
Abstract
Objective:
The etiology of sudden sensorineural hearing loss (SSNHL) remains unknown; inflammation may be one cause. We retrospectively studied SSHNL cases in terms of the inflammatory parameters involved.
Methods:
We reviewed 169 SSNHL cases. The control group contained 132 patients with vocal cord polyps. The C-reactive protein (CRP) level, CRP/serum albumin (Alb) ratio, and neutrophil/lymphocyte ratio (NLR) were compared between the 2 groups. The relationships between these parameters and the time to treatment after SSHNL onset, hearing level, and therapeutic effects were also analyzed.
Results:
The CRP level, CRP/Alb ratio, and NLR were higher in SSNHL patients than in controls, but only the NLR differed significantly between the 2 groups. We found no significant differences between patients with different hearing levels, those evaluated at various times after SSNHL onset, and those with different outcomes.
Conclusion:
The NLR is a reliable SSNHL diagnostic marker. The CRP level and CRP/Alb ratio are not useful indicators.
Introduction
Sudden sensorineural hearing loss (SSNHL), hearing loss of at least 30 dB occurring at a minimum of 3 consecutive frequencies within 72 hours, 1 is a common emergency encountered in ENT departments. Blood circulation disorders are thought to be the major causes of SSNHL 2 -4 ; however, the etiologies remain unclear. Viral infections and autoimmune diseases may be in play. The inflammatory parameters measured 5 -7 include the C-reactive protein (CRP) level, 8,9 CRP/serum albumin (Alb) ratio, 10 and neutrophil/lymphocyte ratio (NLR). 11,12 The results have been controversial, especially the CRP data. Some authors found no relationship between the CRP level and SSNHL. 7,13,14 One study suggested that the CRP/Alb ratio might be prognostic of SSNHL development. 10 We sought relationships between inflammatory parameters (the CRP level, CRP/Alb ratio, and NLR) and SSNHL.
Patients and Methods
Patients
We reviewed 169 patients diagnosed with SSNHL at our hospital from January 2018 to July 2019. The inclusion criteria were as follows: (1) hearing loss exceeding 30 dB at a minimum of 3 consecutive frequencies developing within 72 hours, (2) no otitis media or other acute or chronic disease, and (3) no smoking or alcohol consumption. The control group included 132 cases diagnosed with small vocal cord polyps from January to December 2019; patients complained of excessive phonation. We excluded those with acute or chronic disease and those who smoked and consumed alcohol. The time to evaluation after SSNHL onset ranged from 1 day to 5 months: 0 to 3 days in subgroup 0, 4 to 7 days in subgroup 1, 8 to 15 days in subgroup 2, 16 to 30 days in subgroup 3, and >30 days in subgroup 4.
Audiometric Evaluation
The World Health Organization divides hearing loss into 5 levels: mild (26-40 dB), moderate (41-55 dB), moderately severe (56-70 dB), severe (71-90 dB), and profound (>90 dB).
Treatment
Of the 169 patients, 55 were all managed via vasodilation, prescription of neurotrophics and a corticosteroid regimen, daily intravenous infusion of 0.9% (wt/vol) normal saline (250 mL) with 70 mg of Ginkgo biloba extract, daily intravenous dexamethasone injection (10 mg, reduced 3 days later to 5 mg), and daily intravenous infusion of 0.9% (wt/vol) normal saline (100 mL) with mecobalamin (0.5 mg). The remaining patients who also chose other therapies were excluded. The treatment time was 7 to 10 days. Pure-tone audiometry (PTA) was performed every 3 days. The outcomes were (1) complete recovery (final hearing loss ≤25 dB or follow-up PTA data returning to within 10 dB of the pre-SSNHL levels or that of the unaffected ear), (2) partial recovery (hearing gain ≥15 dB or follow-up PTA data returning to within 50% of the pre-SSNHL level or that of the unaffected ear), or (3) no recovery (hearing gain <15 dB or follow-up PTA data returning to less than 50% of the pre-SSNHL levels or that of the unaffected ear). We termed patients exhibiting complete and partial recovery “recovered” and the others “unrecovered”.
