
Abstract
Background:
The pathologic features and potential predictive biomarkers for recurrence of antrochoanal polyps (ACPs) in children are not fully understood.
Objectives:
To identify the pathologic differences between recurrent and nonrecurrent group and to explore potential clinical markers which predict recurrence of ACPs in children.
Material and Methods:
A total of 11 recurrent and 21 nonrecurrent ACPs children were enrolled into this retrospect study. Clinical basic information was collected before the first surgery. The counts of vessels were evaluated by hematoxylin–eosin (HE) staining, and CD34 was detected by immunohistochemistry. Meanwhile, the percentage of each tissue inflammatory cells (eosinophils, neutrophils, lymphocytes, and plasma cells) was assessed by HE staining.
Results:
No statistical significance was observed between the 2 groups in the basic clinical features. Moreover, both the counts of blood vessels and the tissue neutrophils percentage were enhanced significantly in group with ACPs recurrence (P < .05). According to the receiver operating characteristic curves, the area under the curve for the counts of blood vessels and tissue neutrophils percentage in the prediction of ACPs’ recurrence was 0.779 (P = .0105) and 0.989 (P < .0001) respectively.
Conclusions and Significance:
It was concluded that the counts of blood vessels and the percentage of tissue neutrophils appeared to be potential excellent predictors of ACPs recurrence in children.
Introduction
Antrochoanal polyps (ACPs), originally described by Killian in 1906, are benign polypoid lesions arising from the mucosa of the maxillary sinus and extending into the choana through the nasal cavity. 1 Antrochoanal polyps account for 4% to 6% of all nasal polyps (NP) in the general population. However, the percentage increases to 35% in children. 2 The clinical manifestations are unilateral progressive nasal obstruction, nasal discharge, headache, epistaxis, dyspnea, and/or obstructing sleep apnea, which seriously affect the physical and mental health among children.3,4
The gold standard for the diagnosis of ACPs is nasal computed tomography (CT). 5 The main treatment for ACPs is surgery currently, and functional endoscopic sinus surgery (FESS) has been widely accepted in children. 6 It is generally believed that the key to prevent recurrences of ACPs in children is completely removing the lesions in the maxillary sinus.1,7 In clinical practice, despite continuous improvement in the surgical method, expansion of the scope of surgery and strive to remove the polyps as completely as possible, the recurrence rate of ACPs in children is still as high as 11%, even reaching to 15% reported in recent systematic review.3,8 The recurrence causes not only economic burden but also secondary trauma for the patients, especially for the younger children. Although various clinical potential risk factors, which lead to surgery recurrence for ACPs among children, were reviewed systematically, no one has reported the risk factors in pathogenesis for recurrence of ACPs in children. 3
In this investigation, we compared the differences between recurrent and nonrecurrent ACPs in children through pathological ways to explore new potential predictors for recurrences. Angiogenesis level and inflammatory cell distribution (eosinophils, neutrophils, lymphocytes, and plasma cells) were assessed in the first removed tissue of polyp in children had ACPs. It was presumed that enhanced angiogenesis level and tissue neutrophils percentage may be related to a more chance to recurrences of ACPs in children.
Material and Methods
Patients
A total of 32 children (between 3 and 18 years) with ACPs at Beijing Children’s Hospital from 2008 to 2016 were recruited for this retrospective study. All patients were diagnosed with ACPs according to the European Position Paper on Rhinosinusitis and Nasal Polyps 9 and followed up for more than 24 months. Moreover, none were applied with antibiotics or corticosteroids within 4-week before FESS. Patients were excluded if they had previous history of nasal sinus surgery, complicated with respiratory diseases such as bronchial asthma and cystic fibrosis, Young syndrome, Kartagener syndrome, and other severe systemic diseases. In addition, recurrence criteria were the postoperative follow-up time was more than 2 years; nasal endoscopy showed mucosal hyperplasia and polypoid changes in the nasal cavity; and/or CT scan showed inflammatory changes in the sinuses and soft tissue shadows of the nasal cavity or paranasal sinuses; a second operation was required. Overall, a total of 101 children diagnosed with ACPs in our hospital from 2008 to 2016. And among them, 11 patients relapsed. Therefore, the recurrent rate of ACPs in our hospital was 10.89% (11/101). However, according to the study’s inclusion/exclusion criteria, most nonrecurrent patients did not meet follow-up time or other conditions, thus 21 children were recruited into nonrecurrent group. Among these 32 enrolled patients, 11 children relapsed after FESS in 2 years (432.09 ± 80.76 days) and other 21 children were nonrecurrent up to now. 10 Informed consents were signed by all patients’ parents and this study obtained approval from the Institution’s Research Ethics Board of Hospital.
