
Abstract
Stapediovestibular dislocation is a rare disorder as a result of traumatic injury to the structures in the middle ear. We described a case of a 60-year-old female with stapediovestibular dislocation with associated perilymph fistula. She presented with symptoms including hearing loss, vertigo, and tinnitus after a penetrating injury by an ear pick. After 4 months of conservative management, her symptoms failed to improve. Therefore, she underwent surgery which resolved completely her vestibular symptoms and her hearing loss had partially improved. The restoration of the stapes to its normal anatomical position coupled with ossiculoplasty and closure of the tympanic membrane are effective in patients with stapediovestibular dislocation.
Introduction
Injuries to the structures in the middle ear can be caused by either a direct or indirect traumatic force. Indirect traumatic force is usually associated with a blunt head injury that is frequently encountered in a motor vehicle accident. On the other hand, direct trauma is often caused by an ear pick or cotton through the external auditory canal. It has been reported that the most common cause of middle ear injury is head trauma, while only 3.1% are caused by direct ear trauma. 1 In China, an ear pick is made of metal, bamboo, or plastic, which is commonly used to clean the ear canal. This practice may result in injuries to the structures in the middle ear, including tympanic perforation, ossicular chain dislocation, stapes, or inner ear damage. The traumatic tympanic perforation represents the most common occurrence and is usually treated conservatively because such injury has a high rate of spontaneous healing. However, when an ossicular dislocation or perilymph fistula is suspected, immediate surgical intervention should be considered to prevent permanent sensorineural hearing loss. Stapediovestibular dislocation is an extremely rare type of auditory ossicular dislocation. A review of 166 cases of ossicular injuries reported in the literature has revealed only 5 cases of stapediovestibular dislocation, of which 3 were internal dislocations and 2 were external dislocations. 2 Given its rarity, the treatment for stapediovestibular dislocation remains controversial. Here, we described a case of an internal stapediovestibular dislocation with an intact stapes and perilymph leakage. The management of this disorder and its clinical outcome was discussed.
Case Report
A 60-year-old Chinese woman was accidentally hit by her grandson to the left ear while she was cleaning her ear with an ear pick. Following the trauma, she immediately experienced symptoms of tinnitus, hearing loss, and severe vertigo that could be exacerbated by loud noises. This had resulted in her difficulty with standing or walking. She was treated conservatively at the local hospital, which included high-dose intravenous corticosteroids and antibiotics. After 4 months of these treatments, her vertigo did not improve, while her tinnitus had deteriorated further. Therefore, she presented to our hospital to seek further treatment.
Upon admission to our department, a thorough endoscopic examination of the left ear was performed, which revealed an air-fluid level behind the intact tympanic membrane (Figure 1A). This finding suggested a possible perilymph fistula. Although the patient’s vertigo could be triggered by loud noises, nystagmus was not observed. A vestibular test was not performed to avoid further damage to the inner ear. The pure tone audiogram showed a severe, mixed pattern of hearing loss. The average hearing level of the left ear was 83.3 dB with 33.3 dB air-bone gaps (Figure 3A). The high-resolution computed tomography (CT) of the temporal bone demonstrated that the left stapes footplate had protruded into the vestibular cavity accompanied by an incudostapedial disarticulation (Figure 4).
