
Abstract
Introduction
Intralabyrinthine schwannoma is a rare, slow-growing, benign tumor that affects the most terminal portions of the vestibular and cochlear nerves. It can be located in the vestibule, cochlea, or semicircular canals.
In 2004, Kennedy et al proposed a classification system which recognized 7 subtypes of intralabyrinthine schwannoma; in 2013, Abel et al 1 modified the Kennedy classification, 2 which included intracochlear, intravestibular (IV), intravestibulocochlear, transmodiolar, transmacular, transotic, and tympanolabyrinthine, to also include translabyrinthine, tumors extending into the CPA, and tumors not otherwise specified. They also proposed to rename intralabyrinthine schwannoma as primary inner ear schwannoma to permit clear subsite categorization.
Patients usually have nonspecific symptoms, including hearing loss, tinnitus, and only single episode of vertigo. Among the resulting symptoms, the most frequent is hearing loss, which affects 95% of the patients. Most times, this loss is slow and progressive, but it may be sudden or fluctuating. Less common symptoms include tinnitus (51%), imbalance (35%), vertigo (22%), and ear fullness (2%), which may be present alone or in combination.3-7 We report a rare case of a patient with hearing loss and single episode of vertigo secondary to the intralabyrinthine schwannoma of the IV subtype.
Case Presentation
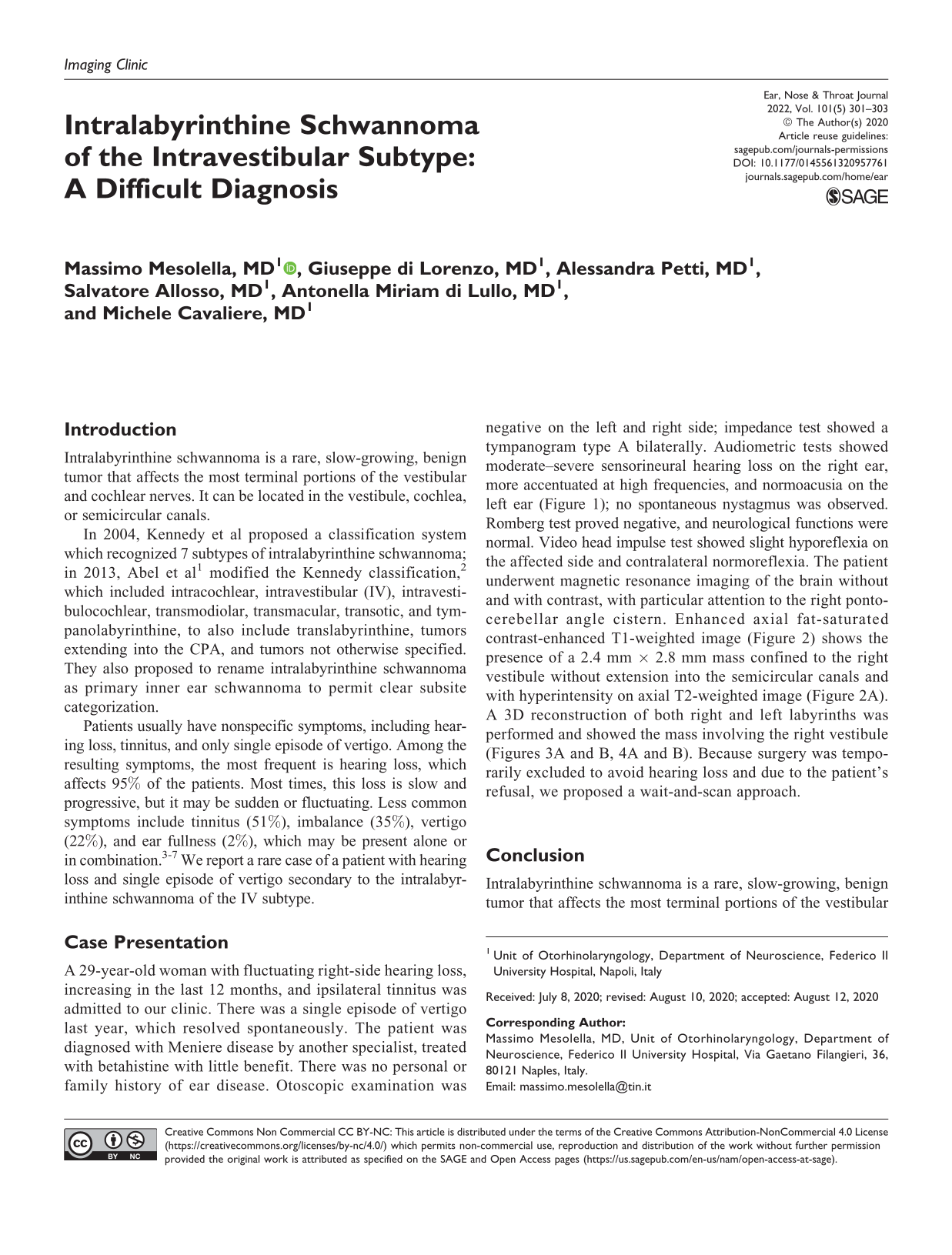
A 29-year-old woman with fluctuating right-side hearing loss, increasing in the last 12 months, and ipsilateral tinnitus was admitted to our clinic. There was a single episode of vertigo last year, which resolved spontaneously. The patient was diagnosed with Meniere disease by another specialist, treated with betahistine with little benefit. There was no personal or family history of ear disease. Otoscopic examination was negative on the left and right side; impedance test showed a tympanogram type A bilaterally. Audiometric tests showed moderate–severe sensorineural hearing loss on the right ear, more accentuated at high frequencies, and normoacusia on the left ear (Figure 1); no spontaneous nystagmus was observed. Romberg test proved negative, and neurological functions were normal. Video head impulse test showed slight hyporeflexia on the affected side and contralateral normoreflexia. The patient underwent magnetic resonance imaging of the brain without and with contrast, with particular attention to the right pontocerebellar angle cistern. Enhanced axial fat-saturated contrast-enhanced T1-weighted image (Figure 2) shows the presence