Clinical Assessment
Nasal symptoms before surgery were evaluated (Yes/No), including nasal obstruction, nasal discharge, and allergic condition. Age, gender, and polyp’s side were also collected.
Immunohistochemistry and Histologic Evaluation of Polyp Tissue
Tissue of ACPs were collected during surgery and made into formalin-fixed and paraffin-embedded (FFPE) sections. After hematoxylin–eosin staining, blood vessels and inflammatory cells (eosinophils, neutrophils, lymphocytes, and plasma cells) were counted under ×100 bright field and ×400 bright field, respectively.
Immunohistochemistry staining for CD34 was as following: After dewaxing, unstained 3-µm FFPE sections were heated for 30 minutes with Bond Epitope Retrieval Solution 1 or 2 (corresponding NO. AR9641 or AR9640; Leica Biosystems Newcastle Ltd) using a Leica Bond-MAXTM automated immunostainer (Leica Microsystems Inc) and incubated with CD34 primary antibodies (ZM-0046, ZSGB-BIO) at 4 °C overnight. Then, the slides were incubated with Mouse HRP Polymer (ZM-0046, PV-8000), and finally developed with DAB (3, 3′-diaminobenzidine-4HCl, Sigma) to generate a brown reaction product. Blood vessels were consequently defined as any brown-stained and the amount of CD34-positive vessels were evaluated under ×200 bright field.
Each sample was read by 2 technicians in a blind method for 10 nonoverlapping fields, and the number of blood vessels, the count of CD34-positive vessels, and the percentage of inflammatory cells were calculated. Then, the mean of the 10 values was taken for comparison.
Statistical Analysis
Statistical analysis was performed by using SPSS version 19.0 (IBM Corp). Data were expressed as means ± standard deviation. Continuous variable differences were analyzed by the Student t test. The χ2 test was used for a 2-group comparison of gender, polyp’s side, nasal obstruction, nasal discharge, and allergic condition status.
Receiver operating characteristic (ROC) curve was generated to determine the value of the counts of tissue blood vessels and the percentage of tissue neutrophils as 2 potentially predictive biomarkers for recurrence of ACPs in children.
Results
Clinical Features
The clinical characteristics of patients with and without recurrence of ACPs are shown in Table 1. In this study, 11 children had recurrent ACPs and 21 children were nonrecurrence ACPs. No statistically significant difference was observed between the means of these 2 groups in the basic clinical features, including age, gender, polyp’s side, nasal obstruction, nasal discharge, and atopy (P > .05). Moreover, they all did not present with epistaxis. It revealed that the 2 groups were comparable in the baseline characteristics.
Clinical Features of the Patients.

Angiogenesis
Assessment of angiogenesis level indicated that the counts of blood vessels were higher in the group of recurrence (39.8 ± 11.7) than that in the group of nonrecurrence (10.1 ± 4.7; P < .05; Figure 1A and B). Besides, the scale of blood vessels was found to be significantly larger in the recurrent group compared with the nonrecurrent group (Figure 1B). Furthermore, it was consistent with the counts of blood vessels by CD34 staining. The amount of CD34-positive vessels was increased significantly in recurrent group (29.2 ± 13.5) than that in the nonrecurrence of ACPs in children (11.7 ± 4.0; P < .0001; Figure 2A and B). All the results revealed that the level of angiogenesis was elevated in subgroups of children with ACPs recurrences.