Hematological Examinations
Blood samples were obtained when patients visited the hospital (before treatment). We recorded the neutrophil and lymphocyte counts and the CRP and Alb levels.
Data Analysis
SPSS ver. 17.0 software was used for analysis. The χ2 test was employed to assess the sex balance of the 2 groups. The independent-samples t test was used to compare age, the CRP level, the CRP/Alb ratio, and the NLR between the groups. We employed an analysis of variance to compare differences in these parameters over time after onset, the hearing levels, and differences between recovered and unrecovered patients and controls. A P value <.05 was considered significant.
Results
The mean ages were 46.69 ± 16.76 years and 44.79 ± 11.19 years in the SSNHL and control groups, respectively. In total, 80 SSNHL patients were male and 89 were female; 58 control patients were male and 74 were female. Neither age nor the sex balance differed significantly between the groups (both P > .05). The number of patients was 75 in subgroup 0, 54 in subgroup 1, 18 in subgroup 2, 8 in subgroup 3, and 14 in subgroup 4. The number of patients with mild hearing loss was 62, 30 with moderate hearing loss, 17 with moderately severe hearing loss, 37 with severe hearing loss, and 23 with profound hearing loss. Thirty-seven patients recovered or had partial recovery and 18 patients did not recover.
The CRP level, CRP/Alb ratio, and NLR were higher in SSNHL patients than controls, but only the NLR difference was statistically significant (Table 1). After SSNHL onset, the 3 parameters changed only slightly. The CRP level and CRP/Alb ratio of group 4 (more than 30 days after SSNHL onset) were highest and differed significantly from those of all other groups except group 3. The control NLR was lower and differed significantly from the SSNHL NLR (Figure 1). The levels of the 3 markers did not differ significantly in the groups of different hearing levels (Figure 2). In patients who underwent vasodilation, neurotrophic, and corticosteroid therapy, the 3 parameters were somewhat higher in unrecovered than recovered patients, but statistical significance was not attained (Figure 3).
Comparison of CRP, CRP/Alb, and NLR of the SSNHL Patients and the Control Group.
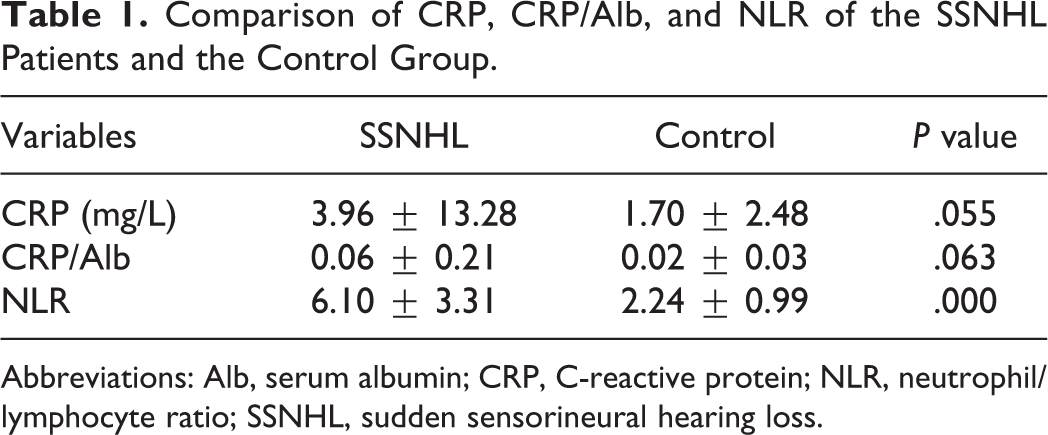
Abbreviations: Alb, serum albumin; CRP, C-reactive protein; NLR, neutrophil/lymphocyte ratio; SSNHL, sudden sensorineural hearing loss.