of a 2.4 mm × 2.8 mm mass confined to the right vestibule without extension into the semicircular canals and with hyperintensity on axial T2-weighted image (Figure 2A). A 3D reconstruction of both right and left labyrinths was performed and showed the mass involving the right vestibule (Figures 3A and B, 4A and B). Because surgery was temporarily excluded to avoid hearing loss and due to the patient’s refusal, we proposed a wait-and-scan approach.
Audiometric tests showed moderate–severe sensorineural hearing loss more accentuated at high frequencies on the right ear and normoacusia on the left ear.
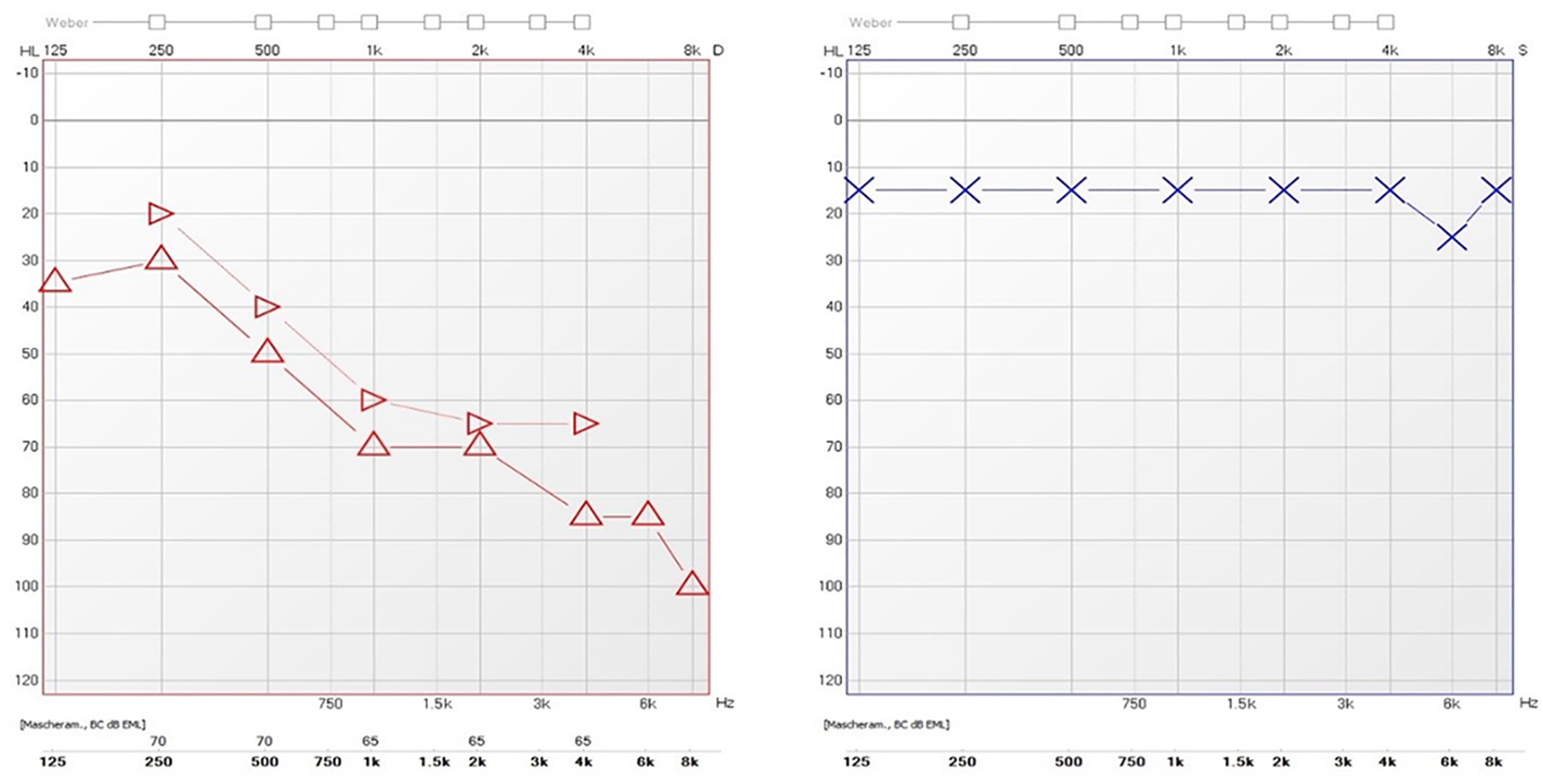
Video Head Impulse Test (vHIT) showed slight hyporeflexia on the right (affected) side and normo-reflexia on the left side (B) in a our patient with unilateral vestibular loss (UVL) compared with a healthy subject (A).
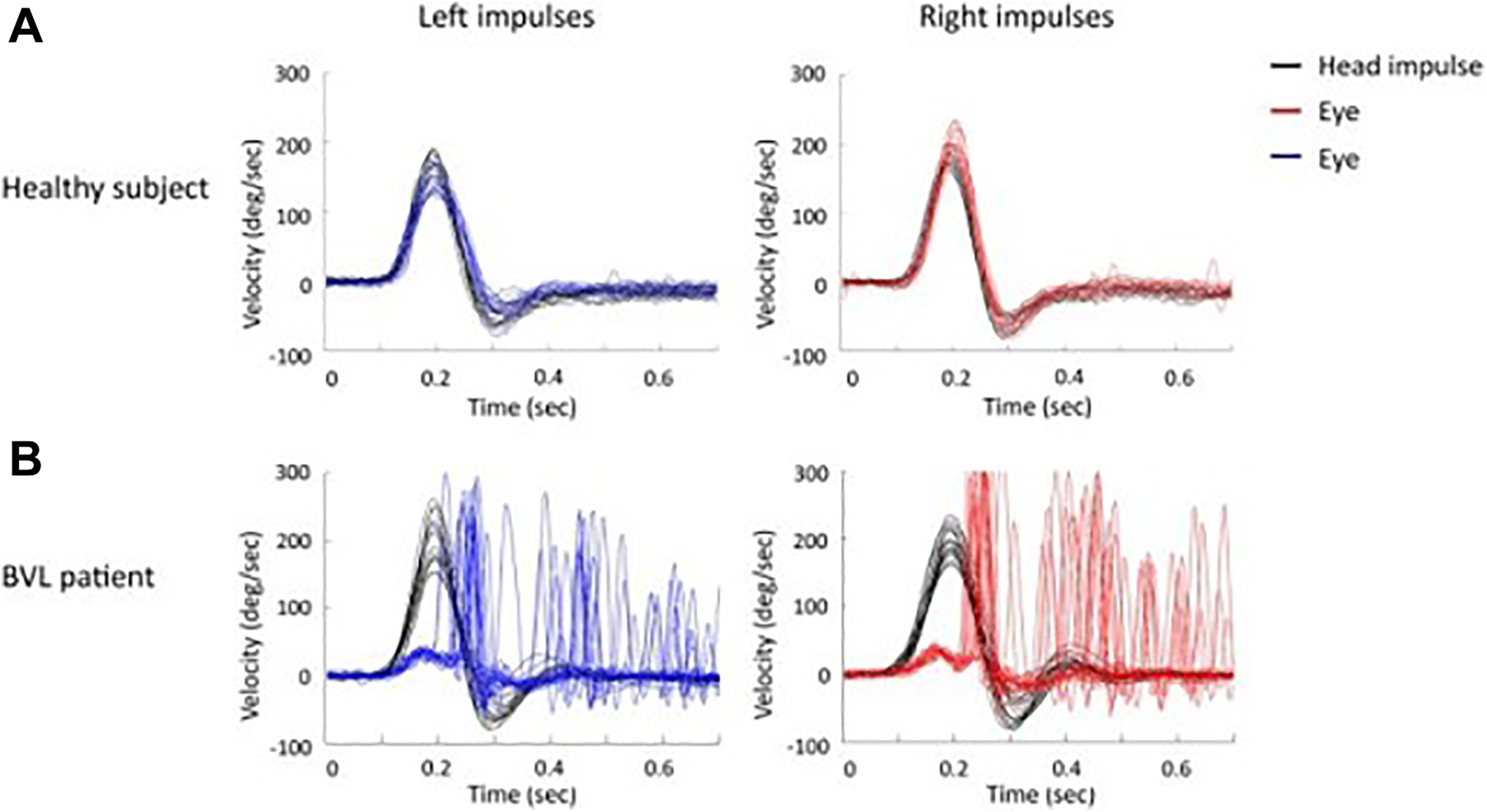
Magnetic resonance imaging of the brain without and with contrast, with particular attention to the right pontocerebellar angle cistern. Enhanced axial fat-saturated contrast-enhanced T1-weighted image (B) shows the presence of a 2.4 mm × 2.8 mm mass confined to the right vestibule without extension into the semicircular canals and with hyperintensity on axial T2-weighted image (A).