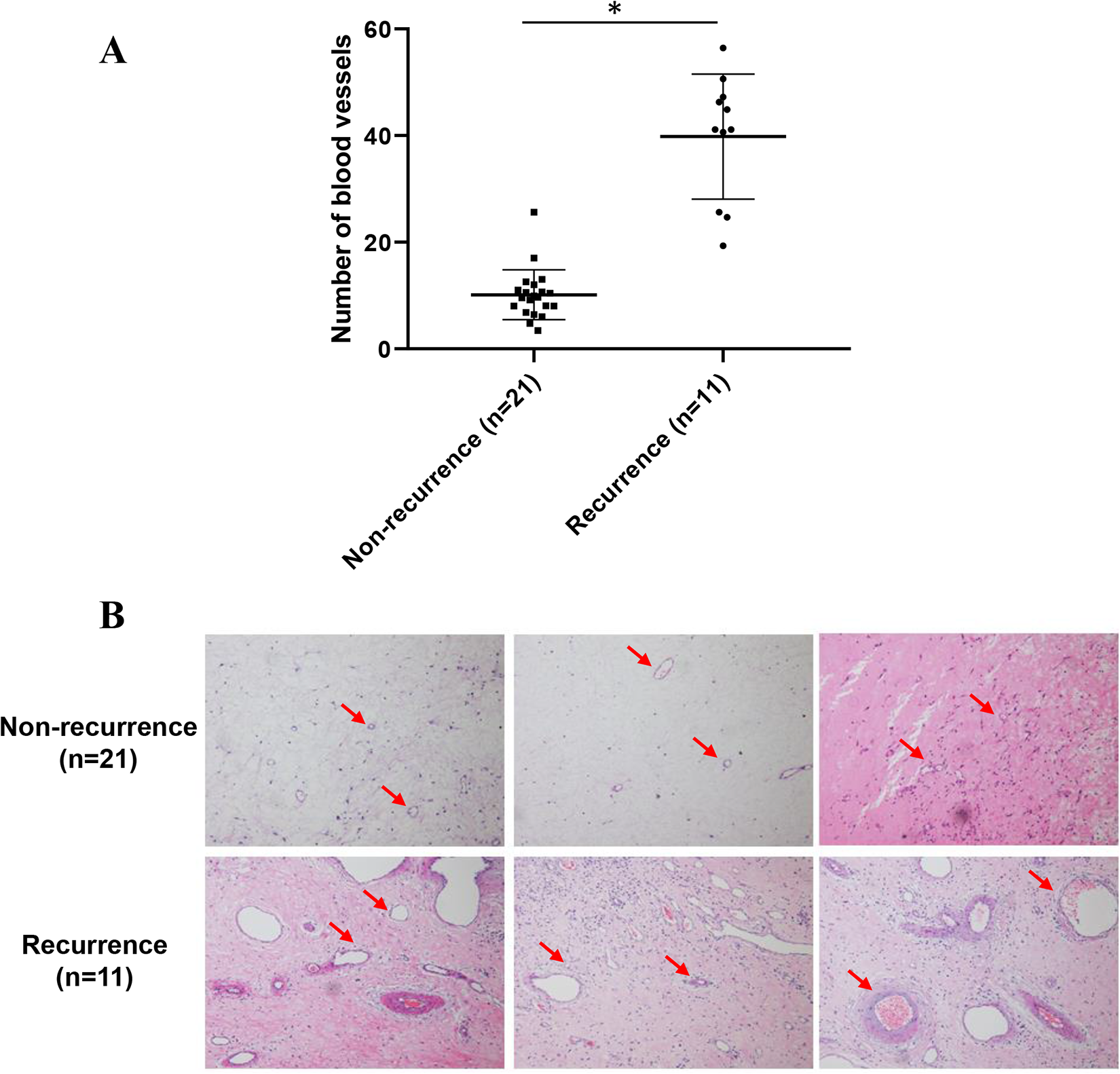
The number of blood vessels in polyp tissue of children with recurrent antrochoanal polyps (ACPs) increased significantly (A) Paraffin sections of polyps in children with recurrent and nonrecurrent ACPs were stained with hematoxylin–eosin (HE). An immunohistochemical slide was taken from each child, 10 fields were randomly selected under a ×100 bright field. And then the number of blood vessels was counted (P < .0001). (B) HE staining of paraffin sections of polyps in children with recurrent and nonrecurrent ACPs. Arrows indicate blood vessels.
