
Abstract
Purpose:
This study was designed to investigate whether preoperative embolization is a useful procedure to decrease blood loss and neurovascular complications for carotid body tumor (CBT) surgery or not.
Methods:
Medical records of our tertiary care center from 2012 to 2019 were scanned for patients who underwent surgery for CBT, retrospectively. Age, gender, complaint and head and neck examination findings at the time of presentation, preoperative complete blood count parameters, imaging records (cervical magnetic resonance imaging and carotid artery angiography), Shamblin classification, tumor size, intraoperative findings, and postoperative complications were noted.
Results:
A total of 26 patients were operated due to CBT between 2012 and 2019 in our clinic; preoperative arterial embolization was performed to 15 (57.7%) patients, and 11 (42.3%) patients were operated without embolization. Youngest patient was 24 years old, while oldest was 69 years and mean age was 44.35 ± 12.73. (embolization group: ages ranging between 24 and 64 with a mean of 41.5 ± 11.02 years; in nonembolization group: ages ranging between 26 and 69 with a mean of 48.1 ± 14.3). Embolization status was not significantly related to cranial nerve injury, vascular injury, overall complications, and hematocrit decrease. Arterial injury is more likely to occur with increasing Shamblin class (r = .39; P = .04). Tumor size is not found to be significantly related to cranial nerve injury, vascular injury, overall complications, and hematocrit decrease, but cranial nerve injury and vascular injury were more likely to occur in large tumors (r = .34; P = .089 and r = .34; P = .087, respectively). Age was significantly and negatively correlated to vascular injury (r = −.51; P = .05). Vascular injury was significantly correlated with gender (male predominance: r = −.64; P = .000).
Conclusion:
Although preoperative arterial embolization is considered to attenuate the complication risk, we found that there was no significant difference among the patients with or without embolization.
Introduction
Paragangliomas are neuroendocrine tumors of autonomic nervous system that are derived from extraadrenal paraganglia. 1 Most common site for paragangliomas is abdomen by far (85%), thorax is the second (12%), and least common site is head and neck (3%). 2 Head and neck paragangliomas constitutes less than 0.5% of all head and neck tumors and approximately 0.03% of all human tumors. 3 Head and neck paragangliomas are named according to their site of origin (eg, carotid body, jugular, vagal, tympanic, etc), and carotid body tumor (CBT) is the most frequent head and neck paraganglioma with a rate of 60% to 78%. 4 Although being mostly benign, malignancy rate of 6% to 10% is reported for CBT.1,2
Surgery is considered the primary and definitive treatment, although in some cases total resection may cause significant morbidity due to involvement of critical neurovascular structures and resulting in complications like stroke, blood loss, cranial nerve paralysis, and aspiration pneumonia. 5 There are many suggested theories to foresee the likelihood of complications to occur, most prominent of them being the Shamblin classification. 6 While class I/II tumors can easily be resected, class III tumors are difficult to be extirpated without complications.6,7 A common finding of studies is the 10- to 15-fold increase of neurovascular complications with class III tumors when compared to class I/II.8-10
Tumor size is also considered as an important risk factor for complications. It has been put forward that with the increasing size of the tumor, risk of arterial injury and cranial nerve paralysis also increases. 11 Patient age with the addition of comorbid diseases is reported to be related with increased complication rates and that is why it can affect the decision whether to perform surgery. Insomuch as, some of the authors suggest that patients older than 60 years with CBT should not be operated on unless proven malignant.10,12
A conflict of whether to perform preoperative arterial embolization or not is still ongoing. While one large scale meta-analysis is putting forth that preoperative embolization reduces blood loss and duration of surgery, 13 another meta-analysis advocates that there is no significant difference 7 ; but most of the meta-analyses reach on a consensus about that the preoperative embolization does not affect the rate of neurovascular complications.7,13,14
In this study, we investigated the relationship between the age, gender, tumor size, Shamblin classification, preoperative embolization, and neurovascular complications or blood loss by reviewing our archives for patients who had undergone carotid body surgery in our clinic in past 8 years. Also, we compared the patients with or without preoperative embolization for different surgical parameters to present whether the preoperative embolization is necessary or not.