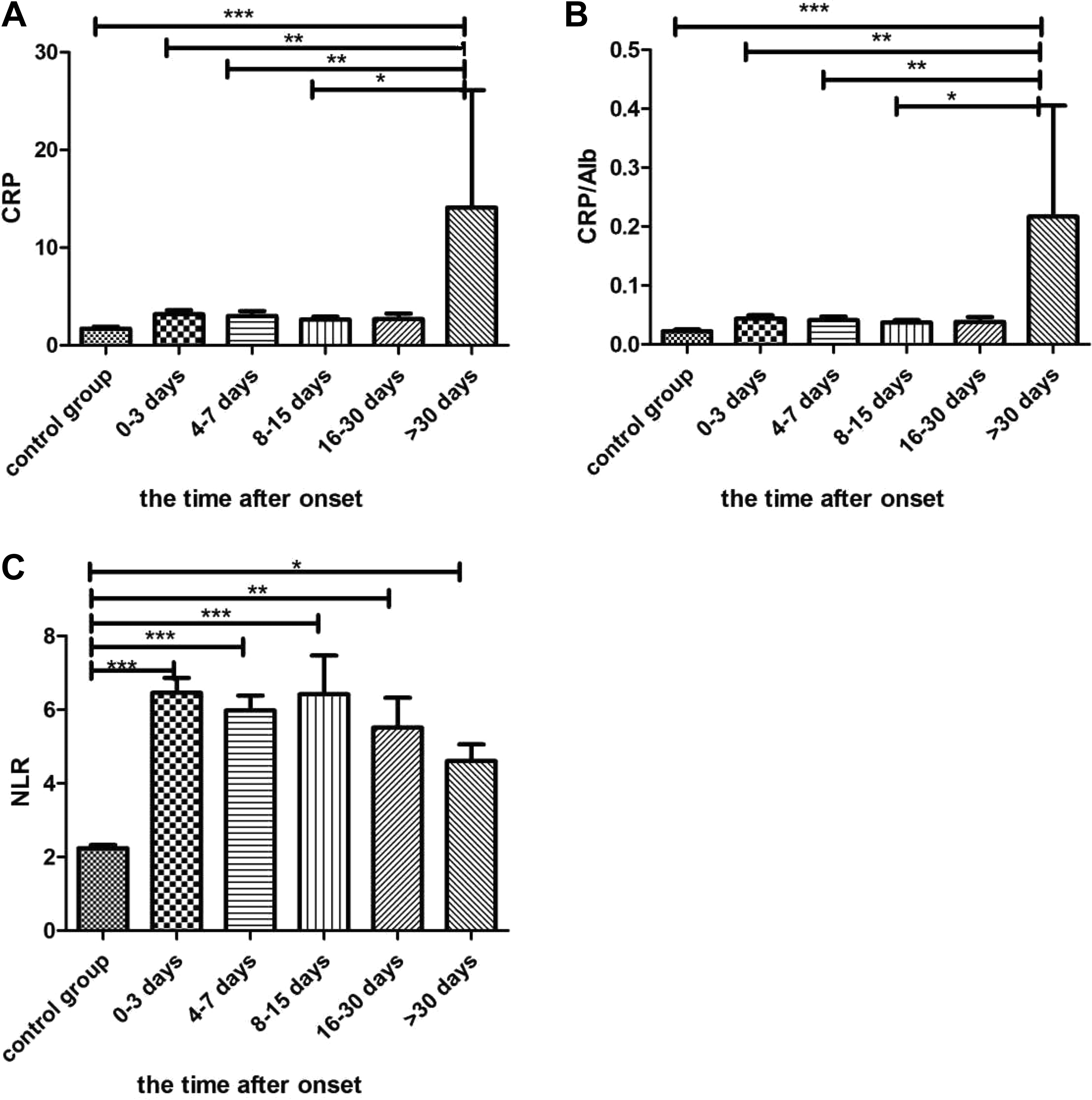
The comparison of the groups of different time after onset of sensorineural hearing loss (SSNHL) and control group. A, The value of C-reactive protein (CRP) in group 4 (more than 30 days) was higher and had significant differences with that in other groups except group 3 (16-30 days). B, The value of CRP/serum albumin (Alb) in group 4 was also higher and had significant differences with that in other groups except group 3 (16-30 days). C, The value of neutrophil/lymphocyte ratio (NLR) in the control group was lower and had significant differences with that in other groups. ***P < .001. **P < .01. *P < .05.
