
Abstract
Chorda tympani schwannoma is a very rare tumor, with only 12 reported cases in the English literature. There are few reports on the diagnosis of chorda tympani schwannoma, and it is easily misdiagnosed. At present, surgery is recognized as a treatment for chorda tympani schwannoma. We describe the clinical course of a patient presenting with a chorda tympani schwannoma treated with surgical resection using a transcanal endoscopic approach, and the results after this treatment were satisfactory. Therefore, we accordingly advocate the minimally invasive method of transcanal endoscopic resection to maximize intraoperative visualization and reduce postoperative morbidity for middle ear tumors.
Introduction
Common lesions in the middle ear include cholesteatoma, glomus tympanicum tumor, schwannoma of the nervous structures traversing the middle ear (facial, Jacobson, and Arnold nerves), middle ear adenomas, and rhabdomyosarcoma. 1 Schwannomas are benign tumors of schwann cells that do not normally invade adjacent soft tissue or bone, but cause symptoms and bone destruction locally. 2 Although the chorda tympani is a branch of the facial nerve, chorda tympani schwannoma is considered an independent subgroup of facial nerve schwannomas because of its clinical characteristics. 3 The main clinical symptoms of chorda tympani schwannoma are audiological, and therefore, it is easily misdiagnosed. Furthermore, only intraoperative exploration can identify the source of the tumor. At present, there are few reports on the diagnosis of chorda tympani schwannoma, and even fewer reports on its treatment. Here, we report the clinical course of a patient presenting with a chorda tympani schwannoma and provide references for the diagnosis and treatment of chorda tympani schwannoma.
Case Report
A 31-year-old woman presented with a 6-week history of pulsating tinnitus on her left side. She had noticed progressive hearing loss on her left side, but had not pursued any medical intervention. She denied experiencing otalgia, previous otologic surgery, or trauma. Audiologic examination revealed conductive hearing loss on the left and normal hearing on the right. Pure tone audiogram showed conductive hearing loss with an air bone gap of 35 to 40 dB at frequencies of 250 to 4000 Hz, and a type C tympanogram on the left side. Facial function and taste were normal. Otoscopic examination revealed an intact and thickened tympanic membrane, and a mass could be seen slightly in the upper part of the tympanic cavity through the tympanic membrane.