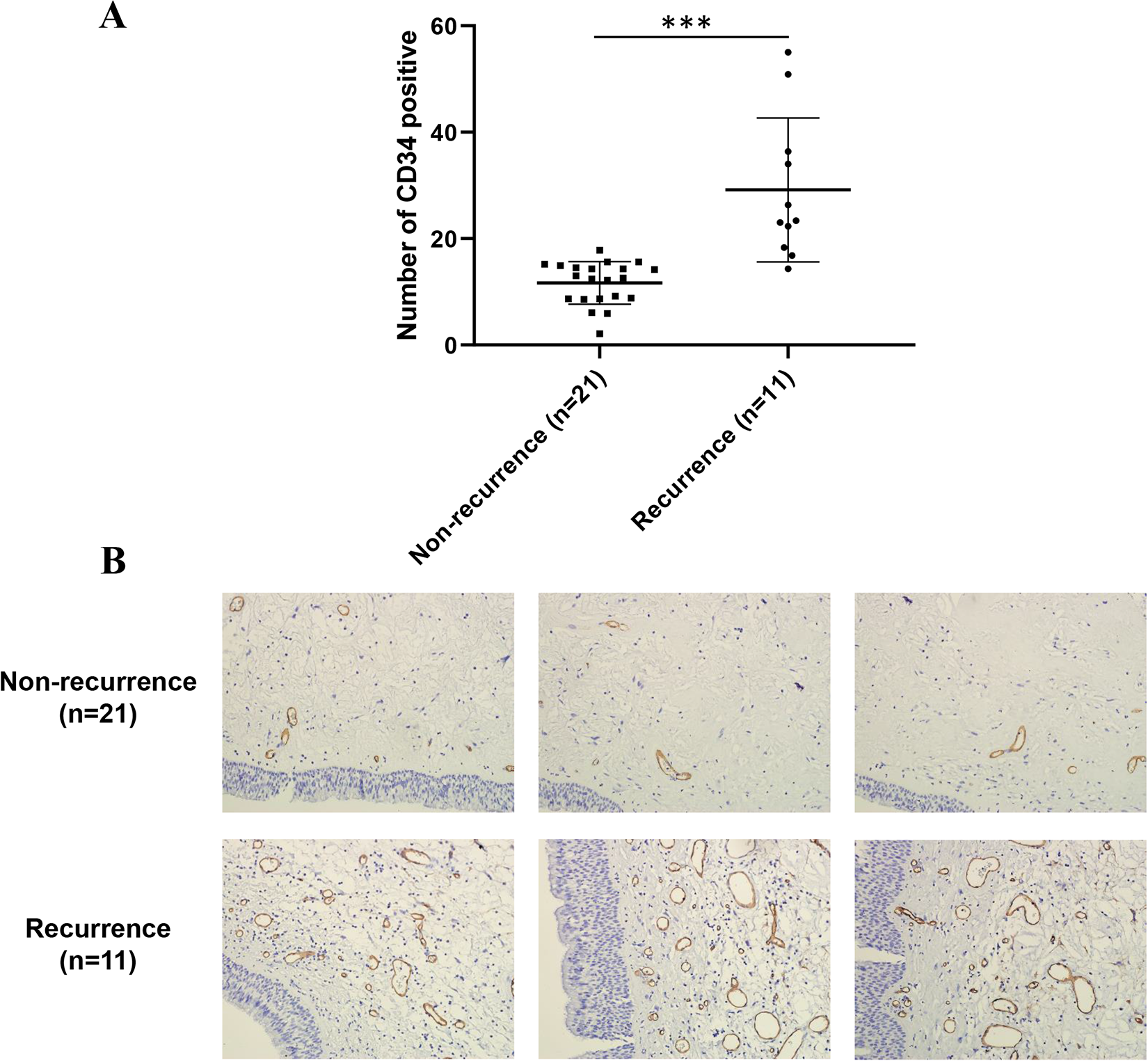
The number of CD34 positive signals in polyp tissue of children with recurrent antrochoanal polyps (ACPs) increased significantly (A) Paraffin sections of polyps in children with recurrent and nonrecurrent ACPs were stained with CD34 antibody. An immunohistochemical slide was taken from each child, 10 fields were randomly selected under a ×200 bright field. And then the number of CD34-positive signals was counted (P < .0001). (B) CD34 antibody staining of paraffin sections of polyps in children with recurrent and nonrecurrent ACPs.