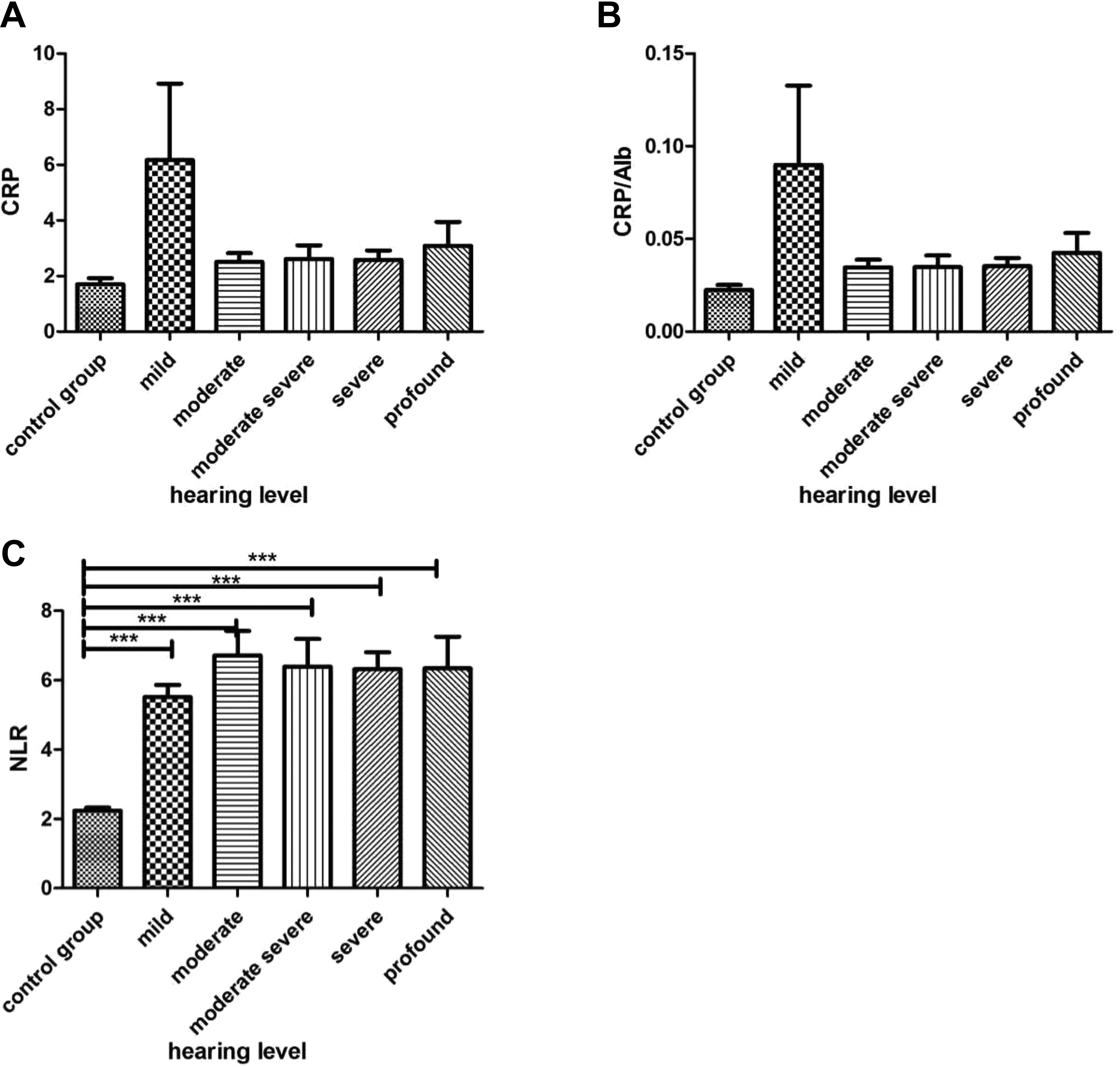
The comparison of groups of different hearing levels and control group. A, The values of C-reactive protein (CRP) had no difference in each groups. B, The values of CRP/serum albumin (Alb) also had no difference in each groups. C, The value of neutrophil/lymphocyte ratio (NLR) in the control group was lower and had significant differences with that in other groups. ***P < .001.
