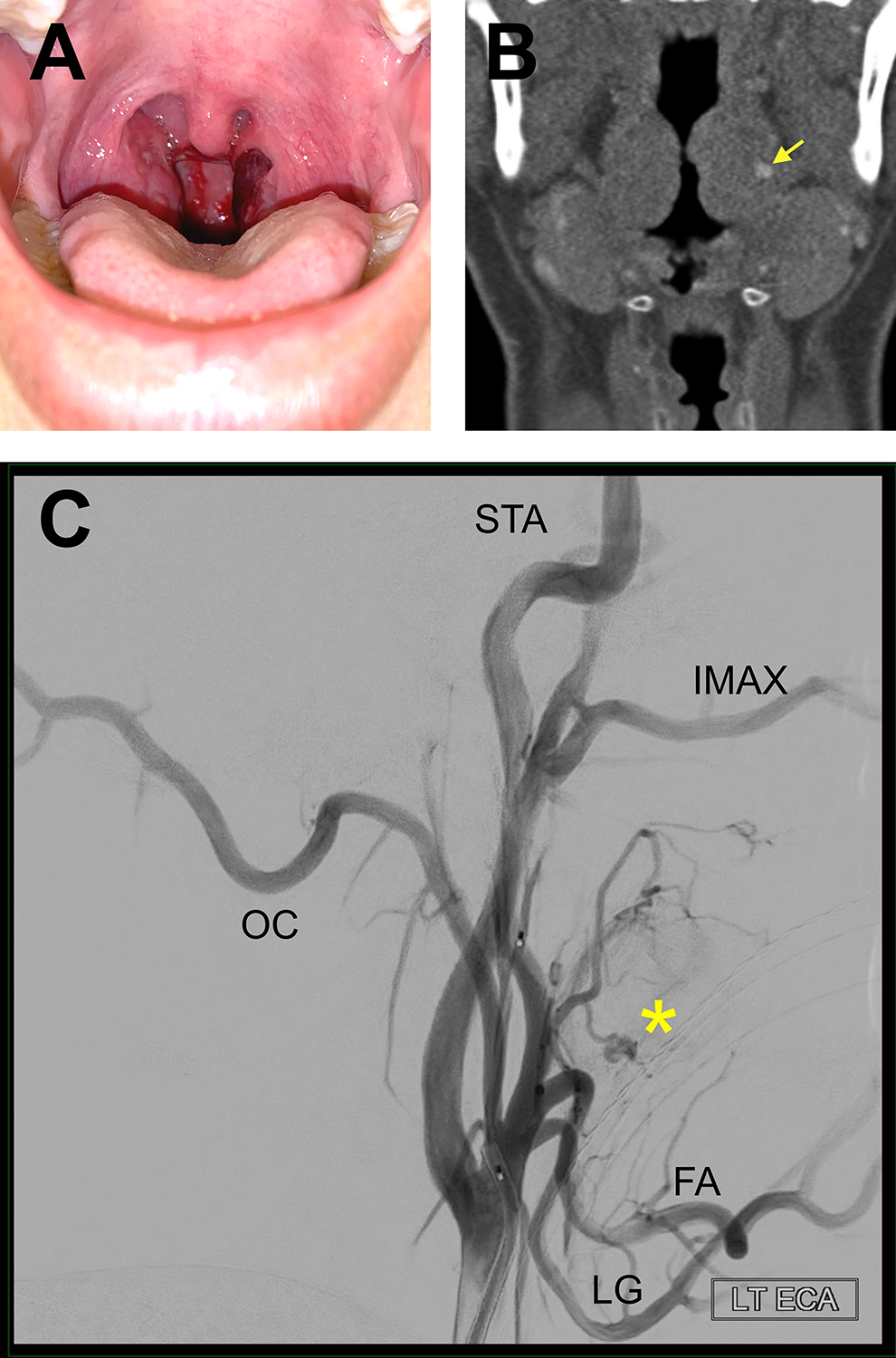
Recurrent bleeding 2 days later prompted his return to the ED. The examination was remarkable for a large clot on the left palatine tonsil and bloody secretions along the posterior pharyngeal wall which were seen on flexible fiber-optic laryngoscopy. The remainder of the oropharyngeal examination including the bilateral tonsillar areas, posterior pharyngeal wall, and soft palate and uvula were nonerythematous, nonedematous, and without exudates. Complete blood count and coagulation studies were all normal. Repeat CTA of the neck revealed a 5-mm enhancing focus in the left palatine tonsil, likely representing contrast extravasation (Figure 1B).
