
Abstract
Purpose:
This study aimed to compare the intraoperative frozen section with the surgical margin in the postoperative surgical margins of the postoperative pathology of oral squamous cell carcinomas in order to examine the reliability of the frozen section.
Methods:
A retrospective analysis was conducted for patients who underwent surgery for oral squamous cell carcinoma in a tertiary hospital between January 2018 and 2019. The intraoperative frozen section examinations, grade of the tumor, number of lymph nodes, number of affected lymph nodes, depth of invasion, perineural invasion, lymphovascular invasion, and extranodal extension were recorded from the pathological records. The concordance between the frozen section examination and postoperative pathology 2 methods was examined using the Cronbach α coefficient. Sensitivity, specificity, positive predictive value, negative predictive value regarding surgical margins, and accuracy were calculated and reported.
Results:
Overall, 181patients who underwent surgery for oral cavity cancers were included; 118 (65.2%) were males. The mean (± standard deviation) age of the included participants was 57.4 ± 16.1 years. The most common tumour subsite was the tongue (n = 71, 39.2%). There was concordancy between the frozen, positive intraoperative malignancy and the postoperative pathology malignancy. The frozen, negative intraoperative malignancy and postoperative safe surgical margin did not significantly differ.
Conclusion:
As a result of intraoperative frozen examination, we found conformity between the postoperative pathology results of patients with positive and negative surgical margins. Frozen section examination could be used safely to examine intraoperative surgical margins of oral squamous cell carcinoma.
Introduction
Oral cavity cancer is one of the most common types of head and neck cancer globally. Due to the complexity of the anatomy of the oral cavity, it is difficult for surgeon to remove tumors with clear margins during oncological surgery. 1 Tumor positivity at the surgical margin causes locoregional recurrence of oral cavity cancers. 1 Therefore, it is very important that there are no tumors in the surgical margins. Although there is not a sufficient definition for safe surgical margins, frozen section biopsies indicate that 90% of surgeons have accomplished surgery with clear margins. 2 Although the frozen result are often reported as negative, there may be a positive surgical margin in the postoperative pathology. Due to time limitations, not all 3-dimensional boundaries are examined; additionally, due to technical reasons, such as crystal formation and melting of ice, 3 the quality is lower than that for paraffin sections. As a result of these limitations, negative examination of the frozen sections of oral squamous cell carcinoma may not always indicate that the surgical boundaries are negative. The definition of a safe surgical margin in oral cavity cancers and how it should be frozen with a technique is still controversial. 2 This study aimed to define safety surgical margins, to compare the intraoperative frozen sections with the surgical margin in the postoperative main specimen pathology in patients who undergone surgery for oral cavity squamous cell carcinoma.
Methods
Study Design and Patients
This was a retrospective study of 181 patients who were diagnosed with oral squamous cell carcinoma between January 2018 and January 2019 at our tertiary center. Patients were included if they had a diagnosis of primary oral cavity squamous cell carcinoma. Patients were excluded if they did not have squamous cell carcinoma as a result of pathology findings; had undergone surgery or prior radiotherapy; did not have detailed pathological information available in their files.
Procedures
The tumor was excised with a 5 mm safe surgical margin in all patients. All surfaces of the surgical specimen were marked with sutures to orient the pathologist. The specimens that the pathologist was unable to orient were identified by the primary surgeon and brought to the pathologist’s attention. Frozen sections were always taken from the area after tumor excision from both margins as a routine procedure for the specimen-driven approach. Rapid hematoxylin and eosin was used for intraoperative frozen section examination (2 or 3 slices from each sample). Dysplasia or cancer were considered positive and a surgical enlargement was performed and frozen sections repeated until a negative result for dysplasia or cancer was obtained. The surgeon did not close the defect until all samples were negative. Number of frozen sections were classified into 2 groups: 1 to 5 and greater than 5. Disease-free survival was defined as time from the date to surgery to local recurrence of tumor at the same site as the previous cancer.