Materials and Methods
Patient Data
Medical records of our tertiary care center from 2012 to 2019 were scanned for patients who underwent surgery for CBT, retrospectively. Age, gender, complaint and head and neck examination findings at the time of presentation, preoperative complete blood count parameters, imaging records (both carotid artery angiography and cervical magnetic resonance imaging for all patients), Shamblin classification, tumor size, intraoperative findings, and postoperative complications were noted. Complications were classified as vascular injury, cranial nerve injury, and overall vascular and cranial nerve injuries. In order to evaluate intraoperative blood loss, we used preoperative and postoperative first day hematocrit levels. Whether preoperative arterial embolization was performed or not was also noted for all patients. Patients with intraoperative arterial injury or postoperative cranial nerve paralysis were further investigated whether there was a relationship between age, gender, tumor size, Shamblin classification, and preoperative arterial embolization.
Surgical Technique
Preoperative arterial embolization was done with carotid artery angiography through transfemoral approach while patient is awake. A 5F diagnostic catheter was used for the procedure. First, diagnostic contrast injection was done to determine the arterial feeders to the tumor. Then a microcatheter was advanced through diagnostic catheter into the selective branches. Embolization was performed using polyvinyl alcohol particles. A final angiogram was performed to evaluate the adequacy of embolization and patency of internal carotid artery. Surgery was scheduled within 24 to 48 hours after the embolization.
All of the patients were operated on under general anesthesia. Following an approximately 5 cm long semihorizontal incision, sternocleidomastoid muscle was lateralized, internal jugular vein was identified, and again lateralized and common carotid artery was exposed. Proximal end of the common carotid artery and distal ends of both the external and internal carotid arteries were secured before starting dissection of the tumor. Bipolar cautery was used in combination with scissors for surgical dissection, and dissection was done in the subadventitial plane as first described by Gordon-Taylor 15 in 1940. All surgeries were performed by experienced head and neck surgeons. In the case of a strictly adherent tumor, participation of a vascular surgeon was requested. Diagnosis was confirmed with histopathological examination for all cases.
Statistical Analysis
The statistical analysis was done with SPSS 21 program. The comparisons between the demographic data, tumor size and side, Shamblin classification, cranial nerve and vascular injury, and status of preoperative embolization were done with Mann-Whitney U test. Correlation analysis between the embolization status, age, gender, complications, Shamblin classification, tumor size, and hematocrit decrease is done with chi-square test and Spearman correlation analysis. A P value <.05 was considered significant.
Ethical Considerations
Informed consent was obtained from all of the patients before surgery took place. Study design has been submitted for approval of ethics committee, and examination of medical records was started after approval. There is no disclosure of personal information and images of patients in this article.
Results
The demographic information, tumor size and side, embolization status, Shamblin classification, status of preoperative embolization, complications, and comparison of the data are presented in Table 1. A total of 26 patients were operated due to CBT between 2012 and 2019 in our clinic; preoperative arterial embolization was performed to 15 (57.7%) patients, and 11 (42.3%) patients were operated without embolization. Eighteen of the patients were female (69.2%), while 8 of them were male (30.8%; male/female in embolization group: 5/10; male/female in nonembolization group: 3/8). Youngest patient was 24 years old, while oldest was 69 years and mean age was 44.35 ± 12.73 (embolization group: ages ranging between 24 and 64 with a mean of 41.5±11.02 years; in nonembolization group: ages ranging between 26 and 69 with a mean of 48.1 ± 14.3). In 57.7% of the patients (n = 15), tumor was right sided and in 42.3% (n = 11), tumor was located on the left side (right/left in embolization group: 11/4; right/left in nonembolization group: 4/7). The difference between the ages, genders, and the side of the patients with or without preoperative embolization was not significant (Table 1).
The Demographic Information, Tumor Size and Side, Embolization Status, Shamblin Classification, Status of Preoperative Embolization, Complications, and Comparison of the Data According to the Embolization Status.a
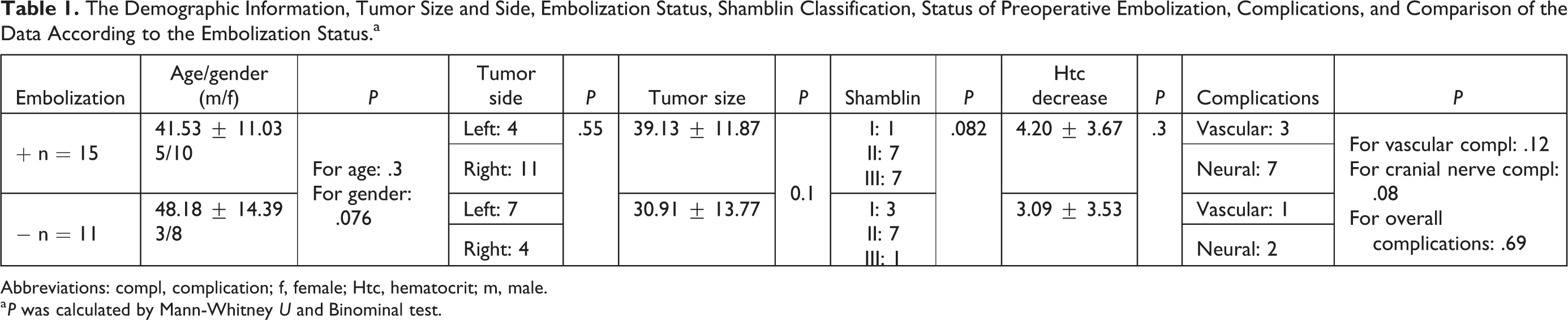
Abbreviations: compl, complication; f, female; Htc, hematocrit; m, male.
