
Abstract

A 21-year-old male was referred to the otolaryngology clinic for a 3 month history of a facial mass. The area of concern originally appeared as an erythematous skin nodule located along the inferolateral aspect of the body of the right mandible, closely resembling an ingrown hair. Upon presentation, however, the mass had steadily grown in size, measuring 4.0 cm. It was well-circumscribed, firm, and adherent to the overlying discolored skin, but mobile relative to the underlying mandible. The patient denied recent fevers, infection, trismus, or lockjaw, and the rest of his head and neck examination was unremarkable.
Importantly, the patient was diagnosed a year prior with a large high grade (grade 3) malignant peripheral nerve sheath tumor (MPNST), a variant of a soft tissue sarcoma, of the right shoulder and flank. Preoperative positron emission tomography (PET) and chest computed tomography (CT) at diagnosis revealed the patient was free of metastatic disease. He initially underwent wide local excision of the 8.5 × 8.0 × 6.0 cm mass. Pathology demonstrated negative margins of resection and a proliferative index of 10% to 15%. The patient subsequently received a total of 6000 cGy of adjuvant radiation therapy. Routine surveillance chest CT scans revealed no evidence of local recurrence or metastatic disease 9 months post-diagnosis.
In light of the patient’s history, a comprehensive workup of the mass was initiated. Fine needle aspiration of the mass was inconclusive. Ultrasound of the area showed a hypervascular soft tissue nodule overlying the right mandible, and a subsequent soft tissue contrast-enhanced CT of the neck demonstrated an intact right hemi-mandible with an overlying subcutaneous mass (Figure 1). Core biopsy revealed a MPNST consistent with metastasis from the patient’s primary tumor. The mass was metabolically active on PET, however, no evidence of disease activity was found elsewhere.
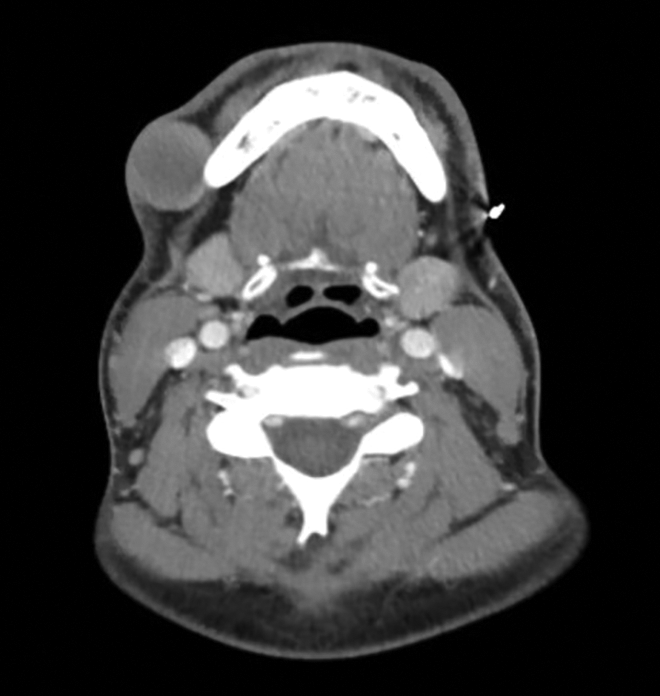
Contrast-enhanced CT soft tissue of the neck shows an intact right hemi-mandible with an overlying well-circumscribed subcutaneous mass. CT indicates computed tomography.
Thirteen months following the resection of his primary tumor, the patient underwent surgical excision of the subcutaneous facial mass. The tumor was entirely superficial to the platysma with no involvement of the facial nerve. The involved skin was excised and the defect was closed primarily by mobilization of the adjacent skin flaps. Histologic evaluation of the mass revealed a 3.9 × 2.7 × 2.6 cm firm, tan, and rubbery lesion with pathology similar to the patient’s previously resected tumor, but with a heightened proliferative index of 30% to 40% and a mitotic index of 20%. The tumor was S-100 positive. Margins of resection were close, but negative. Representative photomicrographs of the metastatic tumor are shown in Figure 2. The patient received adjuvant radiotherapy to the site.
