
Abstract
An 86-year-old female with a past medical history notable for chronic obstructive pulmonary disease, hypertension, atrial fibrillation, and cardiac stent was walking when she missed 2 steps on a staircase and fell forward, hitting her head on a marble wall with loss of consciousness. When she regained consciousness, she was temporarily aphonic, regaining a hoarse voice after 10 minutes. The patient was taken to the emergency department for severe neck pain.
On arrival, the patient endorsed difficulty swallowing, hoarseness, and continued neck pain. She expressed concerns regarding choking and coughing when trying to swallow her own secretions. The patient had no prior history of falls and her only prior head and neck surgery was a tonsillectomy.
Computerized tomography (CT) was ordered and revealed a 4-part Jefferson burst fracture with a 9.6 mm combined C1 lateral displacement on C2 indicating a tear of the transverse ligament (Figure 1). The C1 posterior arch fractures were immediately adjacent to the vertebral arteries and a vertical fracture line through the anterior aspect of the odontoid without displacement was also noted (Figure 2). Computerized tomography imaging also revealed deformity of the right mandibular condyle and temporomandibular joint, likely related to the trauma. Computerized tomography angiogram of the neck ruled out vascular injury. Due to the unstable nature of the injury, the patient was placed in a c-collar.
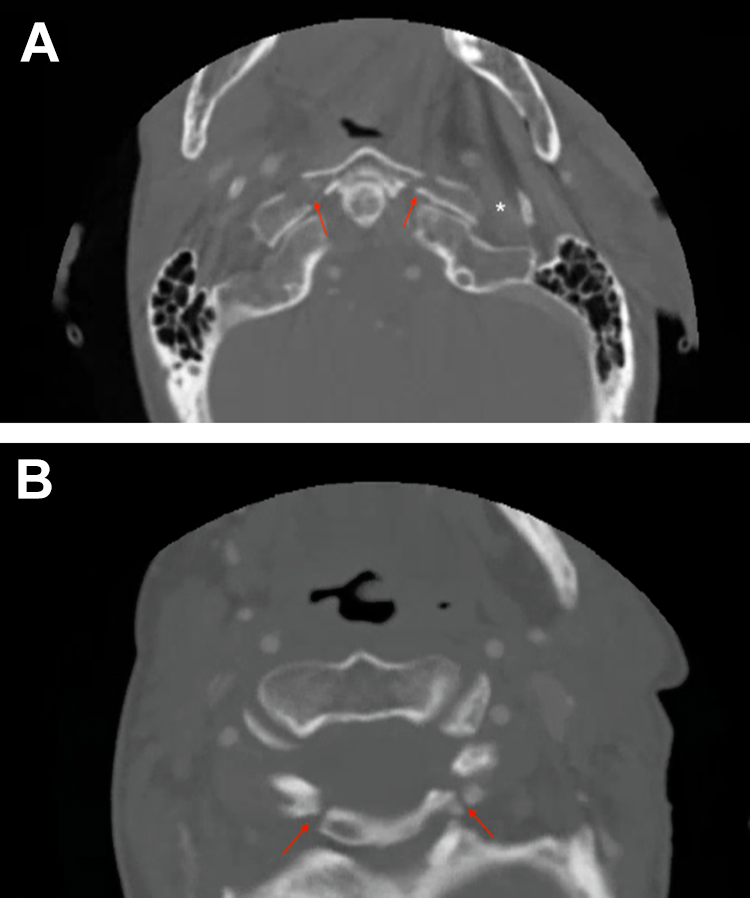
Computed tomography (CT) scans (A-B) show the 4-part Jefferson fracture of the atlas (red arrows). The white * in CT scan (A) denotes the region of the jugular foramen.