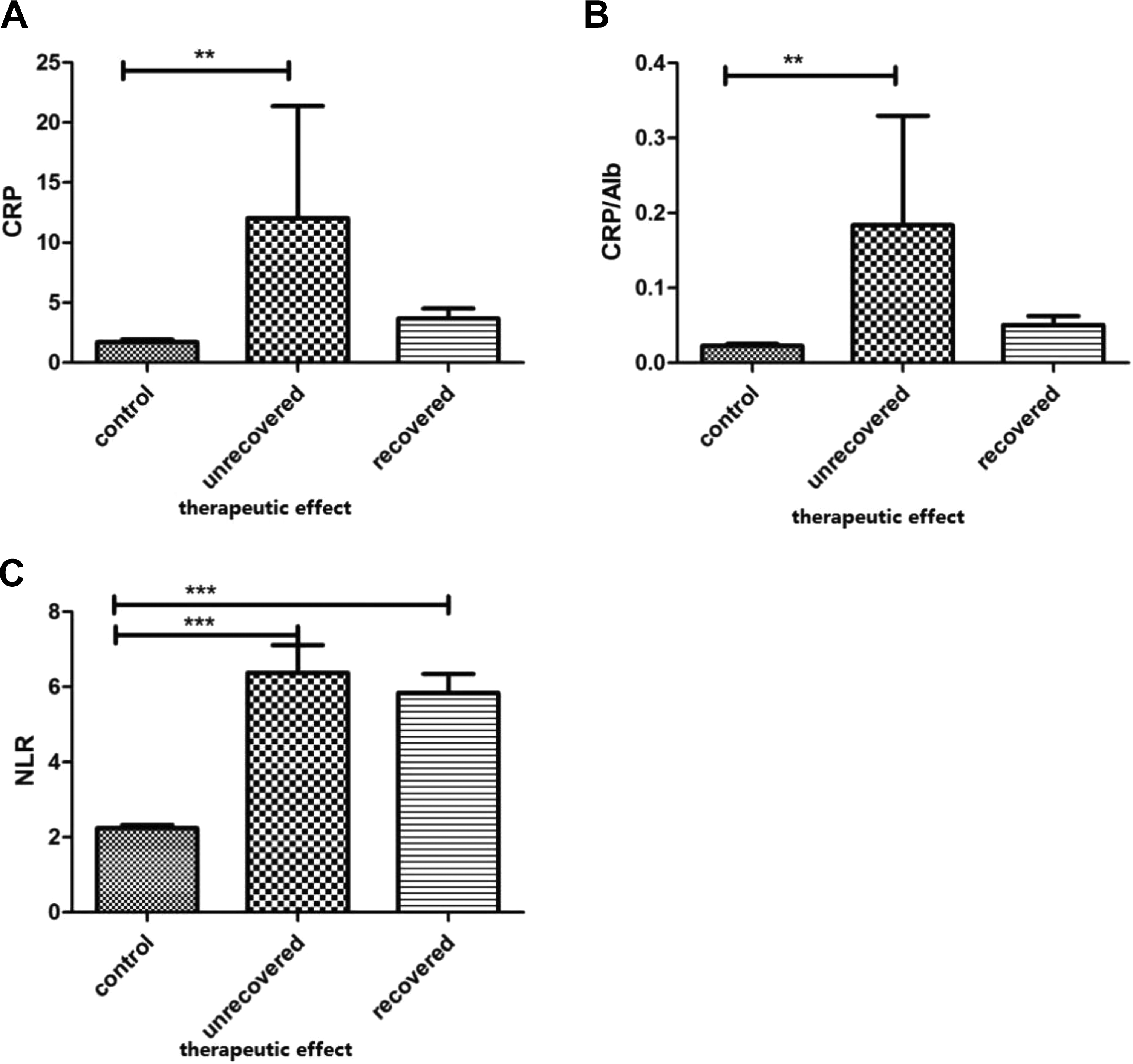
The. The comparison of groups of different therapeutic effects and control group. A, The value of C-reactive protein (CRP) in unrecovered group was higher and had significant difference with the value in the control group but had no difference with that in recovered group. B, The value of CRP/serum albumin (Alb) in unrecovered group was also higher and had significant difference with the value in the control group but had no difference with that in recovered group. C, The value of neutrophil/lymphocyte ratio (NLR) was lower in the control group and had significant differences with the values in the other 2 groups. ***P < .001. **P < .01.
