
Abstract
Objectives:
Postoperative respiratory depression is of concern in children undergoing adenotonsillectomy receiving postoperative opioids and may be mitigated with intraoperative bupivacaine. This study aims to compare the impact of bupivacaine on postoperative pain and sedation in various pediatric age and surgical indication subgroups.
Methods:
This is a case series with chart review of 181 patients <18 years old undergoing adenotonsillectomy at a tertiary care center (2013-2016). Postoperative outcomes were compared between those who received intraoperative bupivacaine before (pre-tonsillectomy) or after (post-tonsillectomy) tonsil removal and those who did not (none) using χ2 test and analysis of variance. Subanalysis was performed after stratifying into age and surgical indication subgroups.
Results:
Ninety-eight patients were included in the pre-tonsillectomy group, 47 in the post-tonsillectomy group, and 36 in the none group. The number of postanesthesia care unit opioid doses (P = .159) and pain scores at arrival (P = .362) or discharge (P = .255) were not significantly different between treatment groups overall. Among 0- to 5-year-olds, pre-tonsillectomy injection was associated with lowest mean (SD) discharge pain score of 0.55 (1.29) pre-tonsillectomy versus 0.71 (1.37) post-tonsillectomy versus 2 (1.63) none group (P = .004). Among 12- to 17-year-olds, no injection was associated with lowest mean (SD) discharge pain score of 2.33 (0.52) pre-tonsillectomy versus 5 (2.65) post-tonsillectomy versus 1.63 (1.60) none group (P = .020). Injection in patients with obstructive sleep apnea and/or sleep-disordered breathing did not improve postoperative outcomes.
Conclusion:
Intraoperative bupivacaine may improve pain scores in younger pediatric populations, though it may not impact the amount of postoperative opioid use. Prospective analysis with a larger sample size is warranted to better outline opioid usage and pain control in this group.
Introduction
With over 500 000 cases performed each year in children less than 15 years old, tonsillectomy or adenotonsillectomy (“tonsillectomy”) is one of the most commonly performed procedures in the United States. In children, it is mainly indicated for sleep-disordered breathing (SDB) and recurrent tonsillitis.1-3
An important consideration of tonsillectomy is postoperative pain, which can lead to reduced oral intake and dehydration.4-6 Nonsteroidal anti-inflammatory drugs are frequently used for pain relief after tonsillectomy, but their analgesic effect is often inadequate. 7 Though opioids may provide effective analgesia, their use may be problematic in the pediatric population as they are associated with risk of sedation, respiratory depression, and nausea. 8 Children undergoing tonsillectomy have especially been shown to carry a high risk of postoperative nausea and vomiting. 9 Tonsillectomies are also increasingly being performed for patients with obstructive sleep apnea (OSA), many of whom are at an increased risk of respiratory complications after general anesthesia and more sensitive to respiratory depression after opioid intake compared to other populations.10-13 The use of opioids for analgesia in certain pediatric patients may lead to delay in time to discharge from the postanesthesia care unit (PACU) whether that is to an inpatient unit or home. 9
Although there has been some controversy regarding the benefit of intraoperative bupivacaine infiltration into tonsillar beds, several studies have demonstrated injection of bupivacaine either immediately before or after tonsillar excision reduces postoperative pain.14-18 The decision to inject bupivacaine before or after excision, if at all, is predominantly at the discretion of the attending surgeon and can be influenced by their training or experience. The still subjective nature of when bupivacaine is given, combined with a lack of consensus on the use of bupivacaine in adenotonsillectomy and the large volume of adenotonsillectomies performed per year, warrants further exploration of the utility of this local anesthetic. Importantly, prior studies have not evaluated the effect of age or surgical indications such as OSA on the efficacy of bupivacaine. Therefore, the aim of this study was to evaluate the impact of intraoperative bupivacaine injection before or after tonsil removal on postoperative pain scores and sedation levels in different pediatric age groups with OSA, SDB, or other indications for surgery.