Computed tomography (CT) and magnetic resonance imaging (MRI) of the temporal bone were performed. Computed tomography showed opacification of the left mastoid air cells, and soft tissue shadow of the left middle ear tympanum (Figure 1A). On MRI, an oval soft tissue signal was observed in the middle ear, displaying high signal intensity in T2 weighted image (T2WI), with a large section of about 0.9 × 0.3 cm (Figure 1B).
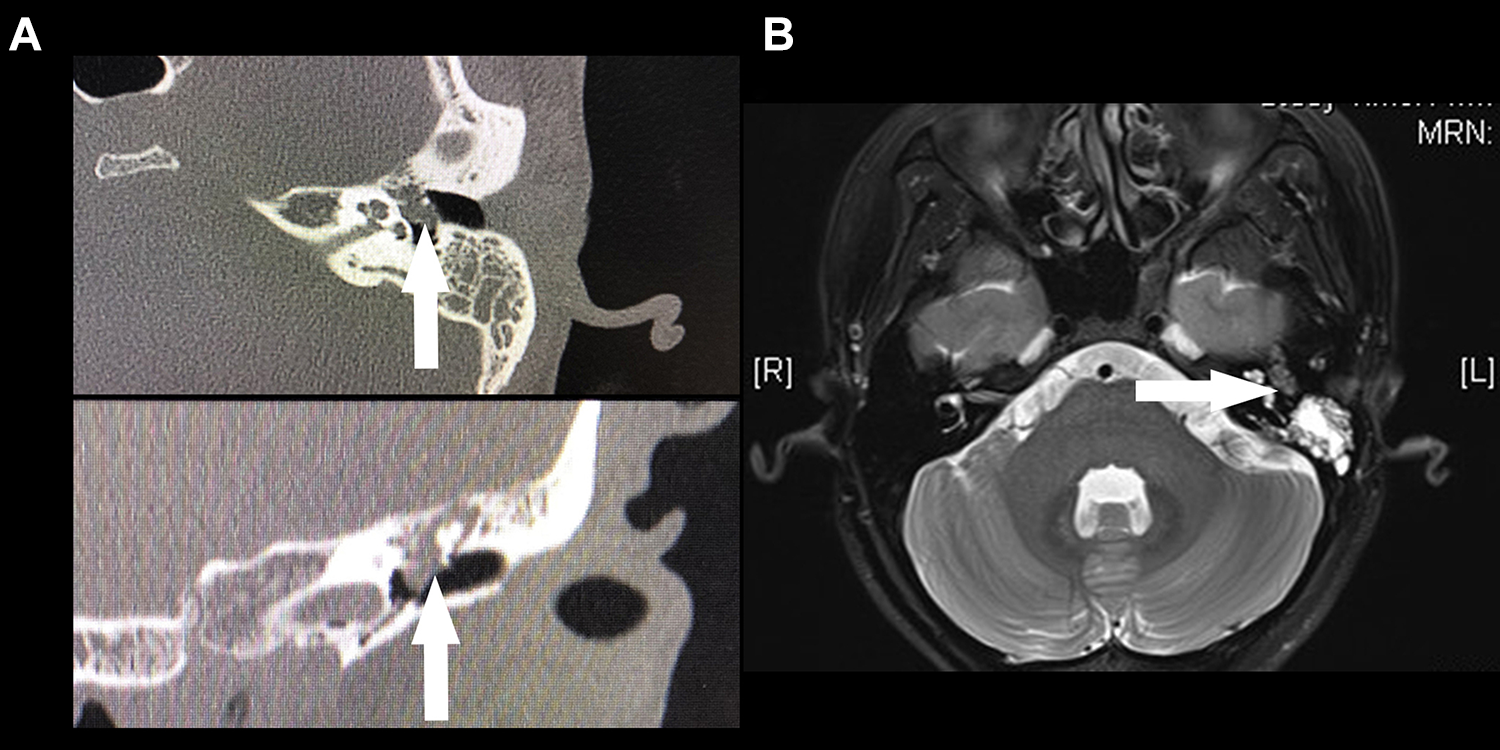
A, Computed tomography (CT) imaging (axial and coronal views of mass). B, Magnetic resonance imaging (MRI; axial view of mass). The arrows point to the mass. L = left, R = right.
The patient elected to undergo resection of the lesion using an endoscopic, transcanal approach with the senior author (Shudong Yu). Raising of the tympanomeatal flap revealed an irregular mass surrounding the ossicular chains in the middle and upper tympanic cavities. The mass was found to be emanating from the chorda tympani (Figure 2A). Frozen section (intraoperative) suggested a spindle cell tumor, which is considered to be derived from peripheral neurogenic tumors. In order to completely clear the tumor, we removed the incus, and the upper tympanic cavity was opened. After full exposure, the tumor was found localized in the tympanic cavity and did not enter the tympanic antrum. It could be seen that the anvil was basically intact, but the head of the stapes was missing (Figure 2B). The malleus, and the anterior and half of the posterior arch of the stapes remained. After complete removal of the tumor, the ossicular chain was reconstructed using an artificial ossicle (TORP, 11940, 4.0 mm, SPIGGLE & THEIS) inserted between the arch of the stapes (Figure 2C). Postoperatively, the patient experienced neither dysgeusia nor facial nerve paralysis. The final pathological assessment revealed the mass to be a schwannoma. The patient’s hearing returned to normal 1 month after the operation. Follow-up at 8 months showed the patient in good health without recurrent symptoms.