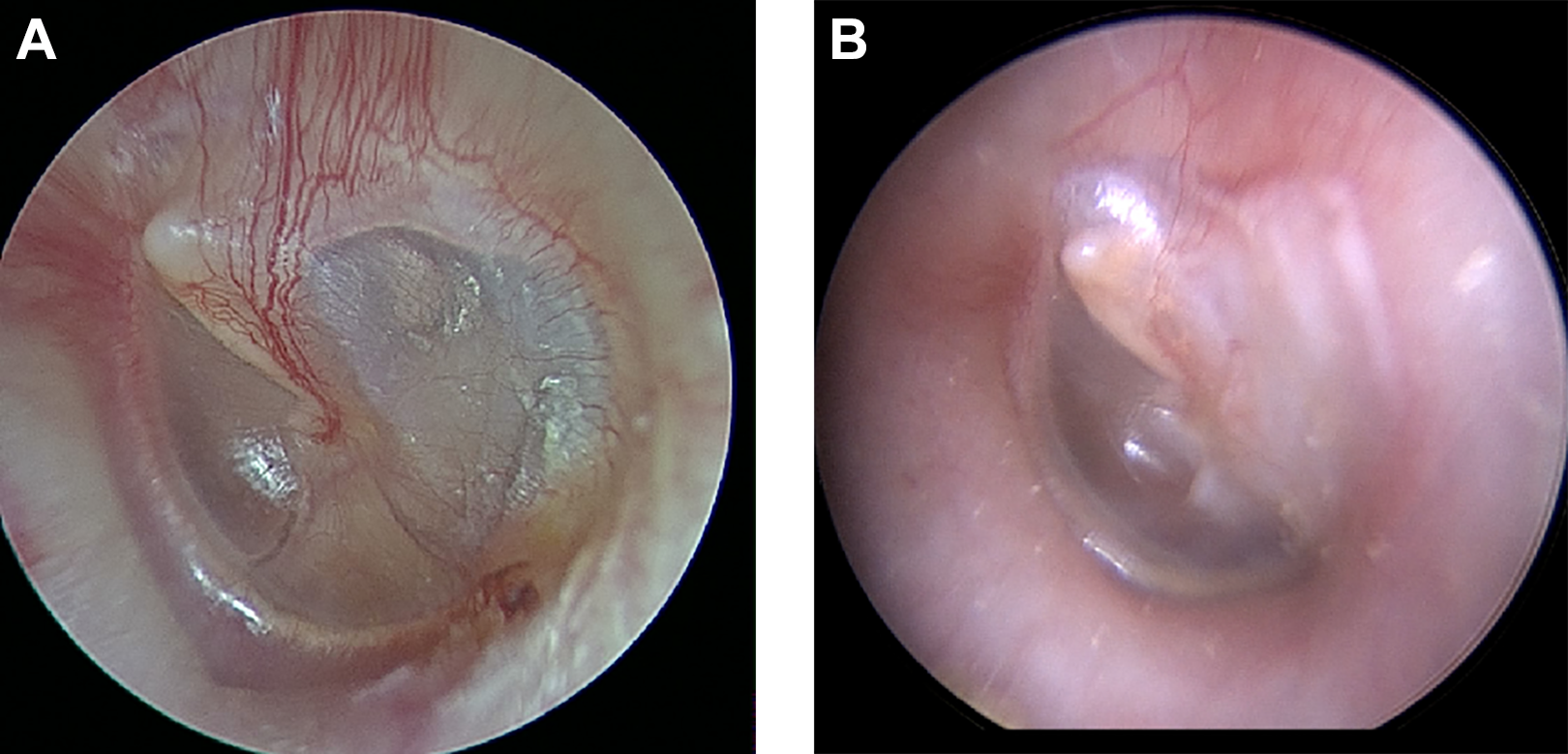
Pre (A)-and postoperative (B) otoscopic finding of the tympanic membrane. The arrows point the air-fluid level of the left ear.
Given the clinical findings and the patient’s persisted symptoms, surgery was performed under the general anesthesia with a 0°, 3-mm-diameter endoscope through the external auditory canal. The tympanomeatal flap was elevated and translocated anteriorly. Then, the middle ear cavity was explored, which confirmed the presence of an incudostapedial joint disarticulation as shown on the CT. There was a ruptured stapes tendon with the stapes footplate protruded into the vestibular cavity (Figure 2A) through the oval window, where a perilymph leakage was evident. Following the removal of the stapes from the vestibular cavity (Figure 2B), a perichondrium graft was placed on the oval window and the stapes was then replaced in the repaired oval window (Figure 2C). Next, the incudostapedial joint was fixed with fibrin glue. Finally, the tympanic membrane was enforced by tragus cartilage and perichondrium. Postoperatively, the patient’s dizziness had resolved. At the 5-month follow-up, her hearing level had improved to 66.7 dB with the closure of the air-bone gap within 10 decibels (Figure 3C). The otoscopic examination of the tympanic membrane of the left ear showed a well-healed incision (Figure 1B). The patient’s subjective speech recognition had improved, but the speech discrimination score was not measured because this assessment was not carried out in our hospital.
