
Abstract
The odontogenic keratocyst, also known as keratocystic odontogenic tumor, represents 10% of all odontogenic cysts of the jaws. 1 The lesion arises from remnants of the dental lamina, the thickening of odontogenic oral epithelium and the underlying ectomesenchyme of neural crest origin. Histologically, odontogenic keratocyst is characterized by a cystic lumen containing keratin debris, lined by a corrugated parakeratinized squamous epithelium, with a hyperchromatic and palisaded basal cell layer.
Odontogenic keratocyst may develop at any age, although it is most commonly diagnosed in patients during the second and third decades of life. There is a slight male predilection. The lesion affects the mandible at least twice as often as the maxilla. Most mandibular lesions are located in the posterior body and ramus. In the maxilla, however, most lesions are located in the canine area. 2 Occasionally, odontogenic keratocysts develop in association with impacted teeth.
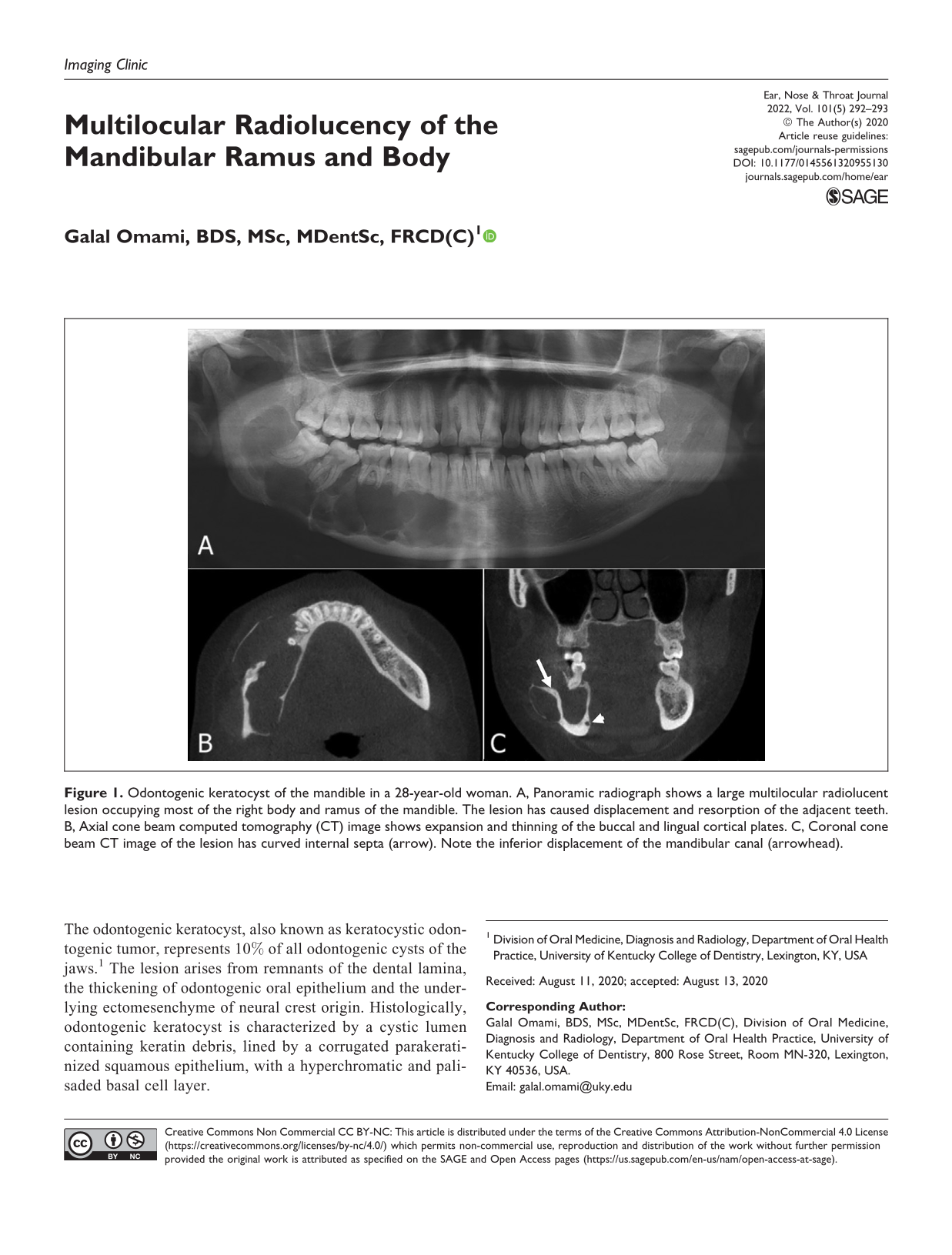
The lesions are either unilocular or, less commonly, multilocular, giving the appearance of a soap bubble pattern (Figure 1). The periphery is usually well defined and corticated and often scalloped in nature. Odontogenic keratocysts often tend to grow along the medullary cavity of the jaws, which causes minimal expansion of the cortical plates considering the overall size of the lesion. Tooth displacement and resorption are infrequently seen. 3
