
Abstract

A 56-year-old woman presented to the otolaryngology department with a 5-month history of postnasal drip and foul odor from the left nasal cavity. She had surgical history of transsphenoidal approach for pituitary adenoma surgery 9 years ago and a revision transsphenoidal hypophysectomy with skull base repair with titanium mesh at the same site 5 years ago. Endoscopic examination of the nasal cavity revealed purulent discharges from the left sphenoid sinus with swollen mucosa which orifice had been enlarged by previous surgeries, and sphenoid orifice at right side was not observed. Her symptoms showed no improvement with oral antibiotics treatment. On examination after 2 weeks, left sphenoid sinus orifice mucosa swelling was improved and the sinus was well-opened and could be observed with nasal endoscope. Whitish hair-like filamentous mycelium rising from the mud-like discharges were observed inside the sinus (Figure 1). Cultures of the nasal discharges obtained at presentation were positive for Staphylococcus aereus and Aspergillus species, a most common pathologic fungus species found in nasal cavity. Computed tomography of the paranasal sinus was subsequently performed and revealed an abnormal soft tissue lesion in the right side of the sphenoid sinus at post-transsphenoidal hypophysectomy status (Figure 2). A diagnosis of an isolated sphenoid sinusitis was made, and functional endoscopic sinus surgery was undergone removing the fungal ball and underlying infective mucosa. Previous skull base repair with titanium mesh could be an infection source and if so implant removal might be needed. Sphenoid sinus mucosa was intact without any evidence of implant displacement or inflammation. Surgical specimen including hyphae was revealed aspergilloma with chronic inflammation. At follow-up 6 months after the surgery, she was symptom-free, and endoscopic examination showed the healed sphenoid mucosa with well-opened sinusotomy opening at both sides.
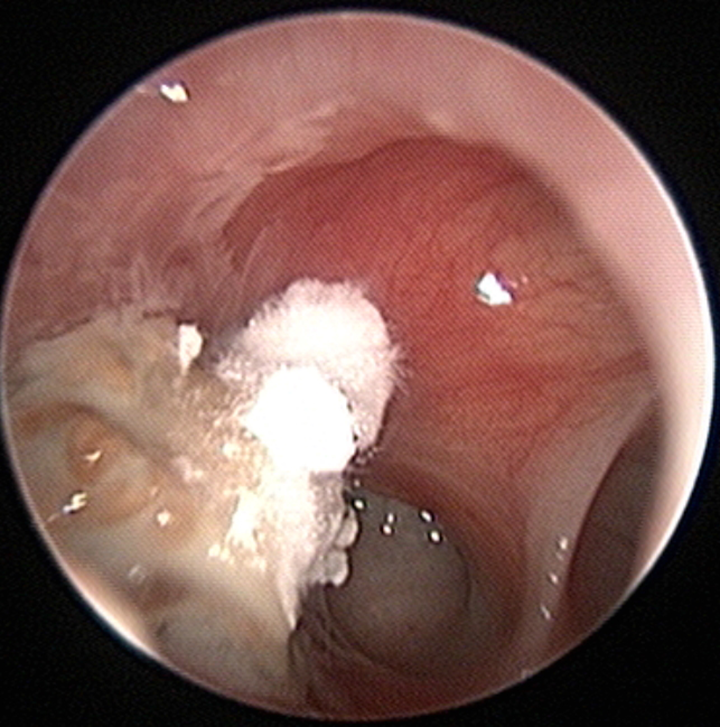
Sphenoid sinusitis after transsphenoidal approach is shown in the endoscopic view (left side). Filamentous fungal hyphae growing over mud-like pus discharges are noted inside the sinus.