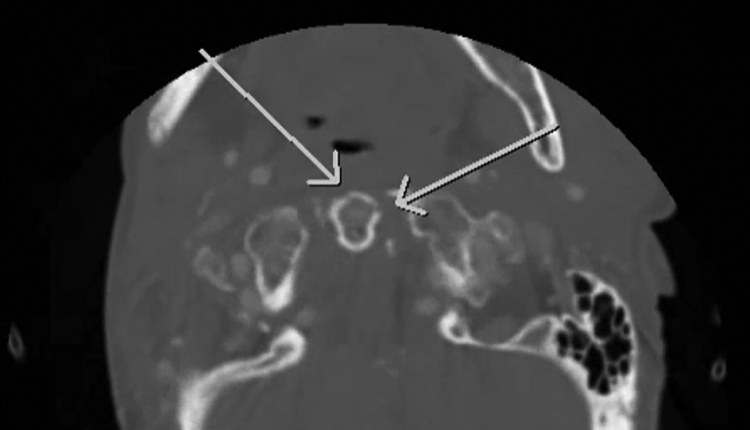
Computed tomography (CT) scan shows the patient’s odontoid fractures (white arrows).
She had severe dysphagia requiring her to remain nil per os (NPO). Otolaryngology was consulted to evaluate dysphagia and dysphonia. Flexible laryngoscopy revealed a paramedian, immobile left vocal fold with moderate bowing resulting in a significant glottic gap. Further cranial nerve examination revealed deficits of cranial nerves IX, X, XI, and XII, evidenced by an absent left gag reflex and left tongue deviation, consistent with Collet-Sicard syndrome (CSS). 1 Radiographic pearls of these neurologic deficits are shown in Figure 3.
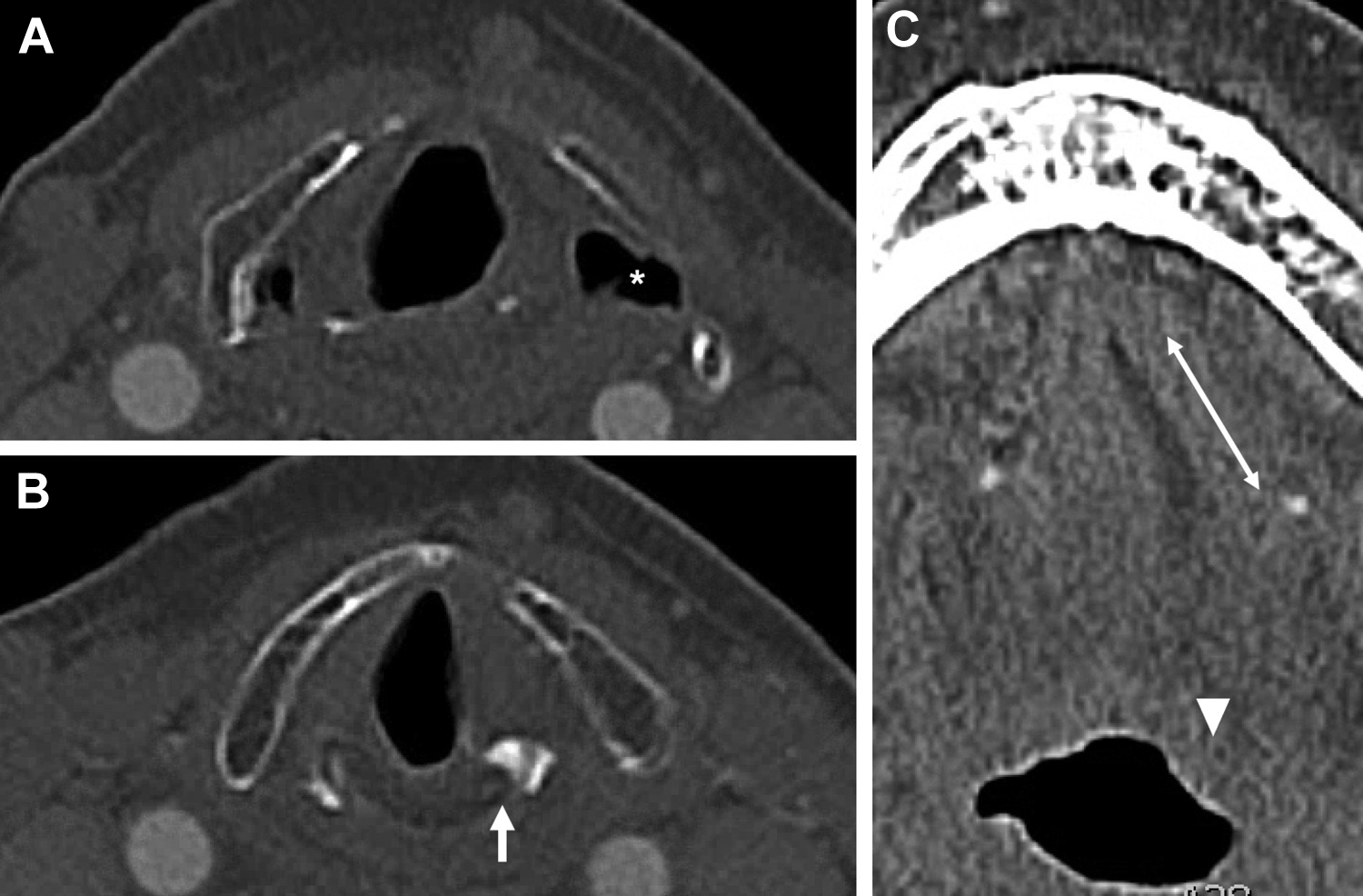
Computed tomography (CT) scan shows radiographic signs of vocal cord paralysis and hypoglossal nerve injury. In CT scan (A), the white * denotes dilated pyriform sinus and in (B) the white arrow denotes the medialized left vocal cord with anteromedial deviation of the arytenoid cartilage. Computed tomography scan (C) shows lengthening and laxity of the left genioglossus (white double arrow) with the tongue at rest and retrodisplacement of left tongue base by gravity secondary to paralyzed tongue protruser muscles (white arrowhead).
Speech language pathology evaluated the patient and discovered moderate to severe pharyngeal dysphagia with reduced hyolaryngeal elevation and signs and symptoms of aspiration across all consistencies. Videofluoroscopic swallow study was performed, confirming deficient tongue base retraction, severely reduced pharyngeal constriction, and frank aspiration.
Given the mechanical nature of the patient’s fall and her abrupt onset of symptoms, trauma was established as the most likely cause. The patient’s symptoms were thought to have resulted from whiplash injury with secondary Jefferson fracture that had likely yielded a compressive peripheral nerve injury. Cerebrovascular accident was ruled out with a CT angiogram, and vascular insult to medullary nuclei without other deficits of facial sensation, dizziness, or Horner’s syndrome would have been unlikely.