Inflammatory Cells Infiltration
Major tissue inflammatory cells (eosinophils, neutrophils, lymphocytes, and plasma cells) were counted in both groups’ polyp tissue. No statistically significant difference was found between the 2 groups in the percentage of tissue eosinophils and tissue lymphocytes. In contract, evaluation of tissue neutrophils percentage was significantly higher in the recurrence of ACPs in children compared with the nonrecurrent group (P < .05). Meanwhile, the proportions of plasma cells were found to be significantly lower in the recurrent group compared with the nonrecurrent group (Figure 3, Table 2).
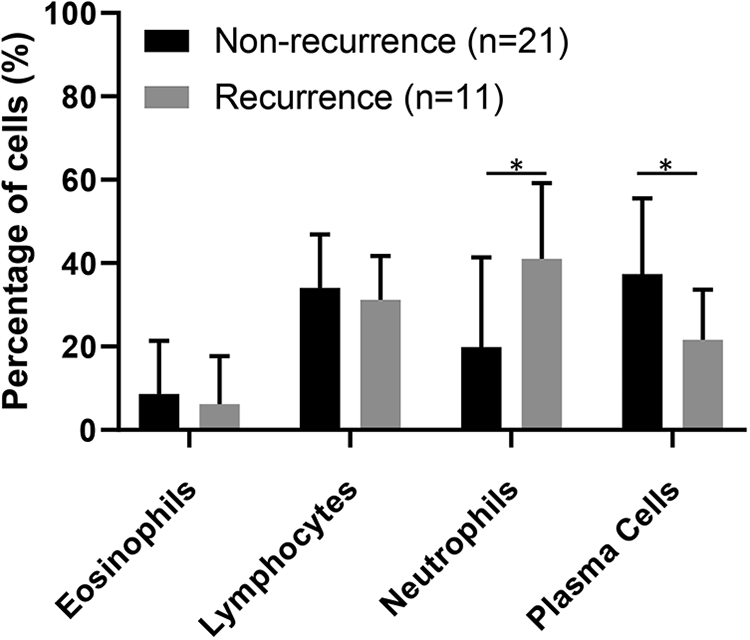
Comparison of the proportion of tissue inflammatory cells infiltration between recurrent and nonrecurrent group hematoxylin–eosin (HE)–stained formalin-fixed and paraffin-embedded (FFPE) sections of polyps in children with recurrent and nonrecurrent antrochoanal polyps (ACPs) were taken from each child. For each section, 10 fields were randomly selected under a ×400 bright field. The number of tissue inflammatory cells (eosinophils, neutrophils, lymphocytes, and plasma cells) was counted, and the percentage of these 4 types of cells was calculated, respectively. Then, the mean percentage of the 10 values was recorded for each inflammatory cell.
Difference of Histological Features Between Recurrent and Nonrecurrent Group.
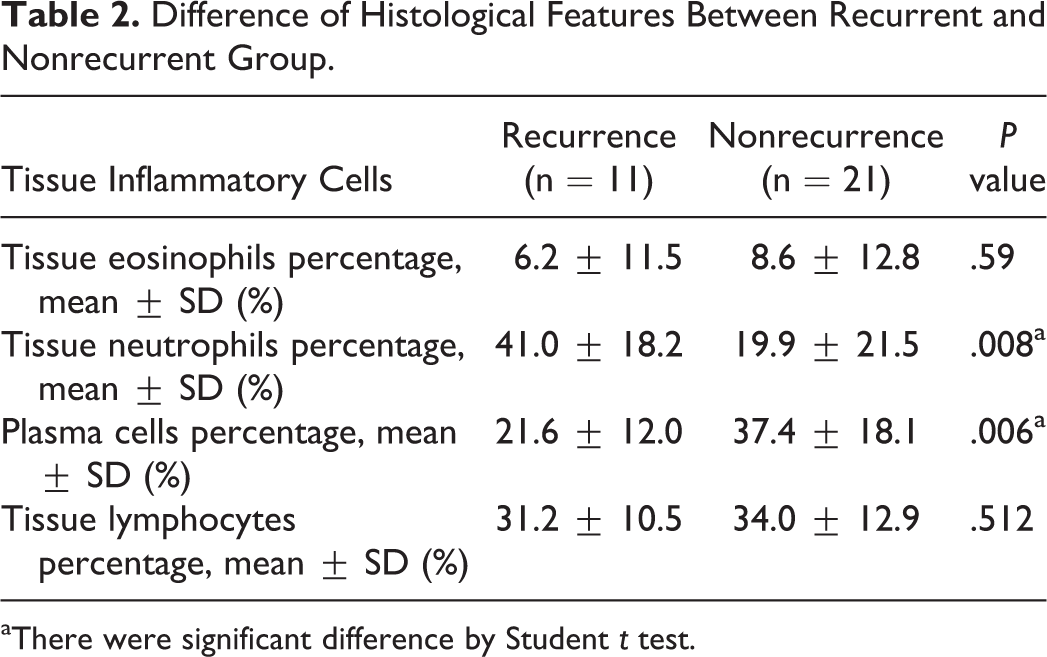
aThere were significant difference by Student t test.