a P was calculated by Mann-Whitney U and Binominal test.
Mean tumor size was 35.65 ± 13.12 mm, with a range between 13 and 63 mm; 15.4% (n = 4) of the tumors were classified as class I according to Shamblin classification, while 53.8% (n = 14) of them were class II and 30.8% (n = 8) were class III (in embolization group, the size of the tumor was ranging between 17 and 60 mm with a mean of 39.1 ± 11.8mm; and in nonembolization group, the size was ranging from 13 to 63 mm with a mean of 30.9 ± 13.7 mm; Shamblin classification of embolization group; I: 1, II: 7, III: 7; and Shamblin classification of nonembolization group: I: 3, II: 7, III: 1; Table 1).
Hematocrit decrease ranged from 0 to 13, with a mean of 3.73 ± 3.58. The hematocrit decrease of the patients without preoperative embolization was ranging between 0 and 11 with a mean of 3.09 ± 3.5, whereas hematocrit decrease of the patients with preoperative embolization was ranging between 0 and 13 with a mean value of 4.2 ± 3.6, the difference being nonsignificant (Table 1).
Complication rate was 42.3% (n = 11); 7.7% (n = 2) was arterial injury, 26.9% (n = 7) was cranial nerve paralysis, and 7.7% (n = 2) of the patients had both arterial injury and cranial nerve paralysis. In total, 4 of the patients had arterial injury and necessitated the participation of vascular surgery team. Primary repair was sufficient for 2 of 4, while remaining 2 underwent saphenous vein grafting. These 2 patients who underwent grafting had also cranial nerve complication. All of the cranial nerve injuries included vagus nerve (n = 4) and hypoglossus (n = 3). In preoperative embolization group, the total number of complications was 9; vascular injury in 2 patients, cranial nerve injury in 6 patients, and both cranial nerve and vascular injury in 1 patient. In preoperative nonembolization group, there were a total of 2 complications one of which was vascular injury and the other was both vascular injury and cranial nerve injury. The comparisons of cranial nerve injury, arterial injury, and overall complication rates among the patients with or without preoperative embolization were statistically nonsignificant (Table 1).
Correlation results are presented in Table 2. There were 11 patients for whom preoperative embolization was not performed, 2 of them had cranial nerve injury, with 1 of them also had arterial injury. In the group that preoperative embolization was performed (n = 15), 2 had arterial injury, 6 had cranial nerve injury, and 1 had both. Embolization status was not significantly related to cranial nerve injury, vascular injury, overall complications, and hematocrit decrease (Table 2).