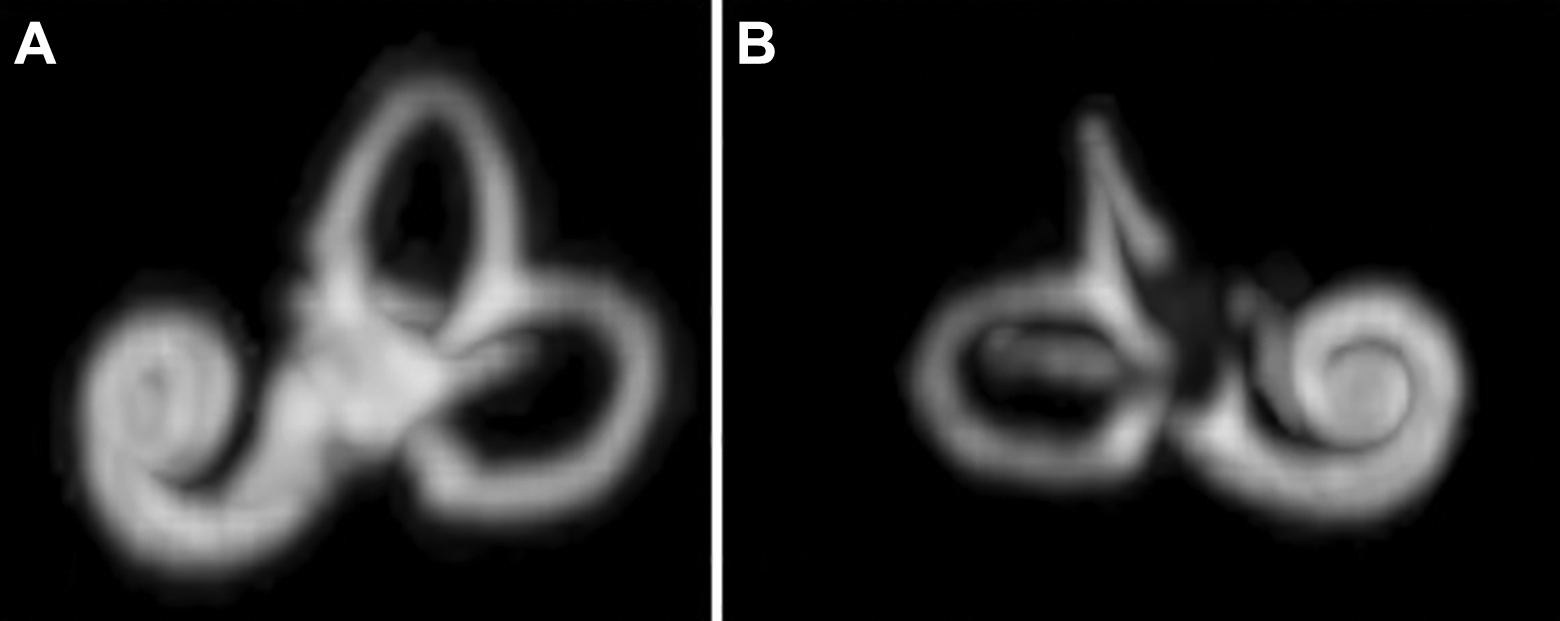
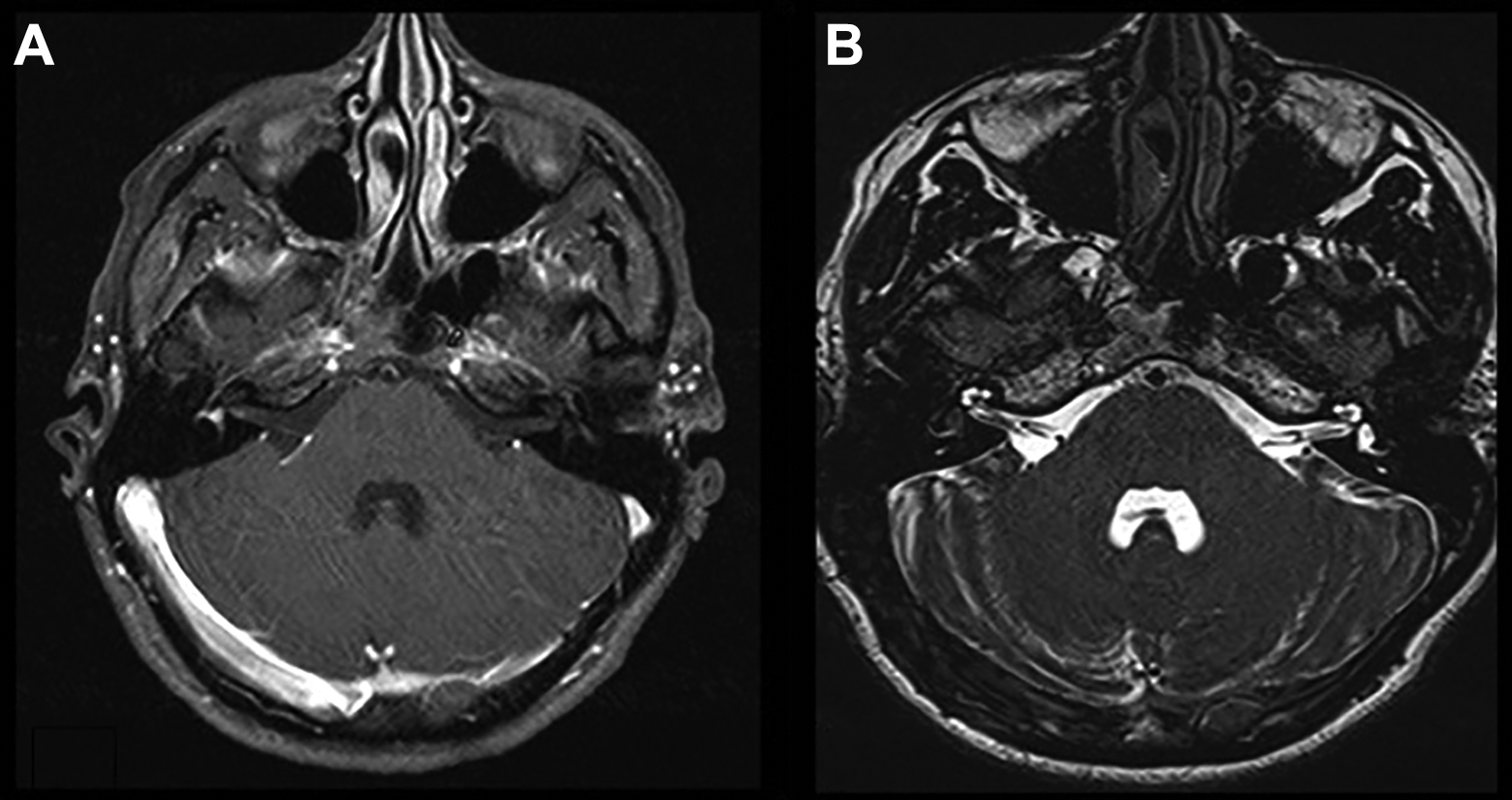
A 3D reconstruction of both right (B) and left labyrinths (A). The examination showed the mass involving the right vestibule (B).
Conclusion
Intralabyrinthine schwannoma is a rare, slow-growing, benign tumor that affects the most terminal portions of the vestibular and cochlear nerves. It can be located in the vestibule, cochlea, or semicircular canals.
The reported case is rare and atypical. It presents an onset symptomatology of the disease with almost exclusive pathological manifestations of the cochlear component (hearing loss) and a very mild and nonspecific vestibular symptomatology (only a very mild episode of objective vertigo). The differential diagnostic difficulty was also given by the fact that the hearing loss presented fluctuation characteristics typical of Meniere disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.