Patients and Methods
This case series was conducted with approval from the institutional review board of the Duke University Medical Center. Pediatric patients <18 years old who underwent tonsillectomy only or adenotonsillectomy at a tertiary care center between June 2013 and June 2016 were included. Tonsillectomy was identified by using CPT codes 42820, 42821, 42825, and 42826. Demographic information including age, gender, race, ethnicity, socioeconomic index, and percentage below poverty line was extracted using Duke Enterprise Data Unified Content Explorer. Surgery type, indication for surgery, ablative technique, surgical indication, PACU pain and sedation scores at arrival and discharge, length of stay, opioid analgesic use, and readmissions were collected from the electronic medical record. Pain scores using the Face, Legs, Activity, Cry, Consolability (FLACC) pain scale, the Wong-Baker FACES pain scale, or the rating pain scale were recorded.19,20 The Wong-Baker FACES pain scale was converted to a corresponding number on the numerical rating pain scale. This allowed for a more standardized comparison among the groups. The Richmond Agitation-Sedation Scale was used to score the level of sedation upon PACU arrival and discharge. Patients who did not meet the above inclusion criteria or those with missing demographic information were excluded from the analysis. Patients were discharged from the PACU either to an inpatient pediatric floor or to home depending on their preoperative assessment and how they did in PACU postoperatively.
Patients
The cohort was divided into 3 comparison groups: pre-tonsillectomy injection group—plain bupivacaine (0.25%) injected into tonsillar beds prior to resection, post-tonsillectomy injection group—bupivacaine injected into the postoperative tonsil bed, and no injection group. Patients were divided into 3 age subgroups (0-5 years old, 6-12 years old, and 12-17 years old), and treatment effects were compared. Our cohort was also subdivided by surgical indication—patients diagnosed with OSA on sleep study, non-OSA SDB (eg, snoring, mouth-breathing, and restless sleep), or neither.
Surgical and anesthetic techniques
Given that no epinephrine was mixed with bupivacaine, surgery was initiated immediately after bupivacaine injection in the pre-tonsillectomy group. The decision when and whether to inject was based on surgeon’s practice protocol, and the timing of bupivacaine injection was not influenced by the patient’s preoperative status.
Statistical analysis
Categorical variables are reported as counts and percentages, while continuous variables are reported as means and SD. Analysis of variance (ANOVA) and χ2 test were used to compare patient characteristics and postoperative outcomes. A P value <.05 was considered to be significant. All analyses were developed a priori, and therefore multiple comparisons testing was not applied. All statistical analyses were conducted using R version 3.3.3.
Results
A total of 181 patients were included in the study: 98 patients in the pre-tonsillectomy injection group, 47 in the post-tonsillectomy injection group, and 36 in the no injection group. Mean (SD) age was 6.53 (3.49) years, and age ranged from 13 months to 17.3 years. Forty-seven percent of ablations were performed via electrocautery, and 50.8% were performed via coblator. Median (IQR) bupivacaine dose in pre-tonsillectomy patients was 0.30 (0.29) mg/kg and 0.25 (0.20) mg/kg in post-tonsillectomy patients. Of the 181 patients, 2.8% received oral acetaminophen and 3.9% received dexmedetomidine preoperatively. There was no significant difference in the number of patients who received preoperative acetaminophen or dexmedetomidine among the treatment groups (P > .05).
Overall, 61.9% of patients received intraoperative intravenous (IV) acetaminophen. 62.2% of pre-tonsillectomy injection patients, 66% of post-tonsillectomy injection patients, and 55.6% of no injection patients received intraoperative IV acetaminophen (P = .591). The median (IQR) intraoperative IV acetaminophen dose given were 14.3 (15), 14.4 (14.9), and 9.8 (14.7) mg/kg for pre-tonsillectomy, post-tonsillectomy, and no injection patients, respectively. The no injection group most frequently received intraoperative fentanyl (70.4% pre-tonsillectomy vs 91.5% post-tonsillectomy vs 100% no injection, P = .83) and least frequently dexmedetomidine (72.4% vs 63.8% vs 33.3%, P = .01). 13.3% of patients received oral or IV acetaminophen after surgery, with a mean dose of 424.3 mg.
Patients with diagnosed OSA comprised 42.9% of the pre-tonsillectomy injection group versus 25.5% of the post-tonsillectomy injection group versus 18.9% of the no injection group (P = .015). There were no differences in the proportion of patients who received opioids between surgery finish time and PACU arrival (P = .884; Table 1). The groups received a comparable number of opioid doses within 2 hours of PACU arrival (1.1 vs 1.1 vs 0.8, P = .28).
Patient Characteristics and Postoperative Outcomes in Pre-Tonsillectomy Injection Versus Post-Tonsillectomy Injection Versus No Injection Groups.