Outcome Measures
TNM stage was assigned according to the current American Joint Commission on Cancer Staging Manual (8th edition). Demographic and clinicopathologic features of patients, intraoperative frozen section examinations, the grade of the tumor, number of lymph nodes, number of affected lymph nodes, depth of invasion (DOI), perineural invasion, lymphovascular invasion, extranodal extension, and worst pattern of invasion (WPOI) were recorded from the pathological records. The findings from the frozen sections performed and assessed by a pathologist during surgery and from the postoperative routine histopathological examination of the same sections were compared.
Statistical Analysis
Descriptive statistics (mean, standard deviation [SD], minimum, median, maximum) were used to describe continuous variables. The concordance between the frozen section examination and postoperative pathology 2 methods was examined using the Cronbach α coefficient. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) regarding surgical margins and accuracy were calculated and reported with a confidence interval of 95%. Values of P less than .05 were considered statistically significant. All analyses were performed using MedCalc Statistical Software version 12.7.7 (MedCalc Software bvba; http://www.medcalc.org; 2013).
Ethics
This study was approved by the Ethics Committee of the University Faculty of Medicine with the number of 514. Written informed consent was obtained from all patients included in the study.
Results
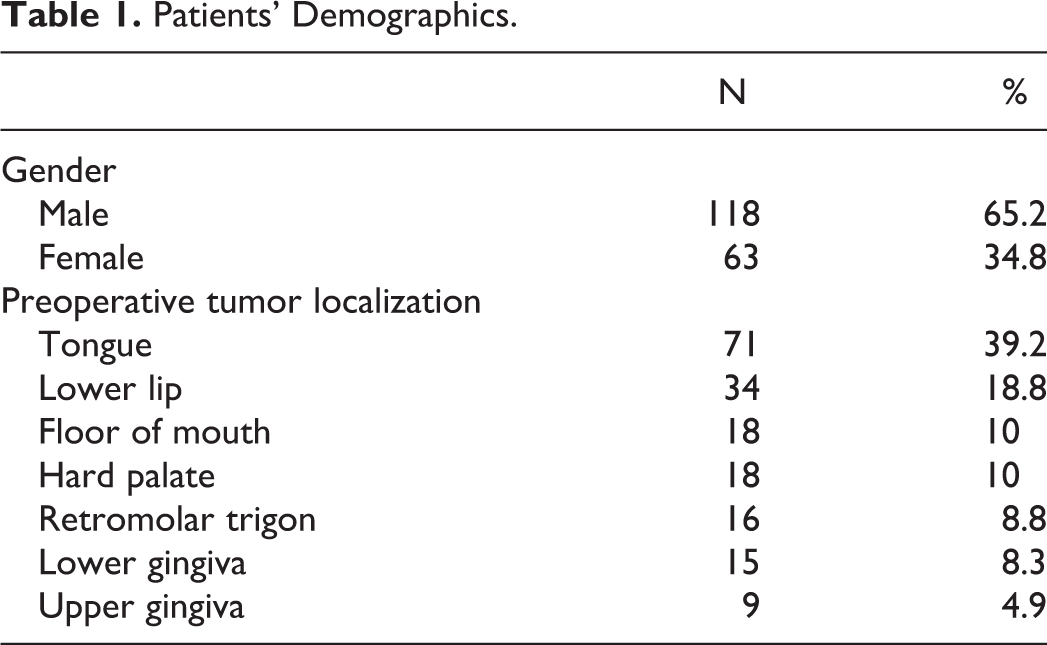
Overall, 181 patients who underwent surgery for oral cavity cancers were included; 118 (65.2%) were males, 63 (34.8%) females, and the mean (±SD) age was 57.4 ± 16.1years. The most common tumour subsite was the tongue (n = 71, 39.2%), followed by the lower lip (n = 34, 18.8%), the floor of the mouth (n = 18, 10%), the hard palate (n = 18, 10%), the retromolar trigon (n = 16, 8.8%), the lower gingiva (n = 15, 8.3%), and the upper gingiva (n = 9, 4.9%; Table 1). The mean (±SD) number of lymph nodes examined and affected lymph nodes were 27.8 ± 22.4 and 3.0 ± 2.2, respectively. The mean (±SD) DOI was 11.9 ± 8.5 (range 1-40) mm. Overall, 50 (27.6%), 72 (39.8%), 22 (12.2%), and 37 (20.4%) patients had grades of 1, 2, 3, and 4, respectively. Perineural invasion, lymphovascular invasion, and WPOI were observed in 88 (48.6%), 43 (23.8%), and 11 (6.1%) patients, respectively. Finally, extranodal extension was positive in 41 (22.7%) patients.
