
Abstract
We present a case of novel penetrating temporal bone trauma with a pintail comb causing facial paralysis. We describe a 42-year-old woman with acute facial paralysis, hearing loss, and dizziness following accidental tympanic membrane puncture. The patient underwent middle ear exploration with tympanoplasty and was found to have an intact but severely edematous facial nerve. The patient demonstrated less than 90% degeneration under electroneuronography and was treated medically without decompression, and by 6 months had exhibited complete resolution of facial nerve dysfunction with normal hearing. This case report highlights a unique cause of penetrating temporal bone trauma and supports the utility of electroneuronography in predicting the likelihood of recovery and need for decompression in patients where the facial nerve has obvious signs of trauma but remains grossly intact.
Keywords
Introduction
Hairdressing combs come in various shapes and sizes depending on their specific function. A pintail comb is a comb with a sharp, pointed handle on one end designed to help part or style the hair. This patient suffered penetrating trauma injury due to improper use of a pintail comb while relieving itchiness in the right ear. Although combs generally have been shown to cause traumatic tympanic membrane (TM) perforation, there have been no previously documented cases of the pintail comb isolated as the cause of temporal bone trauma or facial paralysis.
Penetrating trauma to the middle ear, TM, or adjacent inner ear structures has been reported in children and adults alike. These injuries can be self-inflicted, often seen with cotton-tipped applicators, ear picks, combs, or matchstick injury, as well as caused iatrogenically by caregivers and medical providers. 1 Tympanic membrane perforations from penetrating and blunt injuries tend to have a more favorable prognosis over blast trauma, thermal, or caustic injuries. 2 Factors associated with poor healing of penetrating traumatic injury are posterosuperior and larger-sized perforations. 3
Neurologic and otologic sequelae of penetrating trauma to the ear include vertigo, TM perforation, hemotympanum, perilymphatic fistula, ossicular chain disruption, sensorineural and/or conductive hearing loss, and significantly, facial nerve (FN) paralysis. 4 Facial nerve dysfunction rarely is associated with low-energy penetrating traumas without imaging evidence of bony fracture.
This case report evaluates the diagnosis and short- and long-term management of a patient with acute facial paralysis following penetrating temporal bone trauma from a pintail comb.
Case Report
A 42-year-old female without significant past medical history presented to the emergency department with acute-onset right facial paralysis, accompanied by right hearing loss and dizziness, after accidentally puncturing her eardrum with a pintail comb.
Her neurologic examination at presentation revealed ataxia and a right FN palsy graded as House-Brackmann (HB) grade 6/6. She had no other neurologic deficits.
Otoscopic examination revealed a small, central perforation of the TM without drainage. Temporal CT showed a clear middle ear and mastoid cavity and no displacement of bone involving the right fallopian canal in the tympanic and mastoid segment (Figure 1).
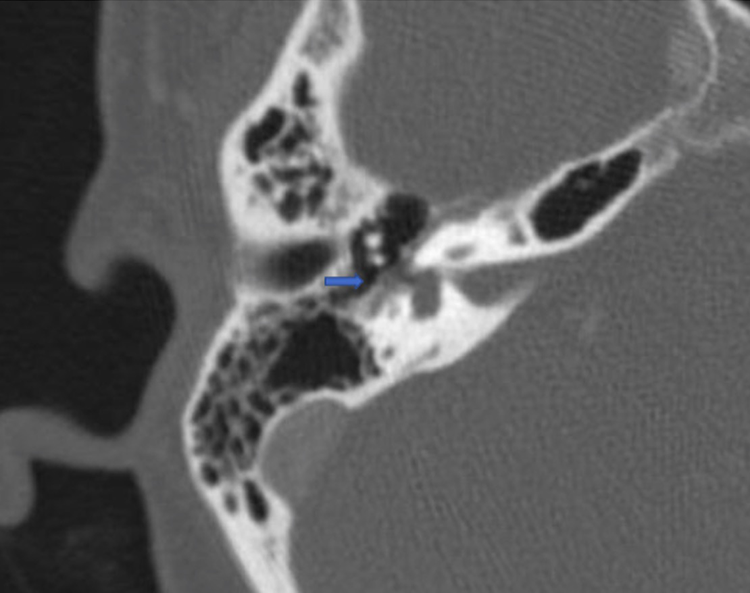
Preoperative axial temporal bone CT demonstrating a normal course to the facial nerve without visible disruption of the fallopian canal (arrow).
The patient was prescribed high-dose prednisone orally in a tapering dosage schedule over 14 days. She was seen by a neurotologist 7 days later and was found to have a persistent perforation and unchanged right HB 6/6 facial palsy. Audiogram showed borderline normal to mild conductive hearing loss (Figure 2). Surgical exploration was recommended because of the persistent paralysis and history of penetrating trauma.
