
Abstract

The preauricular fistula, also termed as preauricular cyst, pit, sinus, tract, and fissure, is a common, benign, congenital malformation characterized by a nodule, dent or dimple located anywhere adjacent to the external ear. 1 The preauricular fistula is classified into 7 types by Congdon et al according to the location of sinus orifice (pit) (Figure 1). 2 According to the results of studies using Congdon’s classification to date, although the results differ slightly for each paper, the marginal helicine type is the most common type, accounting for 80% to 90%, followed by the crural type for 10% to 12.5%. 3 However, there have been no papers on the incidence of other types of preauricular fistula. Especially, the posterior helicine type is so extremely rare that we cannot find any case of posterior helicine type in our literature review.
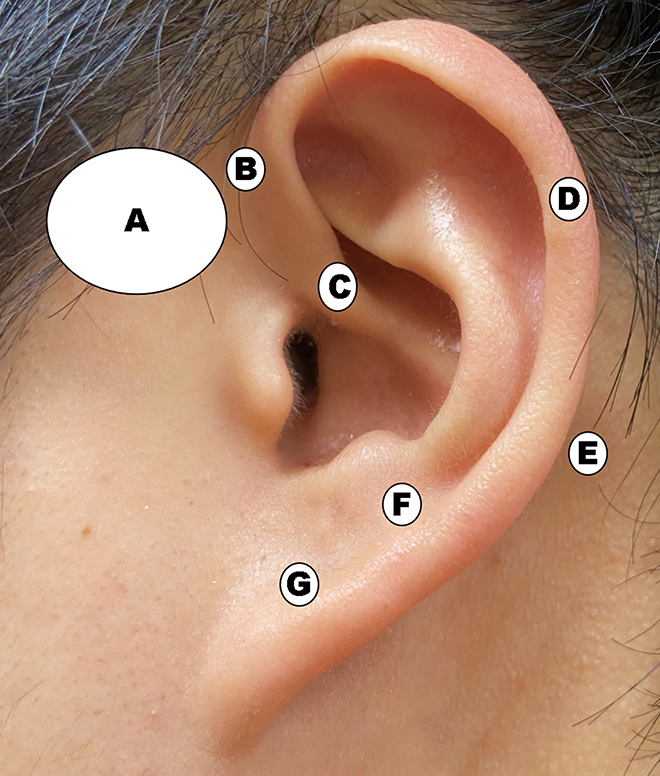
Congdon’s classification. A: Preauricular type, B: Marginal helicine type, C: Crural type, D: Posterior helicine type, E: Postauricular type, F: Helicolobular type, G: Central lobular type.
Recently, as we experienced an asymptomatic case of posterior helicine type of preauricular fistula, we try to describe the difference in the clinical findings compared with the most common type, the marginal helicine type.
Case 1
A 13-year-old healthy female presented with mild snoring. During the physical examination, a small pit was incidentally found in the posterior helix of right ear, together with minimal ear anomaly (Figure 2). Her mother has known that since birth, but she felt no need for treatment because she had no symptoms. Even now, there are no specific symptoms, so we decide to follow-up with no treatment.

Posterior helicine type of preauricular fistua. A small pit (white arrow) incidentally found in the posterior helix of right ear, together with minimal ear anomaly (slightly flattened; white circle).
Case 2
A 27-year-old female presented with the first complaints of reddish swelling in front of right ear for 4 days duration. She had 6-year history of diabetes mellitus but was not treated with medication. She has known that there was a small pit in front of right ear since childhood, but she felt no need for treatment because she had no symptoms. Physical examination confirmed a small pit close to the anterior margin of the ascending portion of the helix (Figure 3). There were swelling, tenderness, and fluctuation around the pit, but no discharge. She was admitted for intravenous antibiotics injection. Initial laboratory tests showed 15 770 white blood cells per microliter of blood, Erythrocyte sedimentation rate (ESR) 81 mm/h, C-reactive protein (CRP) 15.5 mg/L, glucose 293 mg/dL, and HbA1c (glycosylated hemoglobin) 9.7%. After ceftriaxone injection for 5 days with strict glucose control, the symptoms were improved. She was discharged and planned to undergo surgery later.