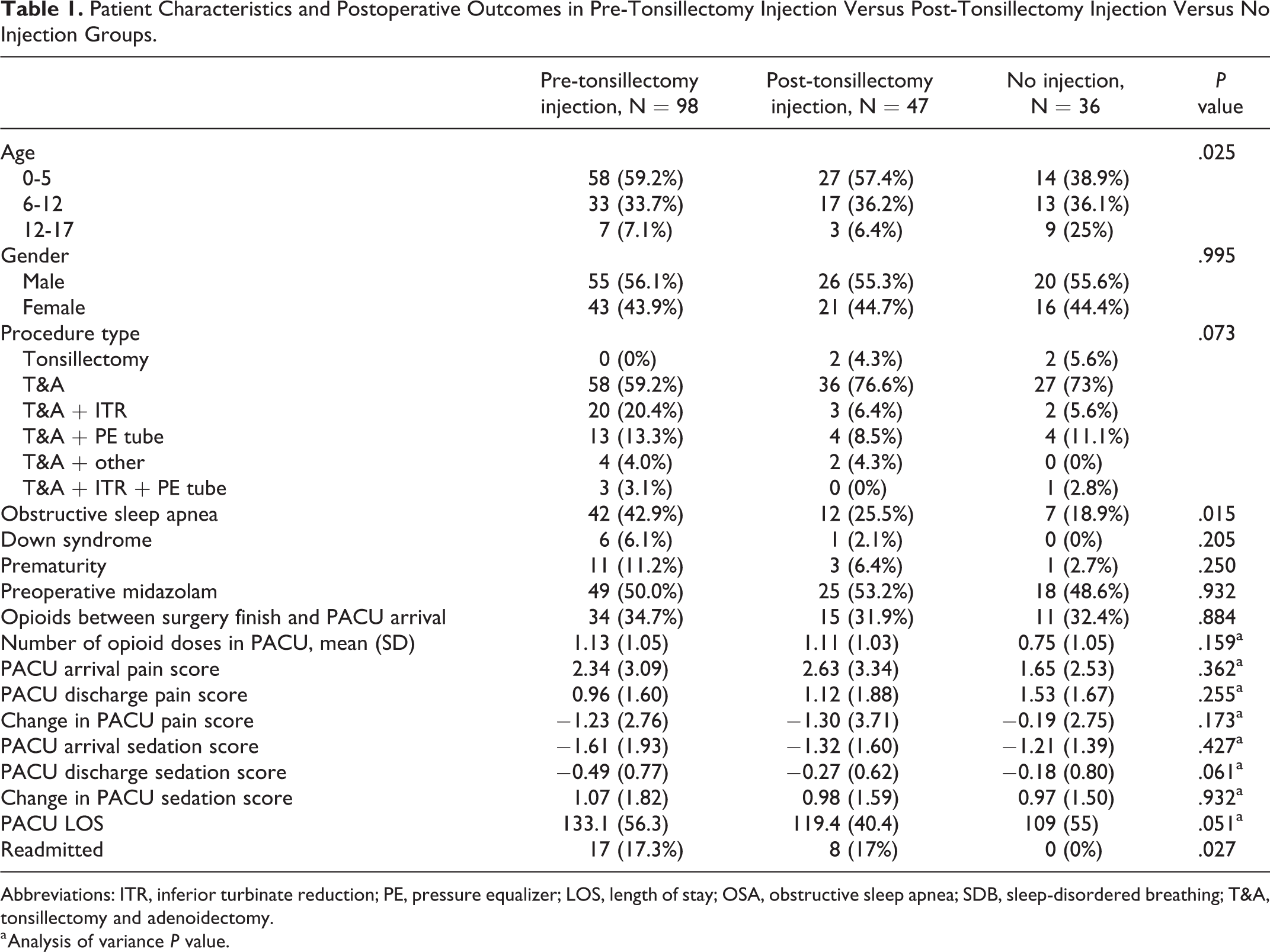
Abbreviations: ITR, inferior turbinate reduction; PE, pressure equalizer; LOS, length of stay; OSA, obstructive sleep apnea; SDB, sleep-disordered breathing; T&A, tonsillectomy and adenoidectomy.
a Analysis of variance P value.