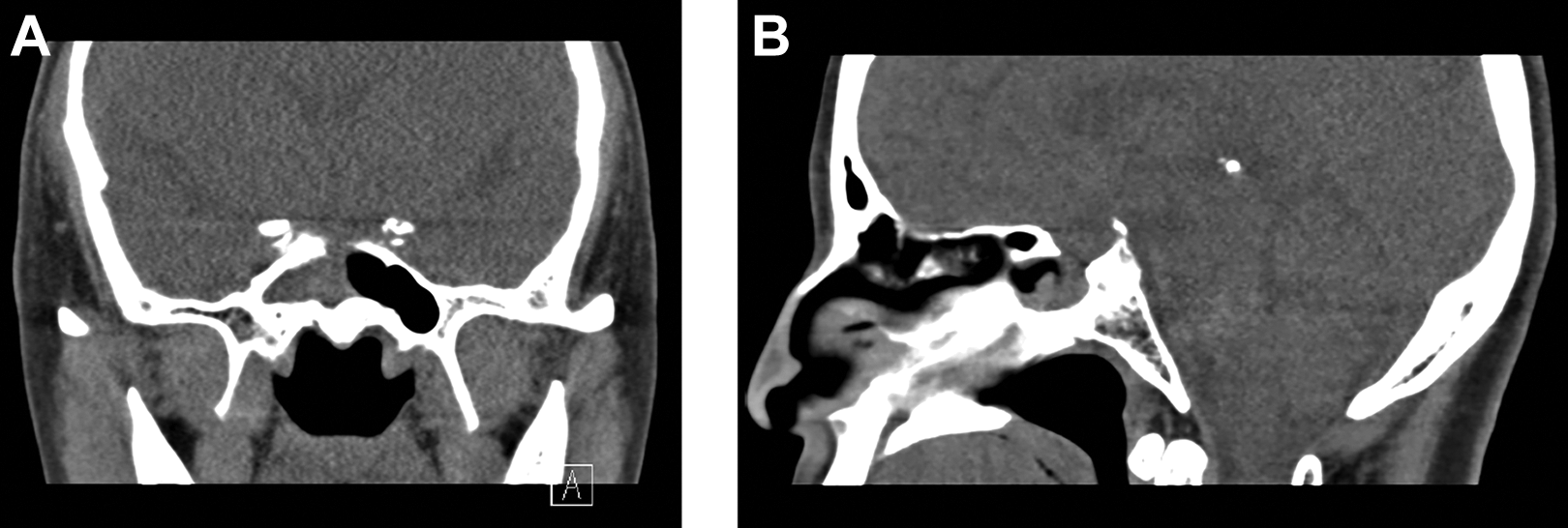
Preoperative paranasal sinus computed tomography (CT) scan without contrast shows a sphenoid sinusitis with the partial dehiscence of the skull base made from the previous transsphenoidal pituitary hypophysectomy; (A) coronal view, (B) sagittal view. Note that sphenoid septation is not observed, and the infection is started from the right side and extended to the left side as shown in Figure 1.
Isolated sphenoid sinusitis and/or mucocele is seen in fewer than 3% of all sinusitis patients, and much rarer in patients received transsphenoidal surgery. 1 Isolated fungal sphenoid sinusitis is also rare and is considered as indolent, noninvasive form of fungal sinusitis, without the need for antifungal therapy following surgery. 2 Sphenoid sinus mycetomas are known to mimic pituitary adenomas, especially when associated with an atypical presentations, previous history of sellar surgery and appearance in immunocompetent patients.1-3
Endonasal transsphenoidal approach has been a well-established method for pituitary gland tumor surgery. Complications of endonasal transsphenoidal surgery are epistaxis, septal perforation, sinusitis, and atrophic rhinitis, relatively not life-threatening compared to open craniotomy.4,5 Isolated sphenoid sinusitis after endonasal transsphenoidal hypophysectomy is a rare complication. Pituitary tumor surgery using transsphenoial approach breaks the anatomical bony barrier between nasal sinus and central nervous system, so the concern of potential ascending infection to central nervous system has been needed. 1
The pathophysiology of sphenoid sinusitis involves the blockage of the sphenoid ostium and impaired mucociliary clearance leading to stasis and secondary bacterial infection, preventing clearance of any fungal hyphae present in the nasal mucosa.1,4,6 Viral or bacterial infection can provide sufficient nutrients to the fungus, which start proliferating in a low pH medium, and sometimes forming a fungal ball eventually. 6
Incomplete mucosal removal or damage of the mucosa near opening during the transsphenoidal approach may result in adhesions or obstruction of the sinus, also leading to possible sinusitis. 4 Mucocele, also, caused by the obstruction of the sinus ostium, which may result from the previous surgery. A retrospective chart review of 323 patients received transsphenoidal pituitary hypophysectomy reported that 20 (6.2%) cases experienced postoperative sinusitis or mucocele, and 7 patients needed endoscopic sphenoidotomy for treatment. 1 The materials remained in the sphenoid sinus for reconstruction such as buttress materials (bone chip, cartilage, or titanium mesh) and tissue sealants in the surgical field may trigger tissue reaction and obstruct sphenoidotomy outlet.7,8
Partially obstructed sphenoid sinus with stasis of nasal discharges may provide a good condition for settlement of bacteria and/or fungi, and well-aerated sinus with sufficient nutrition support may lead fungal hyphae formation in the sinus, shown in this case.
Footnotes
Authors’ Note
The institutional review board of the National Health Insurance Service Ilsan Hospital exempted the review of this study (NHIMC 2020-08-006).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.