Marginal helicine type of preacuricular fistula. A photograph showing a preauricular fistula (white arrow) at the ascending helix crus with inflammation (white circle).
Discussion
As described above, there is no report written in English about the posterior helicine type of preauricular fistula as in case 1, so the difference from the marginal helicine type in the clinical symptoms and treatment cannot be described. However, based on our experience of case 1, we present 2 major differences from the marginal helicine type.
First, we think there is the embryological difference in the formation of the 2 types of preauricular fistula. Most frequently cited and accepted theory for the formation of preauricular fistula is “incomplete fusion theory” which is closely associated with the development of auricle. 4 The developing auricle in the human fetus is first noticeable around the sixth week of gestation, developing from the auricular 6 hillocks, which are derived from the first and second branchial arches. The first 3 hillocks derived from the first branchial arch, form the tragus, crus of the helix, and helix, respectively. The final 3 hillocks derived from the second branchial arch, form the antihelix, antitragus, and lobule, respectively.5-7 Accordingly, the most common type, marginal helicine type of preauricular fistulas can be explained as occurring in failure of complete fusion of 6 hillocks.1,6 However, since the pit is located in the helix, the posterior helicine type may be presumed to originate from the abnormal development of the first branchial arch, not the fusion problem of auricular 6 hillocks.
Second, we think there is a difference in the occurrence of symptoms due to infection. The marginal helicine type of preauricular fistula is usually narrow and short and occasionally takes a tortuous course near the external ear and is also attached to the perichondrium of the anterior crus of the helix. 6 The fistula tracts are lined with squamous epithelium and may sequester to produce epithelial-lined subcutaneous cysts or may become infected, leading to cellulitis or abscess. 5 Also, not infrequently, patients present with discharge from the sinus either as a result of desquamating epithelial debris or infection. The most common pathogens causing infection are Staphylococcal species followed by less frequently Proteus, Streptococcus, and Peptococcus species. 8 However, unlike the marginal helicine type, the posterior helicine type is thought that epithelial-lined subcutaneous cyst formation is difficult, and it is most likely found without symptoms as the helix consists of an irregularly shaped plate of elastic cartilage covered by tightly adherent skin on all sides. So, we think there have been no reported cases of the posterior helicine type.
The preauricular fistula frequently appears as a small pit close to the anterior margin of the ascending portion of the helix which may be highly suggestive of the diagnosis. A thorough history and head and neck examination is necessary to investigate evidence of associated anomalies in all cases. 5
The majority of patients with preauricular fistulas is asymptomatic and remains untreated unless they often become infected. The preauricular fistula in acute phase of infection is treated by administration of appropriate antibiotics and if an abscess is present, we do incision and drainage. Complete surgical excision is indicated with recurrent fistular infections, preferably after significant control of the infection or persistent infection. 7 Various surgical techniques have been described but no one technique gave good results. 5 The standard technique is the simple fistulectomy which excises an ellipse of skin surrounding the preauricular fistula opening and to dissect out the individual tract. Most postoperative recurrences result from incomplete removal of the epithelial lining. The more radical technique made by Prasad et al 9 is the supra-auricular approach which is based on the theory that a fistula is almost always included in subcutaneous tissues between temporalis fascia and perichondrium of the helix cartilage. All the tissue superficial to the temporalis fascia with a portion of the cartilage along the base of a preauricular fistula should be excised.5,9 Recurrence rate up to 42% has been reported due to incomplete excision using the standard technique, but when treated with the supra-auricular approach, the recurrence rate is reported as low as 5%.5,9,10 Unfortunately, there is no report about the surgical method of posterior helicine type yet. Since the possibility of infection is relatively minimal as described above, we think surgical treatment may be not necessary.
In conclusion, on the basis of our experience with comprehensive literatures review, there have been no report of the posterior helicine type of preauricular fistula since the histological characteristics of the auricle make it difficult to form epithelial-lined subcutaneous cyst, and so the chance of infection causing symptoms may be very low. In addition, unlike the marginal helicine type, which is the most common type of preauricular fistula, the posterior helicine type may be caused by a developmental problem of the first branchial arch, not incomplete fusion problem of auricular 6 hillocks.
Footnotes
Authors’ Note
Ethics approval not required. The patient’s permission was obtained.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.