Correlation Analysis Between the Embolization Status, Age, Gender, Complications, Shamblin Classification, Tumor Size, and Hematocrit Decrease Are Presented.a
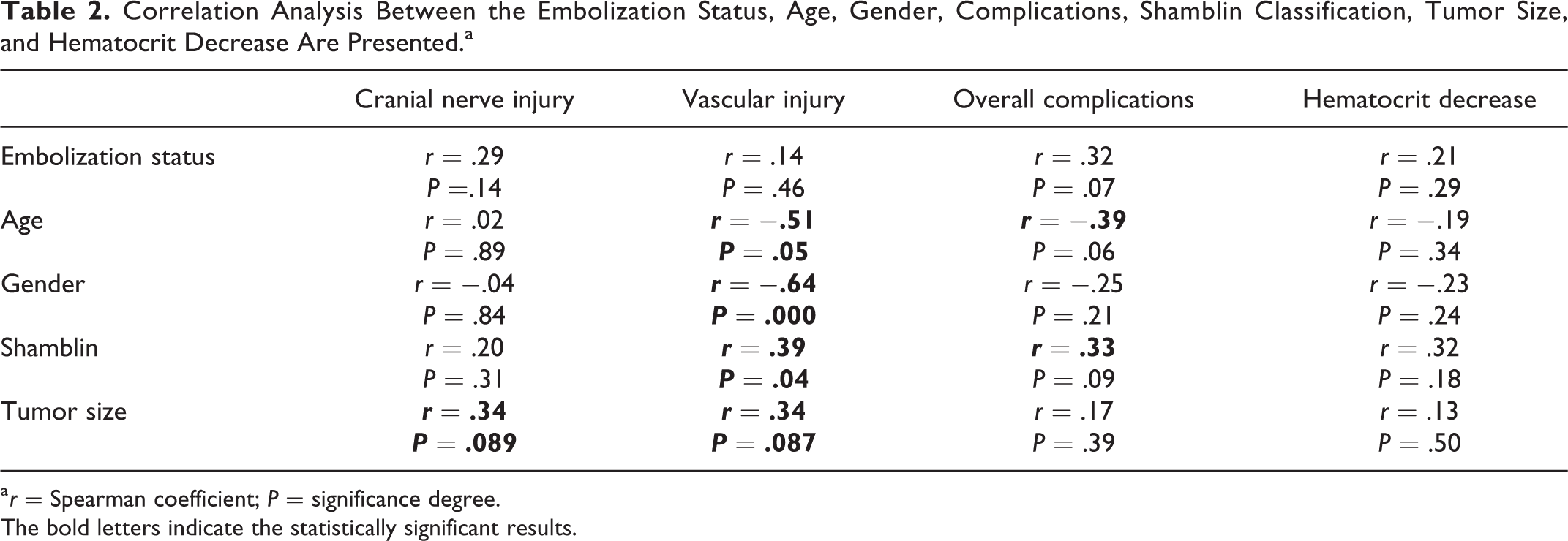
a r = Spearman coefficient; P = significance degree.
The bold letters indicate the statistically significant results.
No significant relationship is found between age and cranial nerve paralysis (r = .02; P = .89), hematocrit decrease (r = −.19; P = .34), or overall complications (r = −.39; P = .06). However, age was significantly correlated to vascular injury (r = −.51; P = .05). Although there was no significant relationship between gender and cranial nerve injury, overall complications, and hematocrit decrease rates, vascular injury was significantly correlated to gender (male predominance: r = −.64; P = .000; Table 2).
Tumor size is not found to be significantly related to cranial nerve injury, vascular injury, overall complications, and hematocrit decrease but cranial nerve injury and vascular injury were more likely to occur in large tumors (r = .34; P = .089 and r = .34; P = .087, respectively; Table 2).
For Shamblin classification; 1 of 4 patients who had vascular injury was class II, while 3 of them were class III. Arterial injury is more likely to occur with increasing Shamblin class, this difference was found statistically significant (r = .39; P = .04). One of 9 patients who had cranial nerve injury was class I, while 4 of them were class II and 4 were class III; and no significant relationship between Shamblin class and cranial nerve injury was found. Shamblin class was also not found to be significantly related to hematocrit decreases (Table 2).
Discussion
Carotid body tumors are the most frequent head and neck paragangliomas, although they are rare when all head and neck tumors are considered.3,4 Their definitive treatment is surgery in expense of neurovascular complications. 5 The efficacy of angiography and embolization before CBT surgery was first reported by Schick et al. 16 The aim of embolization is to control arterial supply of the tumor and by this way to decrease blood loss, to shorten the operation time, and to decrease overall surgical complications. 17 Since then, there has been a controversy whether to perform preoperative embolization or not and also to whom it must be performed. Although there are no clear guidelines, embolization is generally considered for large tumors or Shamblin class II/III lesions. 18
Reducing the blood loss is one of the main points of the preoperative embolization. This is also considered as a factor to shorten the duration of operation. 19 However, there are studies showing that blood loss and operation time are not affected by whether preoperative embolization was performed or not. 20 Zeitler et al 21 found no significant difference for mean blood loss (305 mL in embolization group vs 265 in nonembolization group) and operation time between the embolization group and nonembolization group; and Law et al 22 stated that curative resection of the tumor was nonetheless same between these 2 groups; while Zhang et al 23 advocated that the preoperative embolization significantly lowers the blood loss (mean blood loss 80 vs 200 mL) and operation time. In a similar manner, Wang et al 24 stated that the preoperative embolization facilitated the total resection of the tumor and significantly reduced the blood loss especially for the medium-sized tumors (3-5 cm). Even there are studies that found higher blood loss in embolization group, although this difference does not reach the level of significance.25,26 In our study, we evaluated postoperative hematocrit change as an indirect indicator of blood loss and found that there was no significant difference between the 2 groups (P = .03). Therefore, our findings agree with the studies, which indicate that preoperative embolization should not be considered as a routine measure to reduce intraoperative blood loss.9,25
It is also hypothesized that preoperative embolization may decrease the risk of vascular and cranial nerve injury, 17 and preoperative angiography has also the advantage of evaluating the adequacy of the Willis polygon anastomoses by performing balloon occlusion test. 27 However, most of the studies showed no significant decrease in the vascular injury 28 as well as cranial nerve injury rates in the groups with preoperative embolization. 29 In a study of Mourad et al, 20 it was stated that tumor embolization did not have any effect on postoperative cranial nerve deficits and major vascular injury and vascular sacrifice; furthermore all vascular and neural complications were seen in Shamblin II/III tumors regardless of embolization status. In a similar manner, in our study, preoperative embolization did not affect the rate of cranial nerve injury (P = .08) and vascular injury (P = .12), as well as overall complication rates (P = .69). Although the difference was statistically nonsignificant, cranial nerve injury and vascular injury were even more frequently seen in the group that embolization was performed. This result can be attributed to edema and inflammation, caused by embolization, which makes tumor dissection difficult. 27