Discussion
The level of CRP (an acute phase reactant) increases with inflammation. 15 In previous studies, the level was associated with the risk of cardiovascular disease. 16 Some authors have suggested that CRP is associated with SSNHL and that inflammation causes SSNHL, but the results are conflicting. Compared to healthy (septoplasty) patients, the CRP level was somewhat higher in SSNHL patients, but the difference was not significant. The CRP level did not reflect SSNHL prognosis, the extent of hearing loss, or the PTA results. 13 We found that the CRP level was not associated with the time to treatment after disease onset or the extent of hearing loss. Although the CRP levels were somewhat higher in SSNHL patients and those who did not recover, the differences were not statistically significant. The CRP/Alb analyses yielded similar results. Serum albumin is thought to be a prognostic marker of infection and inflammation; the level decreases in the acute phases. 17,18 The CRP/Alb ratio is high in patients with inflammatory diseases and cancer. 19 -21 However, in SSNHL patients, the CRP/Alb ratio did not differ significantly from that of controls or between patients who recovered and not. Neither the CRP level nor the CRP/Alb ratio is a useful marker for SSNHL patients.
Unlike the CRP data, the NLR results were consistent. A systematic review and meta-analysis showed that the NLR of SSNHL patients was much higher than that of healthy subjects and was an independent risk factor for the improvement of hearing. 22 We found that the NLR differed significantly between SSNHL patients and controls, but not by the time after disease onset, the extent of hearing loss, or the outcomes of treatment. Neutrophils are nonspecific inflammatory mediators of the first line of defense; lymphocytes are regulatory cells that protect against inflammation. 23 The NLR has been suggested to be a reliable marker of cancer and cardiovascular and inflammatory diseases. 11 The NLR is also a reliable marker of SSNHL. The NLR increased in SSNHL patients, perhaps supporting the hypothesis that inflammation plays an important role in SSNHL pathogenesis.
Previous studies examined changes in the CRP level and NLR by the time after treatment. 24,25 We studied these parameters from disease onset (prior to treatment); both the CRP level and CRP/Alb ratio were highest in patients who visited the hospital more than 30 days after disease onset, suggesting that these parameters increase over time without treatment. However, the NLR did not change significantly over time, although a downward trend was apparent.
Other parameters including platelet numbers, the mean platelet volume, and the platelet/lymphocyte ratio (PLR) have been evaluated in diagnostic/prognostic contexts. 26,27 Platelets play major roles in thrombosis and coagulation and secondary roles in inflammation and cancer. 28,29 Platelets release many components that increase vascular permeability and platelet aggregation, thus promoting inflammation. 30 For SSNHL, however, the NLR was more reliably predictive of onset and prognosis than was the PLR. 22
In conclusion, only the NLR was significantly elevated in SSNHL patients compared to controls. When stratified by time since symptom onset, the CRP level and CRP/Alb ratio were significantly elevated in those with prolonged symptoms. Elevations in all 3 parameters correlated with failure to recover, but no parameter differed significantly between subgroups with different hearing levels or outcomes. The NLR is a reliable marker of SSNHL diagnosis, but not prognosis. The CRP level and CRP/Alb ratio are not useful indicators.
Footnotes
Authors’ Note
All authors contributed to the conception and design of the study. Material preparation, data collection, and analysis were performed by Yan Guo. The first draft of the manuscript was written by Yan Guo. Jisheng Liu commented on early versions of the manuscript. All authors read and approved the final manuscript. This study was approved by the Ethics Committee of the First Affiliated Hospital of Soochow University (approval no. 2020-022).
Acknowledgments
We sincerely thank all of our colleagues for their cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Jiangsu Provincial Key Research and Development Program (BE 2019670). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.