
Abstract
The middle ear bone destruction in chronic otitis media is activated and regulated by inflammation. Chronic otitis media with granulation is a highly active inflammatory process in which many cytokines are released. The bone is degraded by osteoclasts but, at the same time, protected by cytokines, growth factors, adhesion molecules and osteotropic hormones. Tumor necrosis factor-α, interleukin (IL)-1, IL-6, and OPG/RANKL present in cholesteatoma and granulation accelerate bone lysis and increase the destructive effect on the middle ear.
Keywords
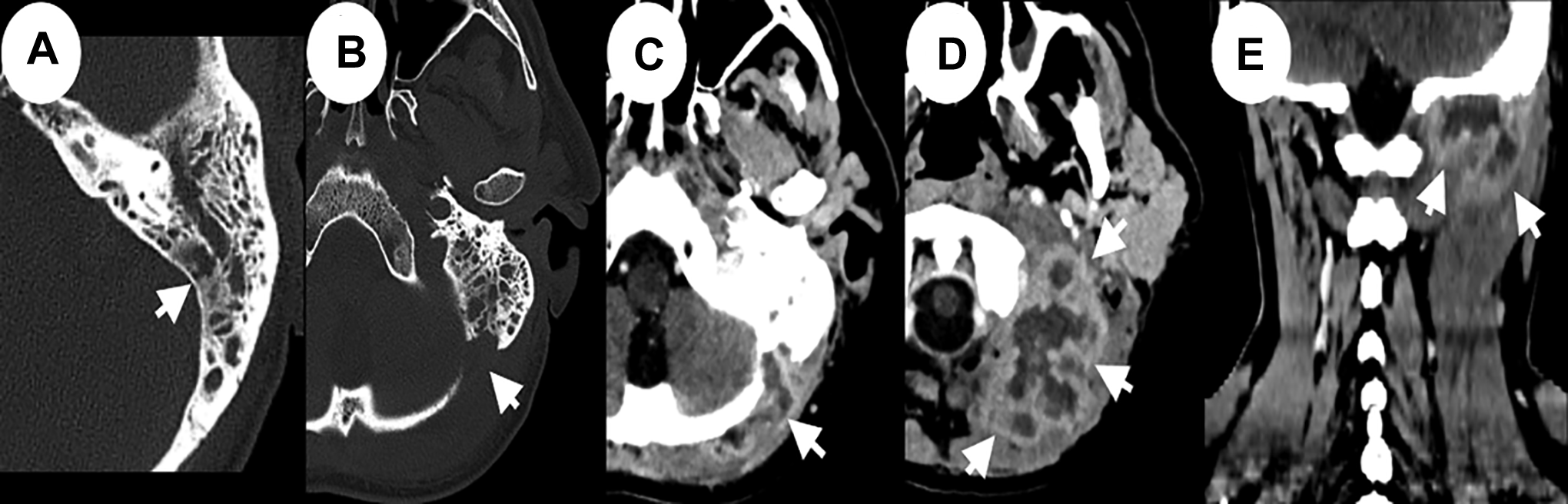
We read with great interest the article, “Patterns of Bone Damage in Patients With Chronic Middle Ear Inflammation” by Wiatr A, Stręk P, Wiatr M. Ear Nose Throat J. 2020. 1 We would like to present some comments on this problem, based on our experience and the literature review. Chronic otitis media (COM) is a disease that causes hearing loss, bone damage, and serious complications. The authors presented a clinical analysis of the destruction of auditory ossicles and bone walls of the middle ear in patients with COM with granulation (COM-G) and cholesteatoma (COM-Ch). In their research, based on 220 patients with COM treated surgically, they stated that destruction of the middle ear bone walls was found in 27 (12%) patients. Bone damage of the middle ear wall was observed more frequently in patients with COM-G than among those with COM-Ch. Furthermore, a very important clinical observation is that COM-G is an unfavorable factor for developmental intracranial complications, but in COM-Ch, damage to the ossicular chain occurred more frequently. 1 Our clinical observations are different. In the Otolaryngology Department of Medical University of Gdansk (in the period 2005-2009), 121 patients with COM-Ch and 38 COM-G were surgically treated. The most affected bones in COM-Ch were the scutum, tegmen, incus, and head of malleus. In patients with COM-G, erosion of the facial nerve canal and the horizontal semicircular canal were found more often and intracranial or intratemporal complications were more common. None of the patients had meningitis. Bone destruction of the tympanic cavity and complications were predominant in cases in which an active infection was found. High resolution computed tomography (HRCT) is a good method for the investigation of osteolysis of the ear canal and bone walls. This method makes it possible to visualize the bone destruction of the scutum, malleus, incus, tegmen, mastoid process, trabeculae, and semicircular canals (Figure 1).
The phenomenon of osteolysis can be explained through molecular analysis. The middle ear bone destruction in COM is activated and regulated by inflammation. Chronic otitis media with granulation is a highly active inflammatory process in which many cytokines are released. The bone is degraded by osteoclasts but at the same time protected by OPG. Osteoblasts synthesize the structural components of the intercellular substance of the bone and regulate the pool of active osteoclasts through the RANKL/OPG/RANK system. The influx of cells is controlled by cytokines, growth factors, adhesion molecules, and osteotropic hormones. Tumor necrosis factor-α, interleukin (IL)-1, IL-6, and OPG/RANKL present in cholesteatoma and granulation accelerate bone lysis and increase the destructive effect on the middle ear. This results in damage of the middle and inner ear and leads to hearing loss, thus significantly affecting patients’ quality of life. The degree of hearing loss in patients with COM-C is higher compared to those with COM-G.2-4