The mean number of opioid doses received in the PACU, pain score at PACU arrival and discharge, change in pain score during PACU stay, sedation score at PACU discharge, change in sedation score during PACU stay, and length of PACU stay were not significantly different between the comparison groups. The pre-tonsillectomy injection group saw a slightly higher rate of readmissions at 17.3% versus 17% in the post-tonsillectomy injection group versus 0% in the no injection group (P = .027; Table 1). Reasons for readmission for pre-tonsillectomy patients were 7.1% dehydration, 9.2% pain, 3.1% bleeding, and 3.1% respiratory distress. Reasons for readmission for post-tonsillectomy patients were 4.3% dehydration, 8.5% pain, 4.3% bleeding, and 2.1% respiratory distress. Some patients were readmitted for multiple reasons. 19.2% of readmitted patients did so within 24 hours of discharge.
Subanalysis After Stratification by Age Group
Postoperative outcomes were analyzed after stratification into 3 age categories. Ninety-nine patients were between age 0 and 5, 63 were between age 6 and 12, and 19 were 12 to 17 years old. Among 0- to 5-year-olds, 48.3% of pre-tonsillectomy injection patients versus 29.6% of post-tonsillectomy injection patients versus 14.2% of no injection patients had OSA (P = .035). There were no differences in the number of opioid doses given between the 3 treatment groups aged 0 to 5 years (P = .609). Mean (SD) PACU discharge pain score was lowest in the pre-tonsillectomy injection group, with 0.55 (1.29) pre-tonsillectomy group versus 0.71 (1.37) post-tonsillectomy group versus 2 (1.63) no injection group (ANOVA P = .004). Length of stay in PACU was longest in 0- to 5-year-olds who received pre-tonsillectomy injection (150.1 [58.3] minutes) compared to those who received post-tonsillectomy injection (120.5 [47.2] minutes) or no injection (118.4 [56.3] minutes; ANOVA P = .035; Table 2).
Patient Characteristics and Postoperative Outcomes in Pre-Tonsillectomy Injection Versus Post-Tonsillectomy Injection Versus No Injection Groups After Stratification Into 3 Age Subgroups.
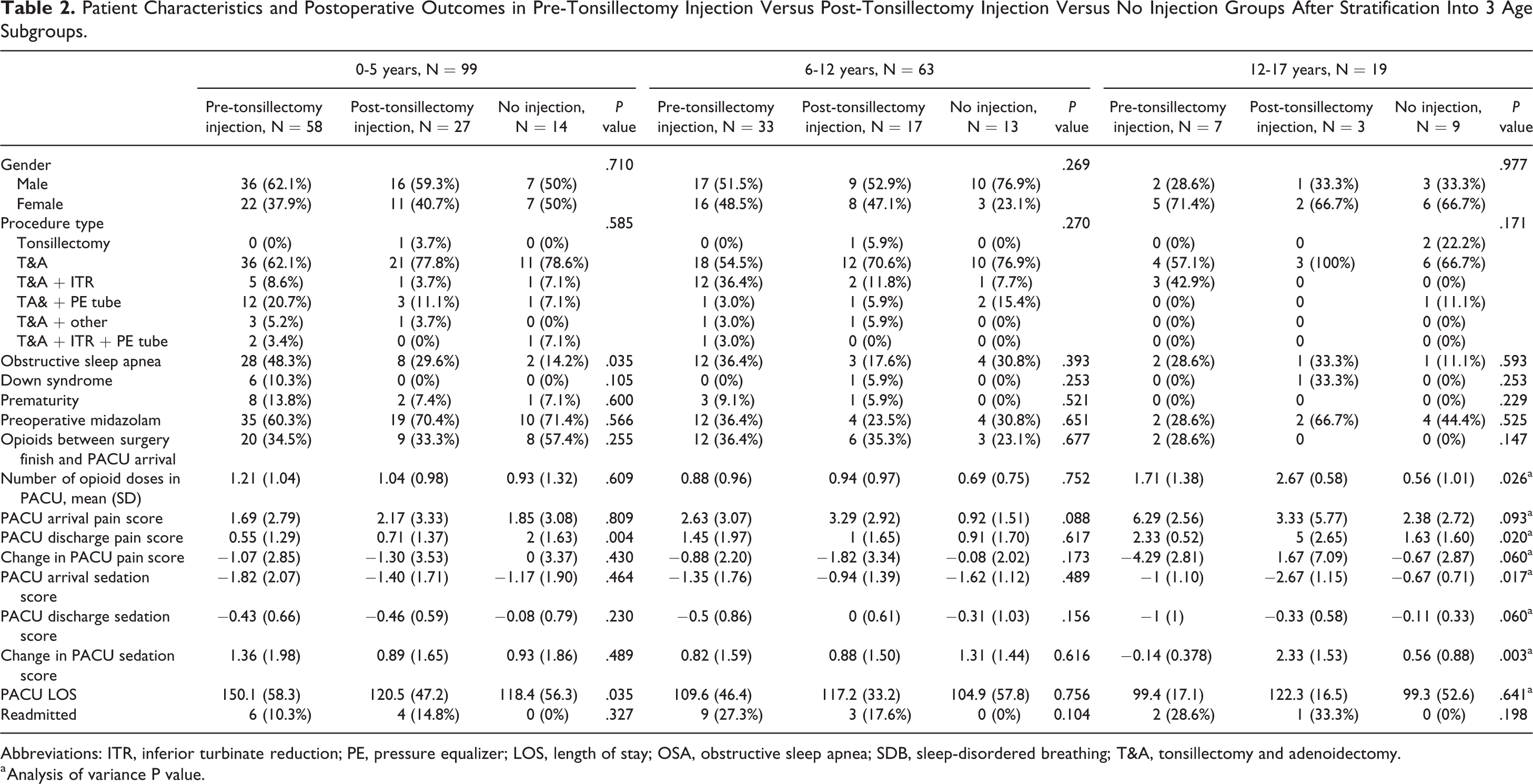