Potentially Predictive Value of Angiogenesis Level and Tissue Neutrophils Percentage for Recurrence of ACPs in Children
To analyze the potentially predictive value of angiogenesis level and tissue neutrophils percentage for ACPs’ recurrence in children, the ROC curves were plotted. Receiver operating characteristic curves for the number of vessels associated with recurrence of ACP are shown in Figure 4, and the corresponding area under the curve (AUC) was 0.9892 (95% CI: 0.9628-1.000, P < .0001). With a cutoff angiogenesis level of 22 vessels per field, the best specificity was 52.38% and the best sensitivity was 90.91%. Meanwhile, for tissue neutrophils, the corresponding AUC of ROC curves was 0.7792 (95% CI: 0.6174-0.9411, P = .0105). With a cutoff tissue neutrophils percentage of 11.53%, the best specificity was 90.91% and the best sensitivity was 95.24%. These results indicated that assessment of vessels number and the percentage of tissue neutrophils had the potential value for being an excellent predictor for recurrence of ACPs in children.
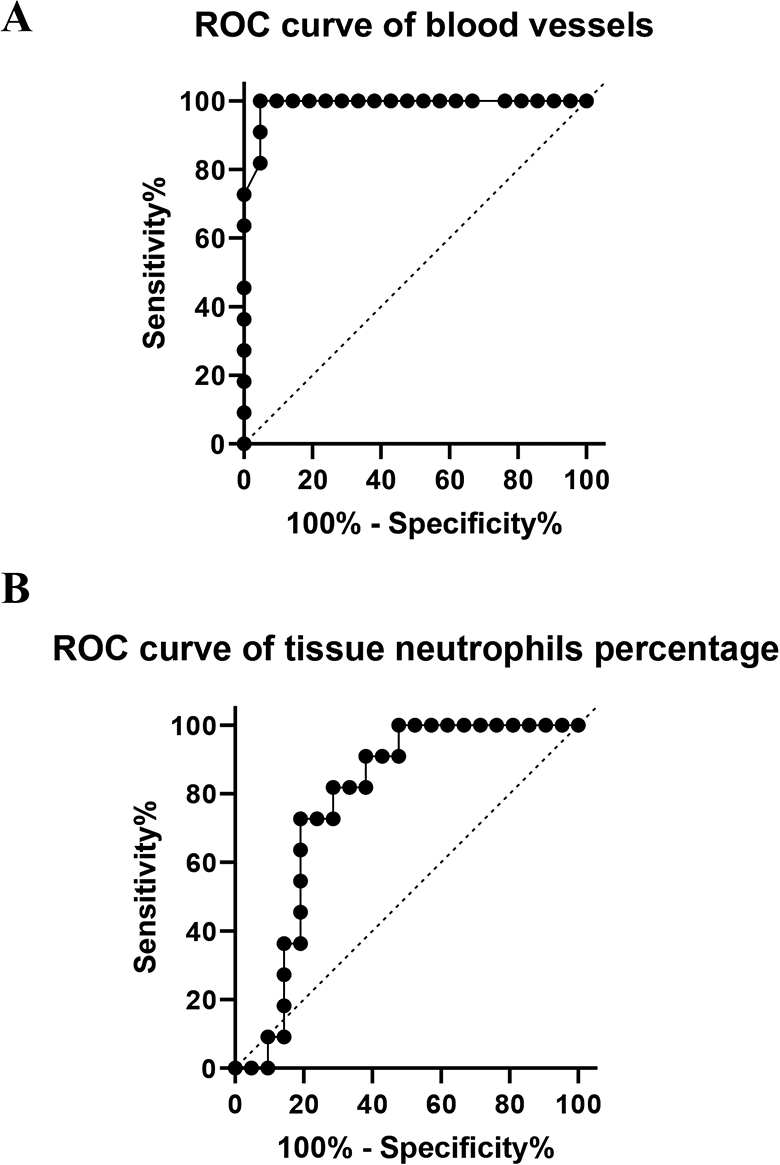
Receiver operating characteristic (ROC) curves revealed that the counts of blood vessels and percentage of tissue neutrophils had the potential for being an excellent predictor of antrochoanal polyps (ACPs) recurrence (A) ROC curve for the counts of blood vessels associated with ACPs recurrence. The corresponding area under the curve (AUC) was 0.9892 (95% CI: 0.9628-1.000, P < .0001). (B) ROC curve for the percentage of tissue neutrophils associated with ACPs recurrence. The corresponding AUC was 0.7792 (95% CI: 0.6174-0.9411, P = .0105).
Discussion
As a benign polypoid lesion, ACPs has significant high incidence in children. Although FFPE is the best treatment for ACPs, there are still about 11% to 15% child patients having recurrence. The pathogenesis and etiology of ACPs are still unknown, especially the reason of high frequency of recurrence. How to control and reduce the rate of recurrence for ACPs is a serious challenge to clinical practice. Clarifying the risk factors for recurrence of ACPs is conducive to the development of treatment strategies, effective control of the disease, avoiding the burden