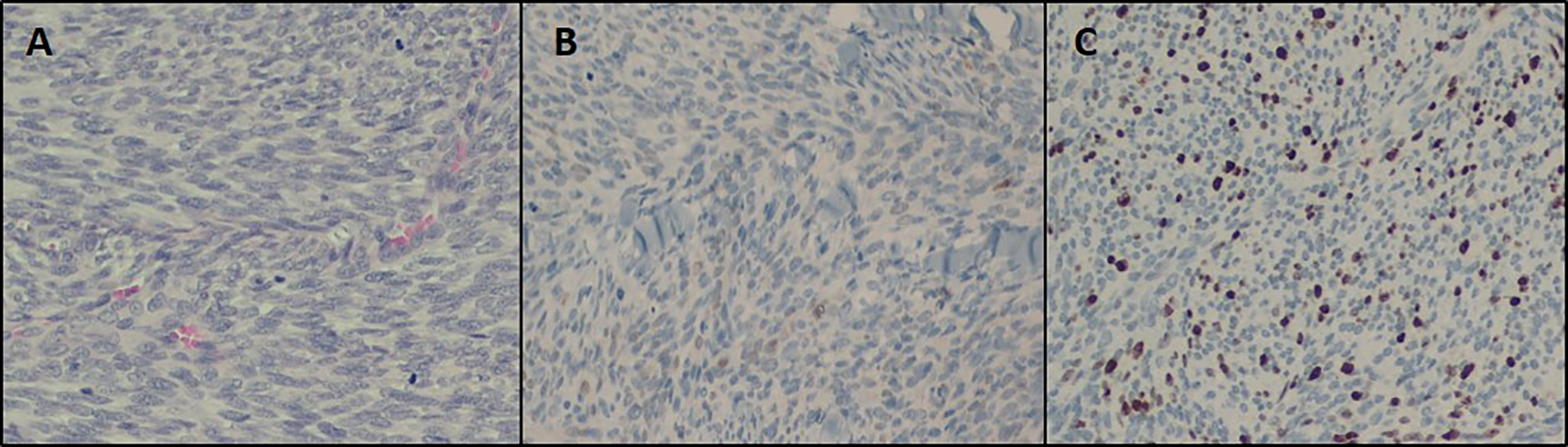
A, The hematoxylin and eosin stained section shows the spindle cell morphology of MPNST with abundant mitosis (×200 magnification). B, Immunohistochemical stains for S-100 show focal positivity (×200 magnification). C, Immunohistochemical stains for MIB-1, a marker of cellular proliferation, demonstrate mitotic index of 20% (×200 magnification). MPNST indicates malignant peripheral nerve sheath tumor.
In this report, we document a case of distant metastasis of a MPNST to the skin and subcutaneous soft tissues of the face. While up to 22.6% of patients with MPNST may have primary tumors of the head and neck, a review of the literature revealed no other reports of a nonhead and neck primary MPNST metastasizing to the region as described here.1,2 In fact, among all types of soft tissue sarcoma, there is just one other documented case of distant metastasis to the head and neck region; a case of metastasis to the tongue that was previously reported in a 41-year-old male with high grade myxofibrosarcoma of the thigh. 3
Malignant peripheral nerve sheath tumors are the sixth most common type of soft tissue sarcoma. 4 Between 30% to 60% of MPNST patients develop metastases, with risk factors including increased primary tumor size (> 10 cm) and tumors American Joint Committee on Cancer stage III or greater. 4 The most common site of metastasis is to the lungs (65%). Less common sites of metastasis include the liver, brain, bones, and adrenal glands. 4 There have been reports of soft tissue sarcomas metastasizing to distant subcutaneous tissue, regional lymph nodes, and the peritoneum. 5
Surgical resection and radiation is the mainstay of treatment for localized high-grade MPNST. 4 For patients with metastatic disease, or unresectable tumors, combination chemotherapy involving ifosfamide and doxorubicin is sometimes initiated, as well. The 2 drugs have been shown to improve progression-free survival, but not overall survival. 6 Overall, the prognosis of MPNST is guarded, with a reported 5 year survival of 20% to 50%. 4 Given this prognosis, otolaryngologists should have a high index of suspicion for an otherwise unexplained mass present in the head and neck region of a patient with a history of MPNST, other soft-tissue sarcoma, or any malignancy, in general.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.