A neurointerventional radiologist performed a cerebral angiogram and discovered a 4 mm × 3 mm × 4 mm pseudoaneurysm of the tonsillar branch of the left facial artery (Figure 1C). The tonsillar and ascending palatine branches of the left facial artery were successfully embolized with superselective polyvinyl alcohol particles. Complete obliteration of the pseudoaneurysm was visualized following embolization (Figure 2A and B).
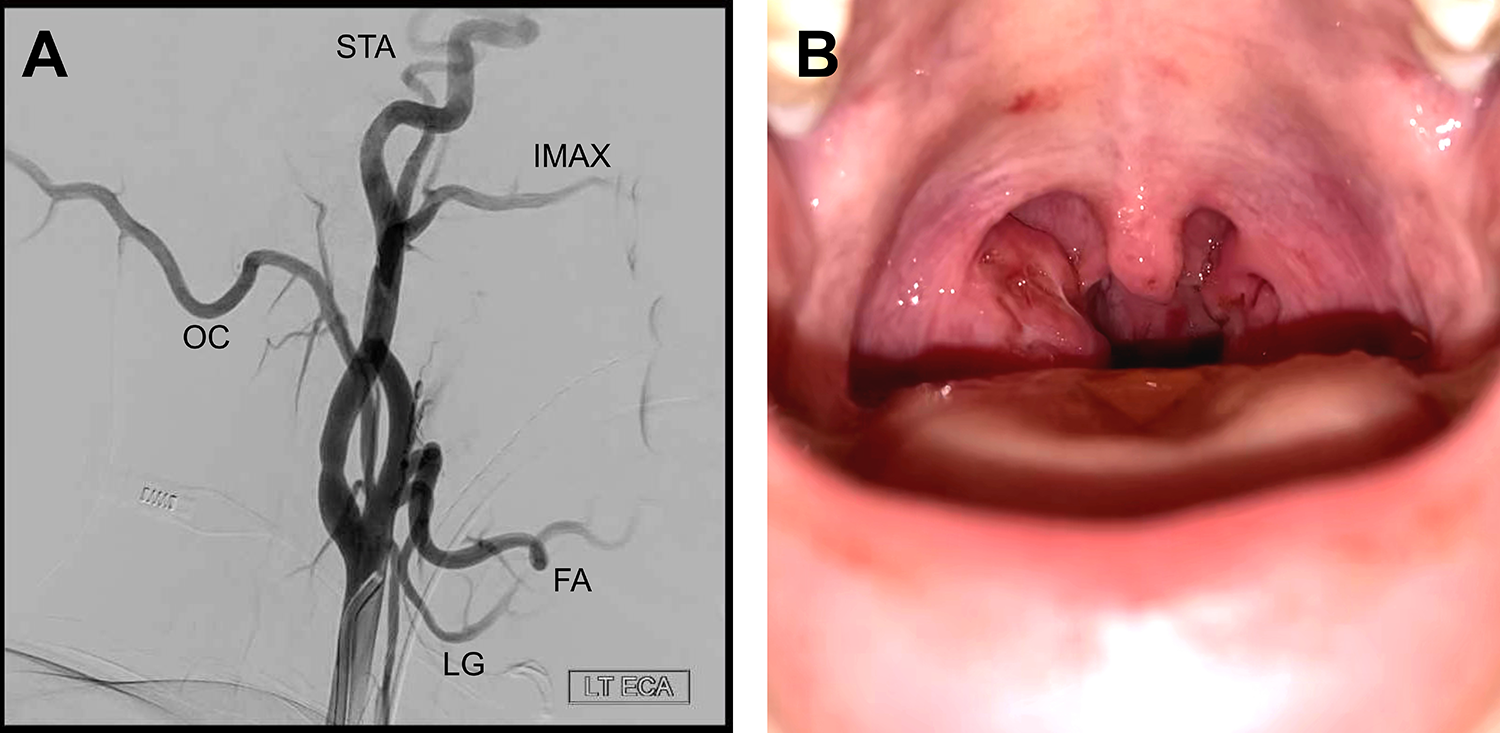
A, Postembolization angiogram demonstrates successful embolization of the tonsillar branch of the left facial artery. Branches shown here include facial (FA), lingual (LG), occipital (OC), superficial temporal (STA), and internal maxillary (IMAX) arteries. B, Resolution of the ecchymosis of the left tonsil 24 hours after embolization is seen here.