of multiple surgical operations on children, and saving limited clinical resources for society. We reasoned that the recurrence of ACPs in children may have other factors besides the causal relationship with surgical resection. Previous studies showed that the recurrence of NP is related to symptom scores, origin of polyps, combined asthma, allergic status, serum eosinophil and basophil levels, histopathological characteristics, inflammatory factors, and immunoremodeling markers.11-13 Moreover, it revealed that tissue lymphangiogenic vessel density may be related to the recurrence of sinusitis and NP. 14 But so far, no research has been reported on the pathologic differences between recurrent and nonrecurrent ACPs in children. Analyzing the pathologic characteristics could be contributed to explore potential clinical markers to predict recurrence of ACPs in children.
In this study, the basic clinical features, including age, gender, polyp’s side, nasal obstruction, nasal discharge, and atopy condition before surgery were retrospective analyzed between recurrent and nonrecurrent group of ACPs in children. There was no significant difference in these basic clinical features. Notably, only one patient had atopy in total 32 patients, indicating that the onset of ACPs was not correlated with allergies inevitably.
Previously study clarified that angiogenesis played a role in the pathogenesis of NP. However, there was no difference in angiogenesis between recurrent versus nonrecurrent NP. 15 Although the previous study show angiogenesis in NP was significantly more enhanced than ACPs, there was no analysis about the relationship between angiogenesis and the prognosis of ACPs. In our study, the counts of blood vessels were compared between recurrent and nonrecurrent group of ACPs in children. Furthermore, as a well-known angiogenic indicator, CD34 was stained to detect the blood vessels in ACPs’ tissue. And the amount of CD34 was also increased in recurrent group of ACPs in children. All these results revealed that the primary ACPs’ tissue from recurrent group occupied more vessels than nonrecurrence group. In other words, increased angiogenesis level may lead to recurrence of ACPs in children.