Abbreviations: ITR, inferior turbinate reduction; PE, pressure equalizer; LOS, length of stay; OSA, obstructive sleep apnea; SDB, sleep-disordered breathing; T&A, tonsillectomy and adenoidectomy.
a Analysis of variance P value.
There were no significant postoperative differences among the 3 treatment groups 6 to 12 years old. This included the mean number of opioid doses given (ANOVA P = .752), PACU arrival pain score (ANOVA P = .088), and discharge pain score (ANOVA P = .617; Table 2).
In the 12- to 17-year-old subgroup, the mean (SD) number of opioid doses received in the PACU was greatest in the post-tonsillectomy injection group at 2.67 (0.58) versus 1.71 (1.38) in the pre-tonsillectomy injection group versus 0.56 (1.01) in the no bupivacaine injection group (ANOVA P = .026). Pain score at PACU discharge was highest in the post-tonsillectomy injection group at 5 (2.65) versus 2.33 (0.52) in the pre-tonsillectomy injection group versus 1.63 (1.60) in the no injection group (P = .0196). Post-tonsillectomy patients (2.33 [1.53]) best recovered from their initial sedated states compared to pre-tonsillectomy bupivacaine (−0.14 [0.378]) and no bupivacaine (0.56 [0.88]) patients (P = .003; Table 2).
Sub-analysis After Stratification by Surgical Indication
Sixty-one patients had OSA only, 92 had SDB only, and 28 had neither OSA nor SDB. Among the 3 subgroups, there were no differences in the proportion of patients with Down syndrome. Among the OSA- and SDB-only subgroups, there were no differences in postoperative outcomes among pre-tonsillectomy versus post-tonsillectomy versus no injection patients. Among those without OSA or SDB, PACU mean (SD) length of stay was longest in the pre-tonsillectomy injection group at 130.5 (42.4) minutes versus 126.6 (40.3) minutes in the post-tonsillectomy injection group versus 75.7 (52.7) minutes in the no injection group (P = .028; Table 3).
Patient Characteristics and Perioperative Outcomes in Pre-Tonsillectomy Injection Versus Post-Tonsillectomy Injection Versus No Bupivacaine Injection Groups After Stratification Into Surgical Indication Subgroups.