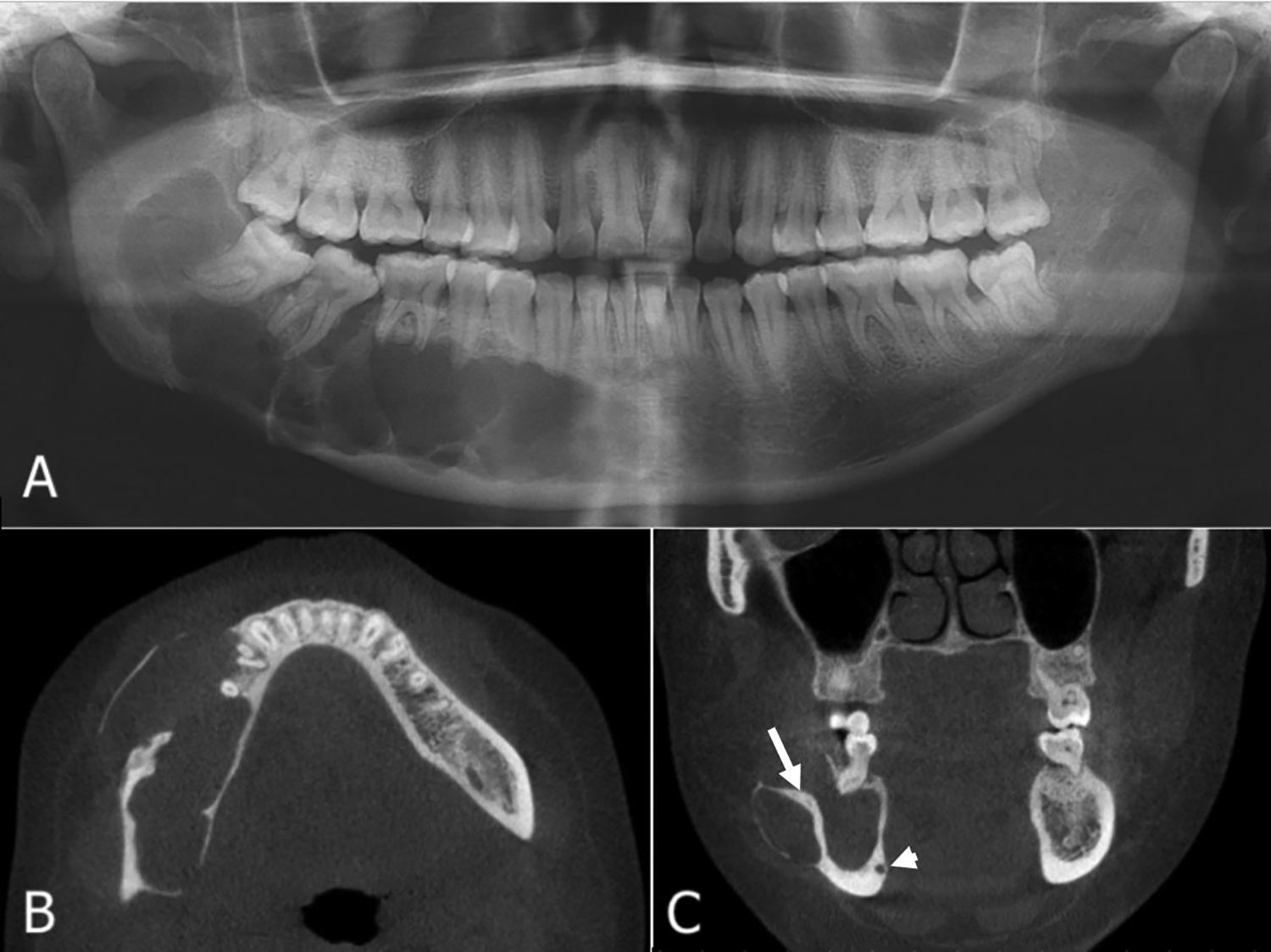
Odontogenic keratocyst of the mandible in a 28-year-old woman. A, Panoramic radiograph shows a large multilocular radiolucent lesion occupying most of the right body and ramus of the mandible. The lesion has caused displacement and resorption of the adjacent teeth. B, Axial cone beam computed tomography (CT) image shows expansion and thinning of the buccal and lingual cortical plates. C, Coronal cone beam CT image of the lesion has curved internal septa (arrow). Note the inferior displacement of the mandibular canal (arrowhead).
Multiple odontogenic keratocysts are associated with nevoid basal cell carcinoma syndrome (Gorlin syndrome), which also comprise multiple basal cell carcinomas of the skin, palmar/plantar pits, calcification of the falx cerebri, and skeletal abnormalities (eg, bifid ribs).
Odontogenic keratocysts are usually treated by thorough surgical curettage, often supplemented with peripheral ostectomy of the bony cavity. Approximately 30% of lesions are reported to recur after treatment. 4
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.