As one major type of white blood cells, neutrophils originate from the bone marrow. 16 It is well known that neutrophils act immune function against invading pathogens such as bacteria. Once resting neutrophils are primed by pathogens, they will move to the site of infection or inflammation and then activate signals to trigger bacterial killing. 17 In our previous study, the allergic condition had no significantly contribution to ACPs pathogenesis, which is in accord with the percentage of tissue eosinophils had no significantly difference between recurrent and nonrecurrent group this study. 18 Meanwhile, previous results also showed that neutrophils could be recruited to sites of infection by IL-6 enhanced in ACPs patients. 18 In our study, the percentage of tissue neutrophils was higher in recurrent group than nonrecurrent group of ACPs in children, indicating that the level of infection or inflammation enhanced was one of the major reason to induce ACPs’ recurrence in pediatric age group.
Furthermore, there has been verified that neutrophils could enhance angiogenesis both in vivo and in vitro in recent studies. In bone regenerative processes, neutrophils induced the expression of pro-angiogenic markers, such as CD34, VEGF-A (Vascular Endothelial Growth Factor A), EGF (Epidermal Growth Factor) and FGF2 (Fibroblast Growth Factor 2) to promote angiogenic process in tissue. 19 Moreover, acting as one kind of immune cells, neutrophils could increase VEGF-A availability during the angiogenesis in tumor microenvironment. 20 In our study, Pearson analysis revealed that the tissue neutrophils percentage of all 4 major types tissue inflammatory cells was correlated with the counts of tissue vessels (Spearman r = 0.456, P < .05; Supplemental Figure 1). It was presumed that neutrophil-mediated enhancement of angiogenesis in ACPs may be one of the reason for recurrence in children.
In this clinical–pathological study, angiogenesis and tissue neutrophils infiltration were compared between recurrent and nonrecurrent ACPs in children. It hypothesized that the results of this investigation might provide insight toward better understanding of the pathogenesis of recurrent ACPs in children. It was presumed that enhanced level of angiogenesis and tissue neutrophils may be related to a more chance to recurrence in ACPs children. Moreover, it was reasonable that assessment of blood vessels counts and the percentage of tissue neutrophils had the potential for being an excellent predictor of ACPs recurrence in children. In the future, regular follow-up review could be used to expand the sample size and conduct prospective studies for verification. If these new blood vessels could be inhibited or destroyed in a targeted manner, it is possible to prevent the growth and recurrence of ACPs. Further research on the molecular mechanism of vascular proliferation, its regulatory pathways, the relationship between inflammatory vascular proliferation and neutrophils, and an in-depth understanding of the recurrence mechanism of ACPs in children are of great significance for reducing surgical injuries and reducing the burden on children.
Limitations
There are some limitations in the present study. Firstly, the small sample size leading to the rate of recurrence and the data of polyp’s side were biased. Secondly, the imaging data such as anatomical abnormality and size of the polyps were not analyzed as a separate risk factor in this study. In addition, although the same protocol of FESS was performed in all patients, it also did not avoid the variability of techniques across operators, which may induce recurrence of ACPs. Finally, further study of the mechanisms in angiogenesis leading to ACPs recurrence needs to be clarified.
Supplemental Material
sj-tif-1-ear-10.1177_0145561320963627 – Supplemental Material for Predictive Significance of Enhanced Level of Angiogenesis and Tissue Neutrophils for Antrochoanal Polyps Recurrence in Children
Supplemental Material, sj-tif-1-ear-10.1177_0145561320963627 for Predictive Significance of Enhanced Level of Angiogenesis and Tissue Neutrophils for Antrochoanal Polyps Recurrence in Children by Yeran Yang, Beibei Song, Xiaojian Yang, Chunju Zhou, Lixing Tang, Jie Lu, Pengpeng Wang, Ping Chu, Shujing Han, Yongli Guo and Wentong Ge in Ear, Nose & Throat Journal
Footnotes
Acknowledgments
The authors are grateful to the child patients and their parents for their participation in this study.
Authors’ Note
Y.Y. and B.S. contributed equally to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Pediatric Specialty Collaborative Development Center of Beijing Hospital Authority (XTZD20180103), Beijing Natural Science Foundation Program and Scientific Research Key Program of Beijing Municipal Commission of Education (KZ201810025034), the Special Fund of the Pediatric Medical Coordinated Development Center of Beijing Hospitals Authority (XTCX201806), and Beijing Advanced Innovation Center for Big Data-Based Precision Medicine, Beihang University & Capital Medical University, Beijing (BHME- 201804, BHME- 201904).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.