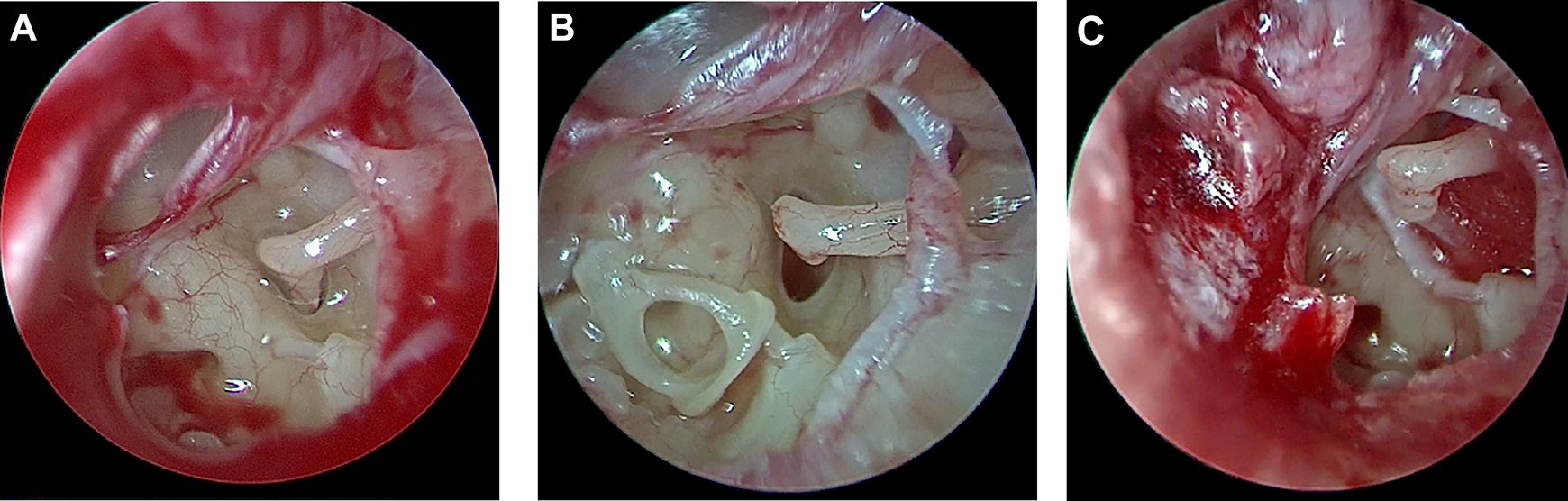
Photographs of middle ear intraoperatively. (A)The stapes footplate depressed into the vestibule window. (B)The intact stapes moved from the vestibule window. (C)The reconstruction of incudostapedial joint.
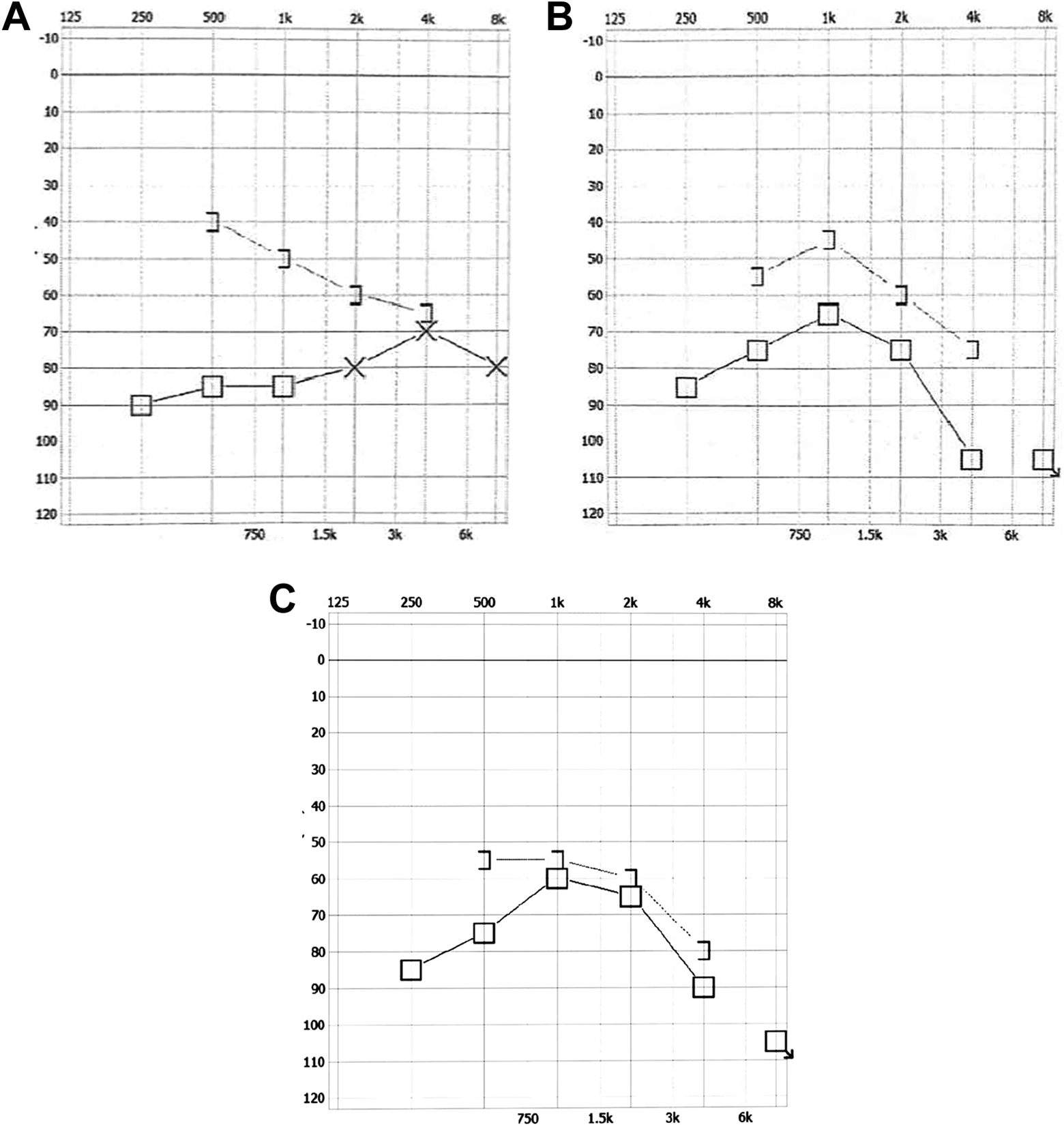
Preoperative (A), one-month postoperative (B) and five-month postoperative (C) audiometric evaluation of left ear.
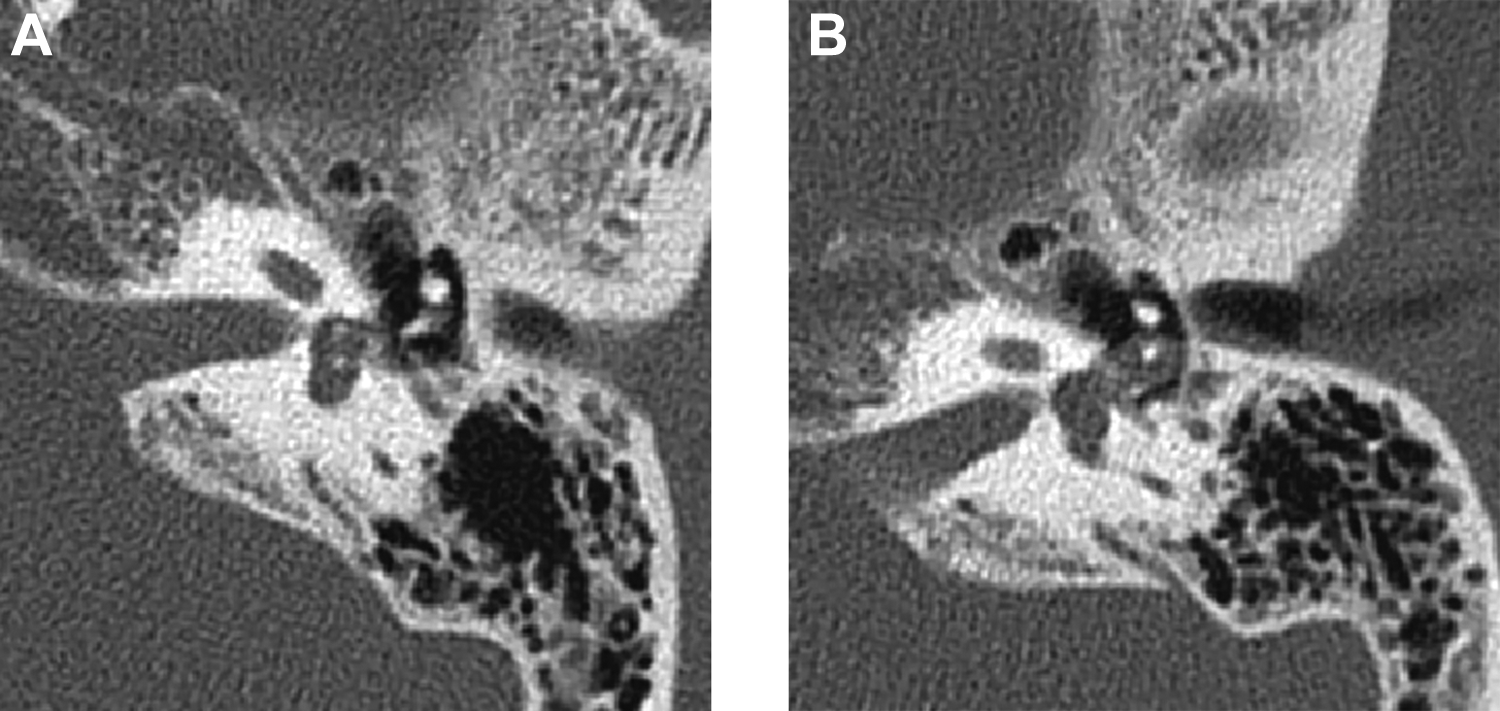
Pre (A)-and postoperative (B) CT scans. (A)The arrow point the stapes depressed into the vestibule. (B)The arrow point the stapes in right position.
Discussion
Traumatic luxation of the stapes was first reported in 1970.3,4 However, the incidence of internal stapediovestibular dislocation without a stapes fracture is rare. Over the years, cases of stapediovestibular dislocation with intact stapes have been reported from all over the world,5-14 as summarized in Table 1.
Stapediovestibular Internal Dislocation With Intact Stapes.
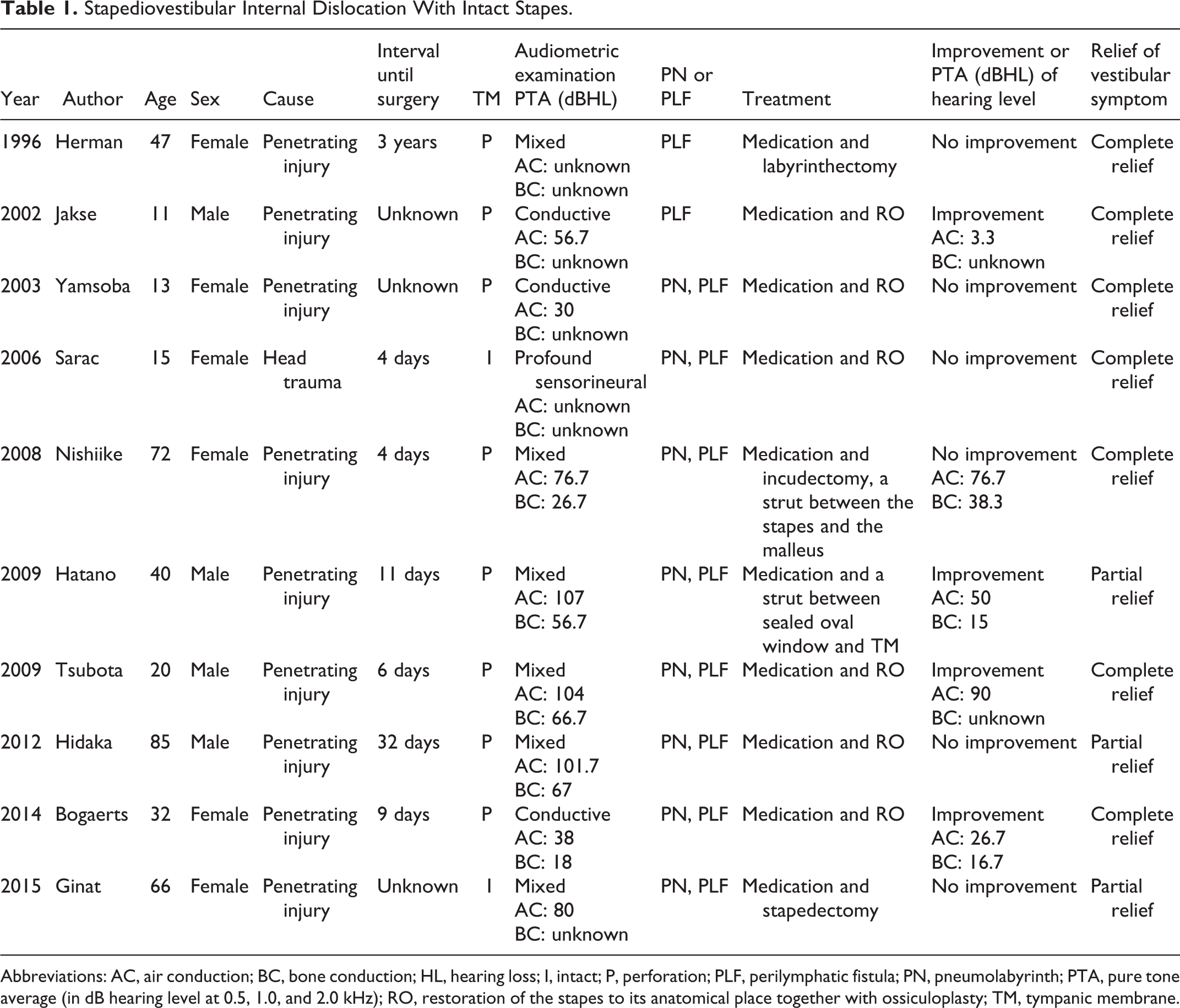