Testing for von Willebrand disease (vWD) came back negative. Two weeks later, the patient was doing well without recurrent bleeding and had returned to full vocal use.
Local inflammation, physical trauma, and iatrogenic causes have been implicated as possible etiologies of tonsillar artery pseudoaneurysms. Such pseudoaneurysms typically occur in the presence of known risk factors such as a peritonsillar abscess, injury, or recent tonsillectomy or radiation therapy. 1 While most pseudoaneurysms of inflammatory etiology are secondary to bouts of recurrent tonsillitis, they have been observed in isolated cases of tonsillitis. 2 Pseudoaneurysm formation secondary to trauma was thoroughly described in a study evaluating vascular injury in 124 patients with penetrating injury to the face and neck. A total of 13 pseudoaneurysms were discovered in 11 patients in which the majority involved branches of the external carotid artery. 3 There are several posttonsillectomy cases reported to be complicated by pseudoaneurysm development, primarily within the lingual, facial, or ascending pharyngeal arteries, all of which contribute blood supply to the tonsillar bed. 1 One review found that pseudoaneurysms in the head and neck have been reported to occur as early as 4 hours to as late as 8 months following surgery. 1
The differential diagnoses for recurrent, spontaneous tonsillar hemorrhage (STH) should include (1) occult bacterial tonsillitis; (2) vascular abnormalities such as arteriovenous malformation (AVM), venous malformation, and pseudoaneurysm; (3) bleeding disorders that could present with normal screening coagulation studies such as vWD, qualitative platelet disorders, or vasculopathies; and (4) benign or malignant tumors such as a tonsillar hemangioma, squamous cell carcinoma, or lymphoma of the palatine tonsil.
Initial assessment of this otherwise healthy patient with known heavy vocal use was superficial mucosal bleeding from straining and exertion. While occult infection is the most common cause of STH, this patient’s examination and laboratory values did not indicate infection. 4 Congenital AVMs can proliferate with hormonal changes or physical stressors; patients present with massive, potentially fatal, hemorrhage. 5 The most frequently encountered site of extracranial AVMs is in the head and neck, making this a relevant diagnosis to consider. 5 This patient’s significant vocal use may have been responsible for an acute proliferation and consequent rupture of a previously subclinical congenital AVM. An incompletely clotted hematoma following AVM rupture, which has been found to give rise to intracerebral pseudoaneurysms, could have then led to pseudoaneurysm development in this patient. 6 Spontaneous tonsillar hemorrhage could be a presenting symptom for vWD; however, it is usually responsive to cautery treatment. While STH can be a sign of early tonsil cancer, an attempt to biopsy the tonsil prior to ruling out vascular anomalies could be catastrophic. It is important to maintain a broad differential diagnosis for patients with acute, large-volume oropharyngeal hemorrhage. Pertinent clinical clues help determine the best route of action and avoid calamitous outcomes.
Footnotes
Authors’ Note
Iram Shafqat contributed to chart review, article preparation, manuscript writing and revision, and figure preparation. Albert Y. Han contributed to chart review, article preparation, manuscript writing and revision, and figure preparation. Marilene B. Wang contributed to chart review and manuscript writing and revision. Taylor R. Carle contributed to chart review and manuscript writing and revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.