Due to her comorbidities and fracture pattern, the patient’s cervical spine injury was treated nonsurgically with the c-collar and several months of halo immobilization. Six days after presentation, she underwent bedside injection laryngoplasty which improved her dysphonia and cough. The patient remains dependent on gastrostomy tube feeds nearly 2 years later.
Collet-Sicard syndrome is a rare condition that manifests as unilateral paralysis of cranial nerves IX, X, XI, and XII.2,3 Collet-Sicard syndrome has multiple etiologies, which can include skull base tumors, vascular lesions, inflammatory disease, and post traumatic fractures.4-7 In rare instances, CSS can result from burst injuries of the atlas (C1), otherwise known as Jefferson fractures. Only 4 cases of CSS resulting from Jefferson fractures have been reported in the literature worldwide, all of which involved male adult patients mainly in high-impact collisions.8-11 This case uniquely involves a female geriatric patient who developed CSS after a 4 part Jefferson fracture sustained during a mechanical fall down 2 stairs.
Jefferson fractures are quite infrequent, representing less than 1% of all spinal injuries.8,9 Although there is very limited literature detailing accounts of CSS following Jefferson fractures, previous cases consist of 2 patients involved in motor vehicle accidents, 1 patient involved in a football tackle, and 1 patient involved in a fall from a height of 2 meters.8-11 Previous reports also indicate that cranial nerve injuries resulting from Jefferson fractures often go undiagnosed, thus emphasizing the importance of a thorough neurological examination in the care of patients presenting with a Jefferson fracture. 9
Our case demonstrates that Jefferson fractures and subsequent CSS are possible even from seemingly minor falls, such as missing 2 steps on a staircase, and thus should be considered as a possible diagnosis in any patient with lower cranial nerve deficits after traumatic injury. Involvement of otolaryngology in the care of these patients is critical, as the otolaryngologist can perform temporizing measures such as injection laryngoplasty to reduce morbidity and improve quality of life.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.