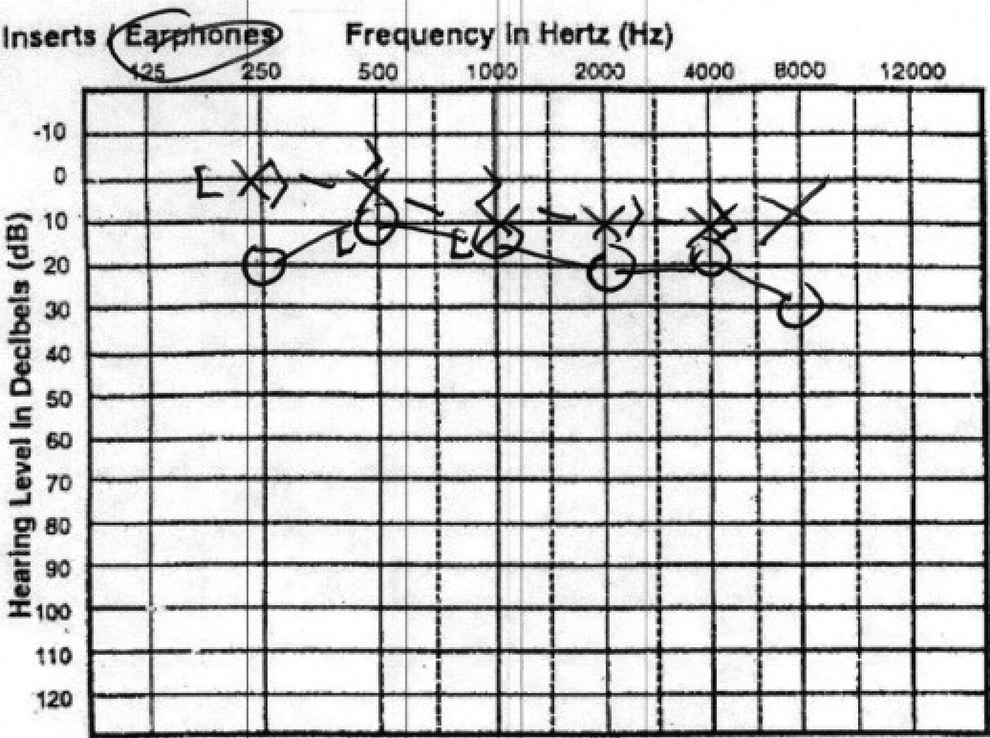
Preoperative audiogram showing borderline normal to mild conductive right hearing loss.
She underwent right middle ear exploration 11 days post-injury. The TM perforation was repaired with fascia, and the ossicular chain was found to be intact with normal mobility. The FN was found to be dehiscent and severely edematous but grossly intact (Figure 3). She was found to have minimal scutal overhang, which made the fallopian canal clearly evident as soon as the tympanomeatal flap was elevated.
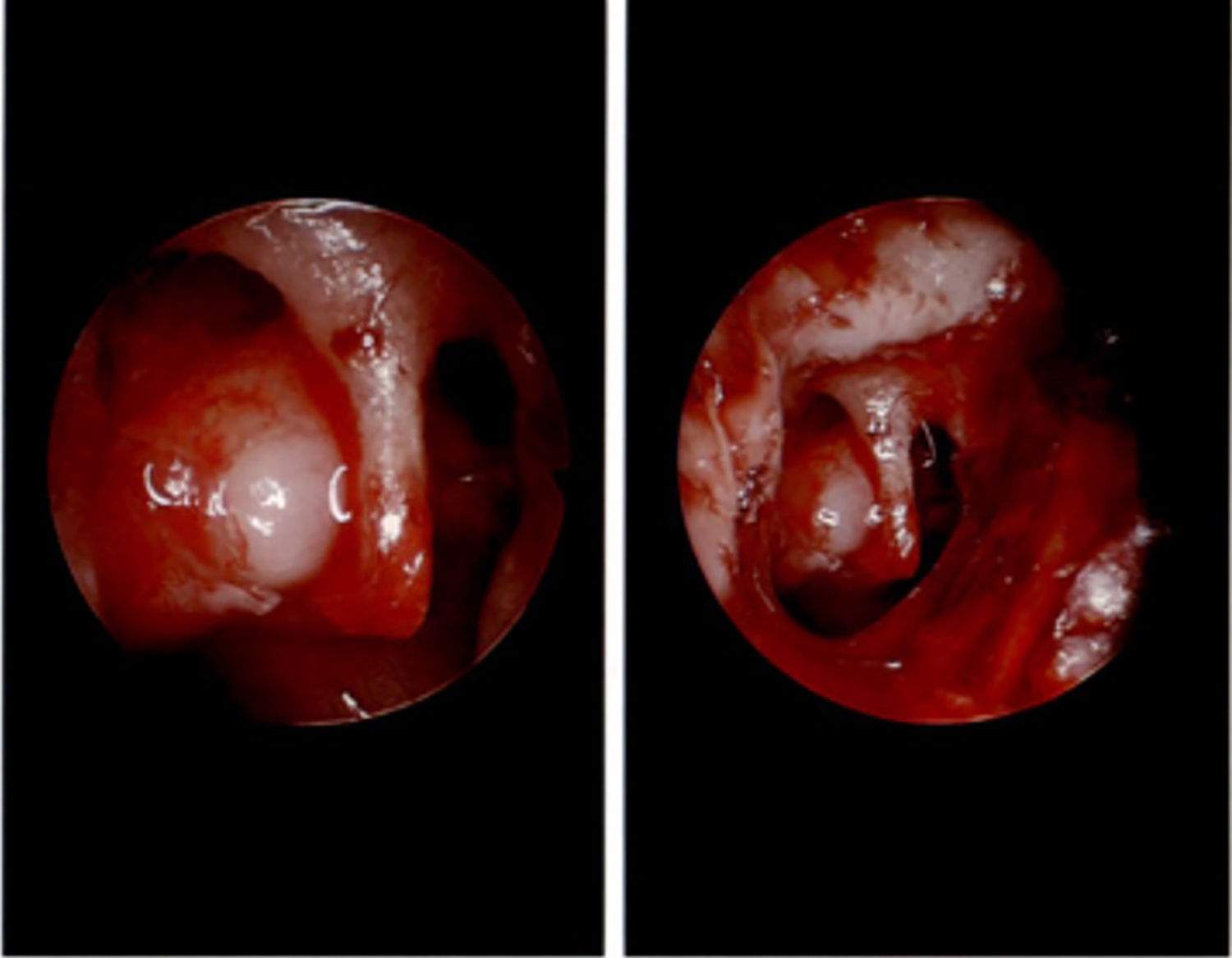
Intraoperative findings of middle ear exploration demonstrating intact ossicular chain and grossly intact but severely edematous right facial nerve.
The FN findings were verified by a second neurotologist who was asked to provide intraoperative confirmation. The proximal portion of the nerve stimulated at 2.5 mAmp but not below this level. Because the FN was found to be grossly intact, the decision was made not to perform FN decompression at the time of initial exploration.
Outpatient electroneurography (ENoG) testing was then performed, which revealed 20% weakness of the upper branch of the FN and 69% degeneration of the lower branches on the right side. Since the degree of degeneration was less than 90%, surgical decompression was not recommended.
The patient had significant improvement in right facial tone within 1 month of surgery, and within 2.5 months of surgery her facial function had improved to HB 2/6. By 6 months after the injury, her facial function had recovered to HB 1/6. Postoperative audiogram showed normal hearing and normal tympanograms in both ears.
Discussion
The most common mechanism of traumatic TM perforation presenting to the ED in the United States is foreign body instrumentation, and this is true of all age groups.5,6 Of foreign body instruments, combs are the fourth most common, comprising 5.5% of cases. 6
Like cotton-tipped applicators, pencils, lollipops, toothpicks, and matchsticks, pintail combs are long, pointed objects that can be easily inserted too deeply into the ear canal. In the majority of cases, penetrating trauma to the TM has a good prognosis with spontaneous resolution of the perforation, 2 as the mechanism of injury is distinct, and the injury is typically isolated. 7