As stated above, one of the main complications of embolization is revascularization edema and inflammation; that is why it is recommended to perform the surgery within 24 to 48 hours after embolization.13,30 Recent studies state that this phenomenon starts even in the very first day after embolization and surgery must be performed in the same day. 31 One of the major risks of preoperative embolization is stroke 32 ; even though Vogel et al 33 found no increased mortality and stroke rates in embolization group. Also, there was no case of stroke due to embolization in our patient group.
There are 3 large scaled meta-analyses and systematic reviews evaluating the efficacy of preoperative embolization in CBT surgery.7,13,14 Common finding of all these reviews was that the rates of vascular and cranial nerve complications are not significantly differed between the embolization and nonembolization groups.7,13,14 Shamblin classification is useful to foresee the probability of vascular and cranial nerve injury. 6 Neurovascular complications mostly occur in the patients with Shamblin class III tumors, as expected. 34 Cranial nerve injuries are more likely to occur with Shamblin III tumors when compared to Shamblin II tumors.35,36 However, Law et al 22 found Shamblin class only useful to predict the blood loss, operation time, and possibility of major vascular reconstruction need but not the rates of complications. Luna-Ortiz et al 37 indicated that the Shamblin classification may only predict vascular injury but not neural complications and even proposed a modification of Shamblin classification. Our findings were also consistent with the literature, and arterial injury was more likely to occur with increasing Shamblin class, with the level of significance (r = .39; P = .04). Again we found no significant relationship between Shamblin class and cranial nerve injury, as with hematocrit decrease (Table 2).
Tumor size was shown to affect the intraoperative blood loss. 34 Although Kollert et al 4 showed no correlation between the tumor size and incidence of cranial nerve palsies; Dardik et al 38 revealed, not Shamblin classification, tumor size predicted cranial nerve injury. We found no significant relation between tumor size and cranial nerve injury, vascular injury, overall complications, and hematocrit decrease, but cranial nerve injury and vascular injury were more likely to occur in larger tumors (r = .34; P = .089 and r = .34; P = .087, respectively; Table 2).
Just opposite to be expected, vascular injury rates were moderately and negatively correlated with age and this correlation was significant (r = −.51; P = .005). Again, vascular injury was significantly higher in males (r = .64; P = .000). This can be explained by prominence of angiogenic and vascularization factors in younger age that makes the resection of paraganglioma harder. The gender difference in complication rates may be attributed to the vascular smooth muscle relaxation effect of estrogen that may cause more elastic vascular wall in females. 39 The vessel walls are stiffer in males and that may predispose to vascular complications in CBT resection. But there is no way to link the increased vascular complication rates to sex hormone differences by the findings of our study. Although most of our findings are consistent with the current literature, still there is a need for randomized controlled trials with large patient population to determine the efficacy of preoperative arterial embolization.
Conclusion
Although preoperative arterial embolization is considered to attenuate the complication risk, we found that there was no significant difference among the patients with or without embolization. Our study also demonstrated that neurovascular complications were not related to age but in contrast, vascular complications were more frequent with decreasing age. A significant finding was the likelihood of vascular injury to occur in male patients. Again, Shamblin class and tumor size parameters were significantly related to vascular complication rates.
Footnotes
Authors’ Note
The data of the study can be shared on demand. The faculty ethics committee approved the study protocol and informed consents were obtained from each patient. All participants were informed and informed consents were retrieved. All the patients and all the authors consented the publication of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.