
Abstract

A 26-year-old woman presented with right-sided ear fullness and gradual onset of right-sided hearing disturbance over several years. She had no history of recurrent ear infection or trauma, nor did she complain of other auditory or vestibular symptoms. Pure tone audiometry indicated conductive hearing loss, but the other neurological examinations were normal. Mean hearing level of the right-side ear at 0.5, 1, 2, and 3 kHz calculated from the audiograms was 56.25 dB with an air-bone gap of 48.75 dB. Otomicroscopy demonstrated a dark, reddish, pulsatile mass behind the tympanic membrane in the posteroinferior quadrant of the middle ear cavity (Figure 1A, Supplemental Video). The tympanic membrane movement in the video was due to transmitted pulsations from the high-riding jugular bulb (HRJB) and not the pneumotoscopy. Temporal bone computed tomography (CT) revealed a right-sided HRJB with bony dehiscence, which protruded into the middle ear (Figure 1B). The left temporal bone appeared normal; intracranial aneurysm or mass, inner ear anomaly, vascular malformation, or other persistent embryological vessels were excluded by magnetic resonance imaging and angiography. The patient was diagnosed with conductive hearing loss and ear fullness due to a HRJB in the middle ear and was informed of possible surgical complications. Despite providing informed consent, the patient refused to undergo surgery or additional radiological interventions and was managed conservatively.
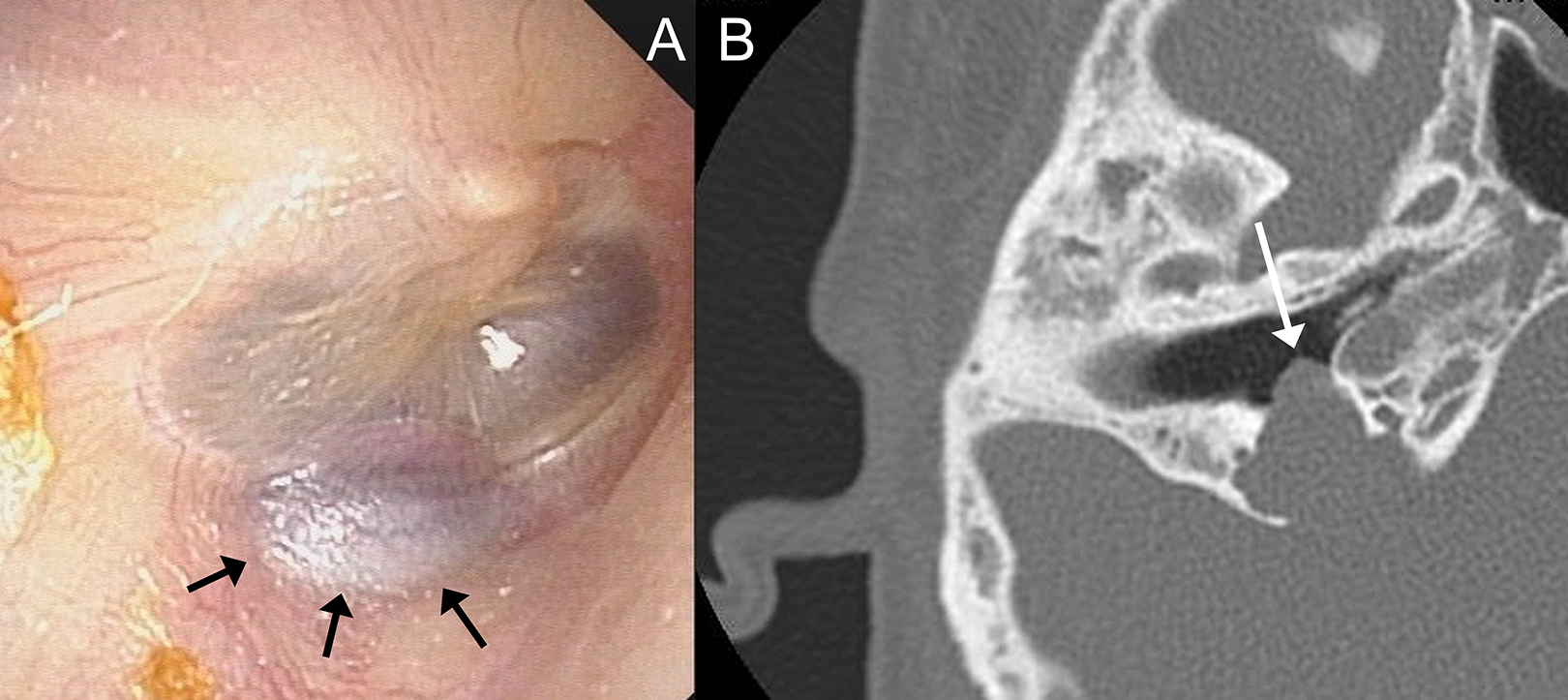
A, Otoscopic images of the right ear show a dark discoloration in the posteroinferior quadrant of the right tympanic membrane (black arrows). The tympanic membrane movement in the video is due to transmitted pulsations from the high-riding jugular bulb and not the pneumotoscopy. B, Temporal bone computed tomography revealed a right-sided high-riding jugular bulb with bony dehiscence that protruded into the middle ear (white arrow).
The axial temporal bone CT image in the current case revealed a dehiscent HRJB protruding into the hypotympanum of the middle ear (Figure 1B) and was in contact with her tympanic membrane (Figure 1A, Supplemental Video). Vascular anomalies of the temporal bone are extremely rare; however, they may cause complications during middle ear surgeries.1,2 The jugular bulb is the expanded upper end of the jugular vein situated in the jugular fossa. It is a venous structure that can be located close to the inner ear. High-riding jugular bulb can be present in 10% to 15% of individuals and can be dehiscent in 0.5% to 1.7% of individuals. 2 It is not present at the time of birth. The size and location are dependent on the pneumatization of the mastoid bone. The size is not any criterion for any pathologies.1-3 Patients with these anomalies may be asymptomatic or experience hearing loss, pulsatile tinnitus, ear pain, or aural fullness. Aberrant HRJB can mimic other middle ear lesions, including a glomus tumor. 1 Otoscopically, it is seen as a blue mass behind an intact tympanic membrane and can be misdiagnosed as a glomus tumor, which may become distended on Valsalva or ipsilateral jugular compression. 1 The HRJB is clinically significant because it can cause a fatal hemorrhage due to an inadvertent puncture in patients undergoing myringotomy or tympanoplasty.1-3 During the surgeries, if a mass is encountered in the middle ear cavity, a biopsy should never be attempted. Although in most cases, HRJB is incidentally detected, and less patients may suffer hearing loss, tinnitus, and vertigo.1-3 Tinnitus is the most common symptom (50.4%), whereas hearing disturbances are rare (1.9%). 3 Even once the diagnosis is established, surgical correction of HRJB is not recommended because it could disrupt venous flow and increase the risk of intracranial hypertension. Removal of the protruded jugular bulb from the affected middle ear has been shown to not improve hearing function.4,5 Moreover, preoperative imaging is essential to avoid intraoperative complications arising from the misdiagnosis, such as life-threatening bleeding.
In conclusion, clinicians should be aware of temporal bone vascular malformations. Aberrant HRJB should be differentially diagnosed in patients with ear diseases to prevent untoward and fatal surgical complications. Although an atypical manifestation, frequent cases of aberrant HRJB in the middle ear have been reported. However, to our knowledge, no useful photographs or video of patients with aberrant HRJB-mediated ear fullness and pulsatile tympanic membrane have been reported in literature. The image reported herein is extremely rare and educationally valuable.
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.