Anatomically, an object as fine as a pintail comb can penetrate the external auditory canal medially through the TM, potentially disrupting the ossicular chain of the middle ear, and even injuring the inner ear. 7 This patient’s unique anatomy may have predisposed her to FN injury. In most patients, the scutum has a posterosuperior overhang which can serve a protective function for the FN against penetrating trauma, but in this case, the fallopian canal was immediately visible without needing to curette bone following tympanomeatal flap elevation.
Clinically, patients with acute onset facial paralysis following penetrating trauma should be considered for urgent surgical exploration. This patient additionally had dizziness raising suspicion for inner ear trauma and/or possible perilymphatic fistula, further supporting a role for urgent surgical intervention. At the time of surgical intervention, the FN was found to be severely edematous but anatomically intact. There remains controversy as to whether surgical decompression of the proximal and distal segments of the FN should be considered in a scenario when the FN is grossly intact but there is obvious evidence of injury. 8 For a grossly intact nerve, ENoG may hold prognostic value in determining the role of decompression even when intraoperative findings suggest a more severe injury. Patients with facial palsy who have less than 90% degeneration have been shown to regain normal facial movements spontaneously.8-10
Facial nerve decompression carries potential morbidity, including risk of additional FN injury and (when decompressing the tympanic segment) residual conductive hearing loss from the need to disarticulate the ossicular chain.
In our patient, it had been discussed preoperatively that FN decompression would only be performed at the time of the initial procedure if there was gross transection of the nerve. When the nerve was found to be anatomically intact, ENoG was used successfully to determine whether the benefit of FN decompression would outweigh its risks.
An individualized approach should be taken to each patient based on clinical presentation, imaging findings, and surgical management. This case report lends credence to the utility of conservative therapy following tympanoplasty in the context of incomplete FN degeneration on ENoG. Through this report, we hope to raise awareness of wide-ranging sequelae and provide our decision-making process for successful treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.