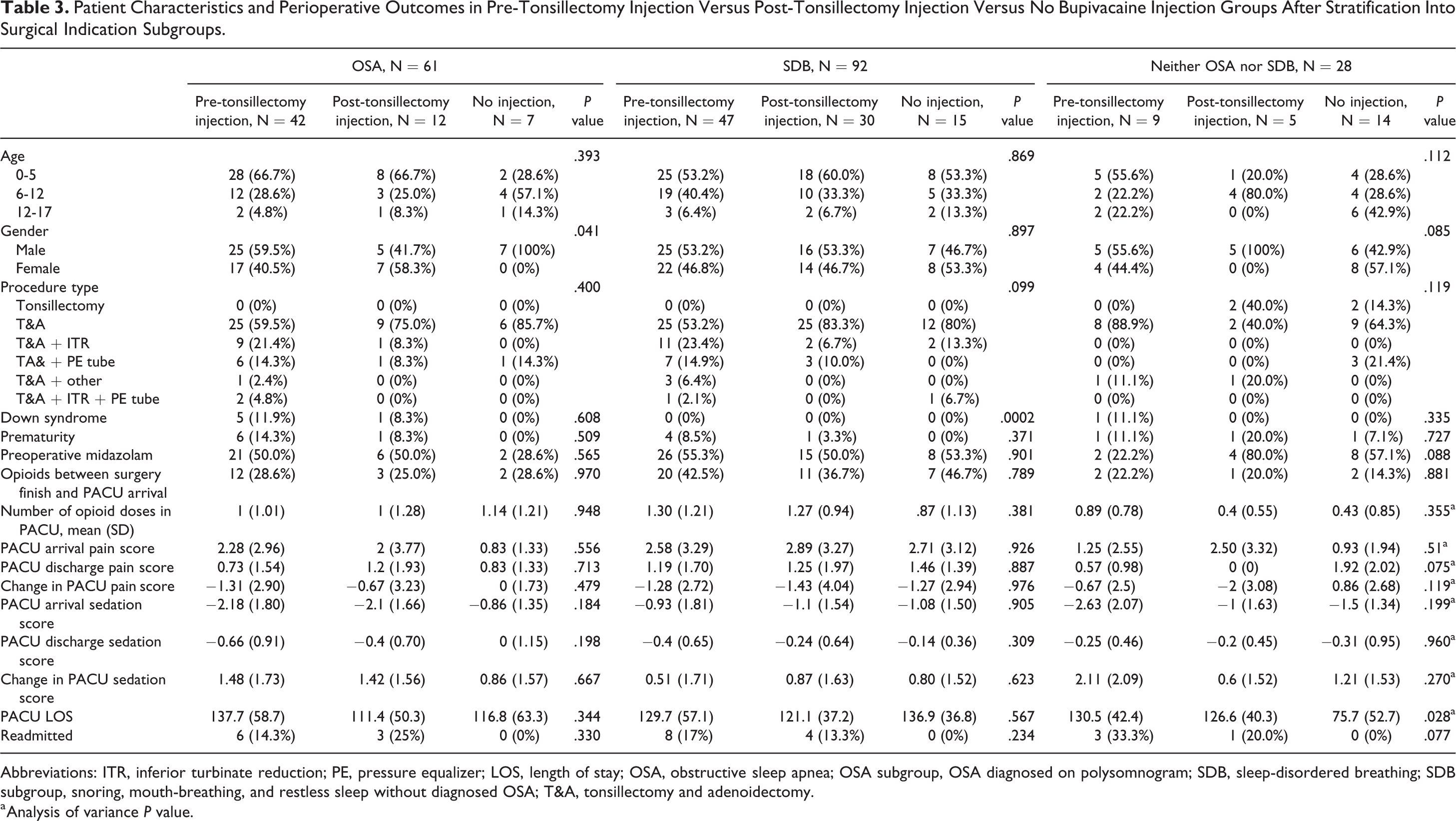
Abbreviations: ITR, inferior turbinate reduction; PE, pressure equalizer; LOS, length of stay; OSA, obstructive sleep apnea; OSA subgroup, OSA diagnosed on polysomnogram; SDB, sleep-disordered breathing; SDB subgroup, snoring, mouth-breathing, and restless sleep without diagnosed OSA; T&A, tonsillectomy and adenoidectomy.
a Analysis of variance P value.
Discussion
To our knowledge, this study is the first to evaluate the effect of intraoperative bupivacaine on pediatric patients after stratification into different age and surgical indication subgroups. Among 0- to 5-year-olds, pain level at discharge was highest in those who did not receive bupivacaine and lowest in those who received bupivacaine prior to resection. Among 12- to 17-year-olds, pain score at discharge was highest in those who received post-tonsillectomy injection. Surprisingly, among 0- to 5-year-olds and among those without OSA or SDB, patients who received pre-tonsillectomy bupivacaine experienced the longest PACU stays. Patients who received bupivacaine also saw higher rates of readmission, though most readmissions occurred more than 24 hours after discharge.