Abbreviations: AC, air conduction; BC, bone conduction; HL, hearing loss; I, intact; P, perforation; PLF, perilymphatic fistula; PN, pneumolabyrinth; PTA, pure tone average (in dB hearing level at 0.5, 1.0, and 2.0 kHz); RO, restoration of the stapes to its anatomical place together with ossiculoplasty; TM, tympanic membrane.
In most cases, several causes of penetrating injury have been described, such as the ear picks,7,10,11 cotton tip applicators, 5 and chopsticks, 12 while a few cases were attributed to head trauma. 8 Symptomatically, most patients suffer a hearing loss as well as vestibular symptoms such as dizziness, nausea, and vomiting. Otoscopic examination often reveals a perforated tympanic membrane, while an intact tympanic membrane is uncommon. Preoperative pure tone audiometry shows a conductive, sensorineural, or mixed deafness, and the CT examination shows features of stapediovestibular luxation or subluxation accompanied by pneumolabyrinth. The interval from injury to surgical treatment has been reported to be within a month, but in our case, it was 4 months. Despite the delay in surgical intervention, our patient not only had retained her residual hearing but also achieved a complete resolution of her vestibular symptoms such as vertigo after surgery, which is extremely rare.
Most patients choose to have conservative treatment after an injury but eventually proceed to surgical treatment when the vestibular symptoms persist. The pneumolabyrinth is considered an important cause of vestibular symptoms. Nearly all patients with stapediovestibular dislocation would have pneumolabyrinth soon after injury. However, the temporal bone CT may show no evidence of pneumolabyrinth after a period of months or years following the injury, suggesting that the pneumolabyrinth resolves spontaneously over time.
The options of surgical procedure will depend on the degrees of hearing loss. For patients who have irreversible total or complete deafness, the main procedure of choice is labyrinthectomy. 5 If the patient still has some residual hearing, auditory chain reconstruction and tympanoplasty are usually performed.6-8 Several methods and materials of reconstruction can be employed, such as the temporal myofascial flap or perichondrium, artificial auditory ostium, and autogenous columellar cartilage. 10
Conclusion
Ossicular chain injury should be suspected in patients with a history of penetrating trauma to the external auditory canal and presenting with symptoms of persisted hearing loss, dizziness, and vomiting. The high-resolution CT of temporal bone often provides valuable information in delineating the extent of the injury. Conservative treatment does not resolve vestibular symptoms, which leads to poor quality of life. Although immediate surgical intervention is controversial, it may be better to remove the stapes from the vestibular as soon as possible when the stapes has deeply depressed into the vestibule.
Supplemental Material
sj-tif-1-ear-10.1177_0145561320968925 – Supplemental Material for Traumatic Stapediovestibular Dislocation With Intact Stapes: Report and Review
Supplemental Material, sj-tif-1-ear-10.1177_0145561320968925 for Traumatic Stapediovestibular Dislocation With Intact Stapes: Report and Review by Qinzhan Ren, Jinfei Su, Jinyuan Si, Yue Li and Xiuyong Ding in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.