Patients’ Demographics.
While the Cronbach α coefficient for the frozen section examination and postoperative pathology was found 0.897 among all patients, it was 0.923 and 0.847 for those with 1 to 5 and greater than 5 frozen sections, respectively. Although high compliance was observed in all 2 groups, the compliance was slightly higher in those with 1 to 5 frozen sections (Table 2). Cronbach α coefficient was 0.95 for the intraoperative-postoperative negative numbers among all patients; however, according to groups, it was 0.988 and 0.934 for those with 1 to 5 and greater than 5 frozen sections, respectively (Table 2).
Comparison of Malignancy (−) and (+) Frozen Section Examination With Postoperative Pathology.
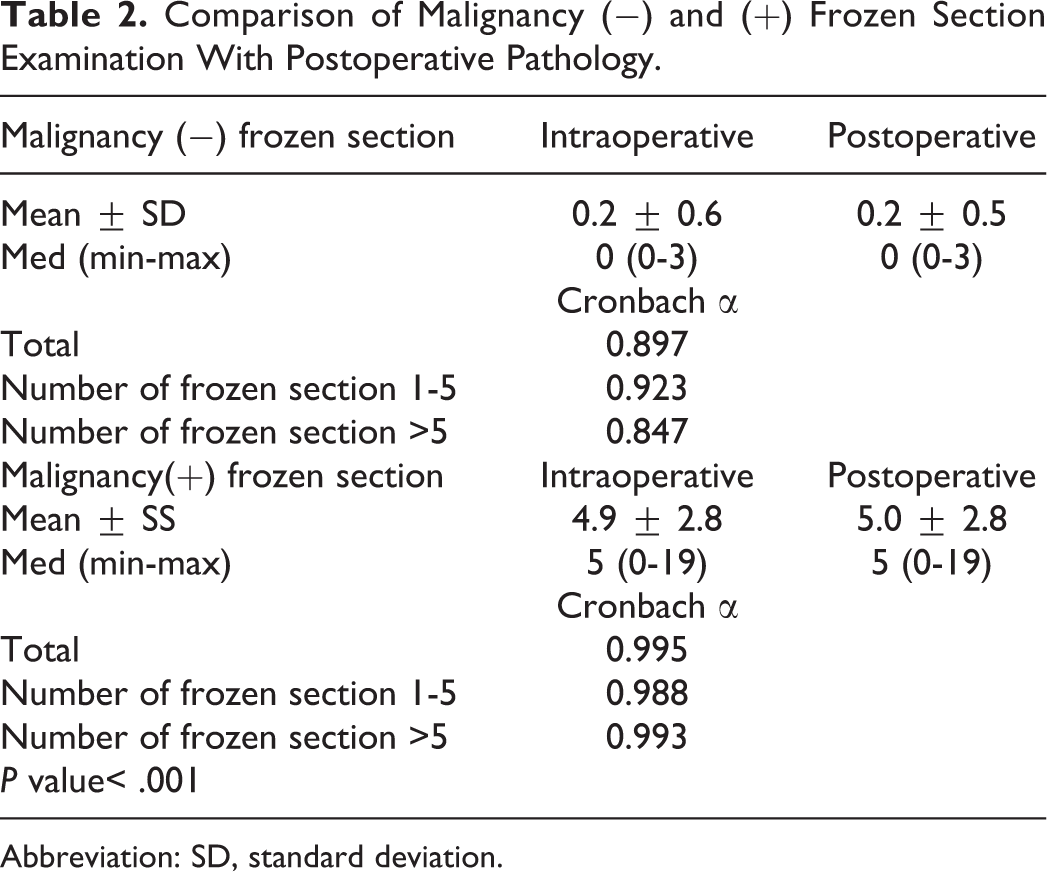
Abbreviation: SD, standard deviation.