Though there is some controversy regarding the efficacy of intraoperative bupivacaine, most previous studies have demonstrated that bupivacaine infiltration reduces immediate postoperative pain in the pediatric adenotonsillectomy population.16,21-23 Our results, however, suggest bupivacaine infiltration or its timing may not be associated with postoperative pain control or opioid requirement for all pediatric populations. Notably, bupivacaine use was associated with greater length of stay in PACU and higher readmission rates overall. It is possible length of stay was confounded by availability of inpatient beds or by speed of the discharge process. Readmission trends seen in our study could be attributed to the pre-tonsillectomy and post-tonsillectomy injection groups consisting of a higher percentage of OSA and patients with Down syndrome. The majority of readmissions also occurred after 24 hours from reduced oral intake and pain. Since bupivacaine only lasts for several hours after injection, it is doubtful if it contributed significantly to differences in readmissions in our cohort.
Our findings are consistent with prior data demonstrating inverse relationship between half-life and age for bupivacaine. 24 Our youngest patients who received bupivacaine clearly saw a benefit in pain reduction. In contrast, teen-aged patients who received bupivacaine reported less favorable postoperative outcomes in terms of pain control and opioid use compared to those who did not. This may be related to local inflammatory response from the injection or the fact that these patients were experiencing dysphagia, which was perceived as pain. This finding in our teen-aged patients is in contrast to a study of 68 tonsillectomy patients between 8 and 65 years of age by Molliex et al, which reported that bupivacaine infiltration produces mild decrease in postoperative pain during the first 24 hours. Approximately one-third of the patients in this study were between 8 and 15 years of age. 25 Jebeles et al also found that pre-tonsillectomy bupivacaine injection leads to lower pain on the day of surgery in patients between 8 and 18 years of age. 16 Currently, there is a paucity of information in the literature regarding differences in pain thresholds in younger versus older children and this would be an area for further investigation.
Our findings demonstrate a lack of significant association between intraoperative bupivacaine and postoperative outcomes after stratification into OSA, SDB, or neither indication. In patients with OSA and SDB, opioid use is carefully titrated or even avoided due to the risk of apnea and desaturation. 26 Our results imply a lack of significant benefit from bupivacaine in patients with OSA or SDB and suggest against potentially unnecessary intraoperative intervention using the local anesthetic.
Of note, though nearly half of the tonsillectomies were performed using electrocautery and the other half using coblator, the 2 techniques have been shown to produce comparable postoperative pain and complication rates.27,28 Therefore, having mainly these 2 ablative techniques likely did not impact our findings. Furthermore, relatively few patients received acetaminophen before or after surgery, and intraoperative IV acetaminophen was given to a fairly uniform proportion of patients across all age and surgical indication subgroups. Therefore, delivery of acetaminophen likely did not impact the validity of our findings.
There are conflicting data on whether other local anesthetics positively contribute to pain outcomes in adenotonsillectomy. Local ropivacaine infiltration has been shown to have mixed effects on pain outcomes. Some studies have demonstrated improvement in postoperative pain control with ropivacaine with or without clonidine, whereas others have not.29,30 In fact, ropivacaine has even been shown to adversely affect neck pain scores and retching frequency compared with placebo. 31 A prospective study by Zhang et al 32 demonstrated reduced pain for patients receiving bupivacaine or lidocaine injections after tonsillectomy, compared to neither, though there was no significant difference in pain reduction between the local anesthetics. Again, no prospective study has explored the impact of timing of local anesthetic injection on pain outcomes, and variations in study outcomes warrant larger prospective cohort investigations with the above local anesthetics.
There are several limitations to this study. The first is the relatively small sample size of our cohort and the retrospective nature of this study. Larger studies—especially ones that stratify by pediatric age groups and surgical indications—could help validate our findings. The retrospective nature of our study does not allow for appreciation of unmeasured confounders and unobserved associations. A potential confounder of length of stay in the PACU is the availability of inpatient beds or speed of discharge processing. Lack of available bed space at time of PACU discharge or logistical challenges in discharge could have increased the recorded length of stay. Moreover, at the time of PACU arrival and discharge, there was variability in when pain and sedation scores were measured and the providers that measured them. Lastly, surgical technique could have impacted outcomes.
Conclusion
In conclusion, there were no overall differences in postoperative pain and sedation scores or amount of opioids received among patients who received intraoperative bupivacaine and those who did not. This study also indicates that intraoperative bupivacaine injection may be beneficial in younger children in the immediate perioperative period but may not be as useful in older children. A prospective study could help clarify whether there is benefit to administering intraoperative local anesthesia in tonsillectomy for different age groups.
Footnotes
Authors’ Note
This study was an oral presentation at AAO-HNSF New Orleans, LA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.