Discordances were identified in 6 (3.1%) patients. There were 3 false negative results among the 6 patients who were determined to have a positive result following permanent pathology examination. While this discrepancy was due to a sample error in 2 patients, in the other patient it was due to an interpretation error upon investigation of the permanent sections. Although the frozen sections were reported as malignancies in 2 (1.1%) patients, the malignancies were reported as negative in the permanent pathology.
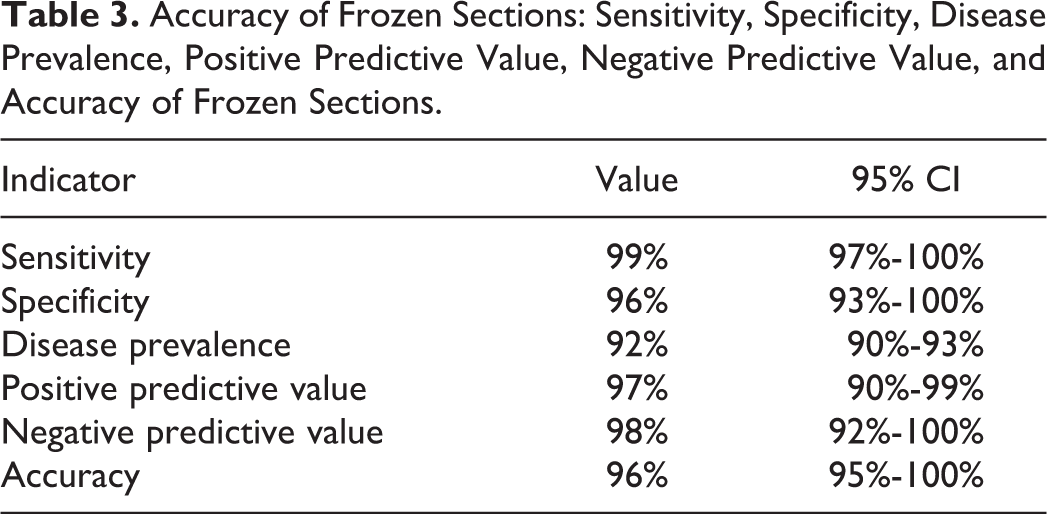
A secondary review of these cases showed that the frozen section was false positive in 1 patient and false negative in 1 patient. The sensitivity and specificity and accuracy of the frozen section evaluation were 99%, 96%, and 96% respectively. The PPV of a positive frozen section at diagnosis was 93.30%, while the NPV of negative frozen section was 97.60% (Table 3). None of the patient experienced a local relapse.
Accuracy of Frozen Sections: Sensitivity, Specificity, Disease Prevalence, Positive Predictive Value, Negative Predictive Value, and Accuracy of Frozen Sections.
Discussion
It is very important to achieve clean surgical margins in cancer surgery. Even if surgeons remove the tumor macroscopically, their aim is to confirm a negative microscopic surgical margin. Frozen section examination is the most common technique that is used clinically to assess surgical margins. 4 In addition to time and staff occupation, increased cost due to over-sampling and increased surgical time, Mannelli et al reported that they might miss the positive surgical margin. 4 However, in our study, the results for both positive and negative frozen examination of surgical margins were found to be compatible with the postoperative pathology. Due et al reported that 2% to 10% of frozen results, which were defined as negative based on the intraoperative findings, could be positively detected in the postoperative pathology. 5 In our study, it was observed that there was a high agreement between frozen investigations that were reported as negative based on the intraoperative findings and the exact pathology, thus confirming that our findings are consistent with those reported in the recent literature.6,7
We found that as long as the number of frozen examinations increased, the accordance also increased. Due et al suggested that sampling from the surgical bed should be better defined for intraoperative frozen examination. 5 Although this is an option, as the number of frozen examinations increases, the rate at which the pathologist misdiagnoses samples will decrease. Although increasing the number of frozen sections has disadvantages such as increasing the duration of surgery and increasing the cost of frozen examination, these disadvantages are not outweighed when considering postoperative surgical margin positivity and retreatment. We identified that the sensitivity and specificity of the frozen section evaluations were 99% and 96%, respectively. While these results are compatible with some of those previously published,6,8 they are very optimistic compared to other studies.5,9
Our findings might be impacted by the sampling method used, including where the samples were taken from; this is an important factor that affects frozen results. There are 3 accepted sampling techniques: specimen-driven, tumor-bed, or a combination of both of these approaches. 4 The specimen-driven approach increases the surgical defect and indicates that the resection is complete if the frozen result is negative compared to the specimen technique. 6 However, this technique causes false results as the surgeon obtains the frozen sections from the deeper side of the tumor bed. 10 This illusion is due to the withdrawal of the retraction of the deep soft tissue, especially in cases where the defect is large, such as in T2-4 oral squamous cell carcinoma. Recent studies emphasize the superiority of the specimen- driven technique compared to the tumor bed technique.9,11 We used the specimen-driven approach and thus believe that this had an impact on the high level of compliance.
Frozen section examination is a very frequently used technique but fluorescence-guided optical imaging spectroscopy or Raman spectroscopy, narrow band imaging, and optical coherence tomography are new techniques that are used for intraoperative frozen examination of surgical margins. 4 Although each of these techniques have their own characteristics, their superiority in examining whether there is a tumor at the surgical margin is still not understood. 4
Regardless of the technique used, one of the most challenging factor in frozen examination is that the optimum distance for clean surgical margins is not clearly defined. 12 A recent study emphasizes that concerns about frozen examinations are actually due to the lack of identification of safe surgical margins. 10 The shrinkage of biopsies taken from oral cavity contributes to this uncertainty. 10 Szewczyk et al approached the frozen examination from a different perspective. They reported that the positive surgical margin is a factor that indicates the aggressive course of the tumor in the biopsies sent by the surgeon from the surgical bed (even if the definitive pathology after the excision is negative) and this condition should be taken into consideration while providing adjuvant therapy. 13 Although this result may seem surprising, it suggests that the specimen-driven approach is more accurate than the tumor-bed approach.
However, none of the patient experienced a local relapse, the follow-up is too short. It was a limitation of this study. Apart from this, the present study has a number of limitations. It was a retrospective study, managed at a single institution. It will be more beneficial to evaluate frozen results with the participation of different surgeons and pathologists in multiple centers. Pathologies of patients who have received radiotherapy and had surgery before have not been studied in the study. Both preoperative radiotherapy and surgery increase fibrosis and make it difficult to define safe surgical margins.
Conclusion
In oral squamous cell carcinomas, it is difficult to exclude the tumor with a safe surgical margin. Frozen examination, which is used to make sure the surgical margin, is an extremely reliable method. Specimen-driven method should be used for frozen examination. As long as the number of frozen examinations increased, the accordance also increased. Future studies involving more centers, which take into consideration effect of frozen section examination on survival, should be conducted.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.