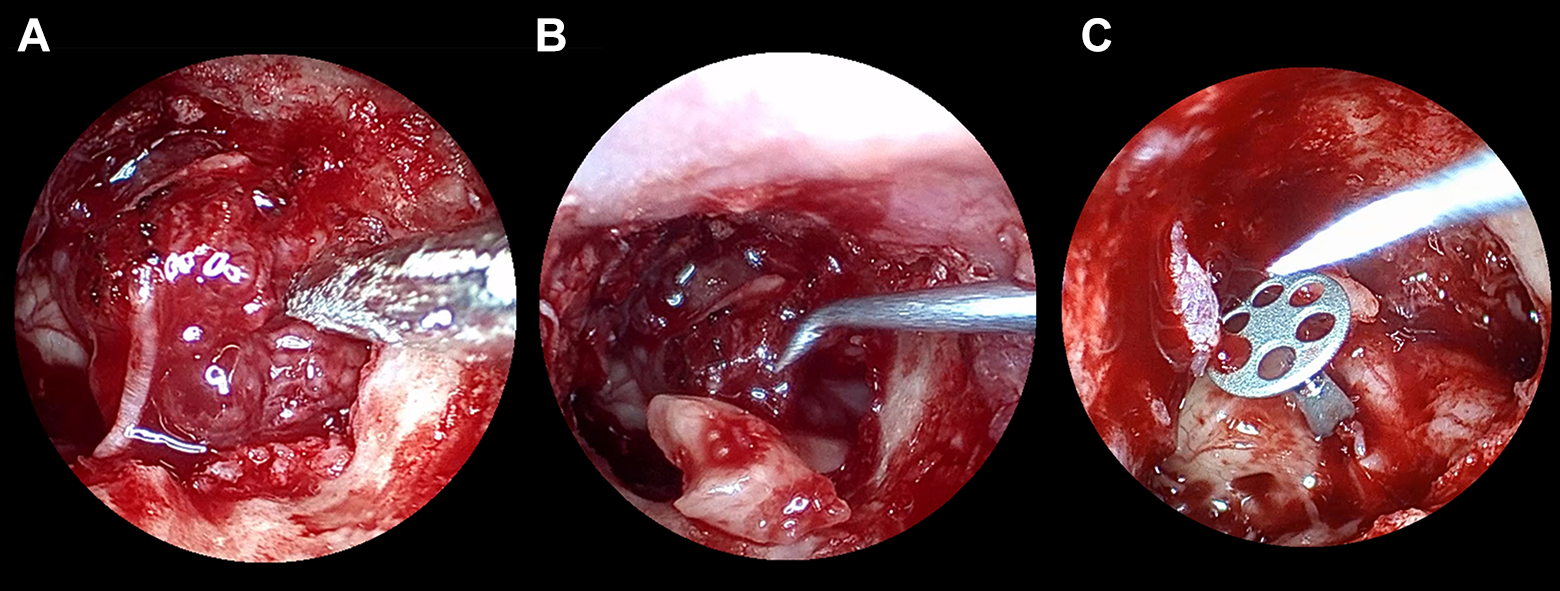
Intraoperative endoscopic view. A, An irregular mass is found emanating from the chorda tympani. B, The anvil is basically intact when the anvil was removed. C, Ossiculoplasty with an artificial ossicle is inserted between the arch of the stapes.
Discussion
About 25% of schwannomas are reported to occur in areas of the head and neck, 2 but chorda tympani schwannomas are exceedingly rare, with only 12 reported cases in the English literature.1,4,5 Only 2 cases of chorda tympani schwannoma have been clearly reported in the Chinese literature.6,7 In this case report, we describe the clinical course of a patient presenting with a chorda tympani schwannoma treated with surgical resection using a transcanal endoscopic approach.
In the cases that have been reported, the patient’s history is often more than 6 months or even years, while the history of our patient is only 6 weeks. This is the fastest diagnosis of a patient with chorda tympani schwannoma. We suspect that this is related to the rapid growth of this patient’s tumor. Conductive hearing loss and tinnitus are the most common presenting symptoms, and some patients display symptoms of facial palsy.3,6-8 Preoperative dysgeusia has not been reported in the current literature. Most cases show a mass obstructing the external auditory canal or behind an intact tympanic membrane.1,3,5-7,9 The clinical symptoms have no obvious specificity and are similar to other diseases, making chorda tympani schwannoma prone to misdiagnosis.
For the diagnosis of chorda tympani schwannoma, in addition to relying on the patient’s symptoms, signs, and audiometry, clinicians should also perform high-resolution CT scan and contrast-enhanced MRI of the temporal bone. Computed tomography often shows a mass in the tympanic cavity of the middle ear, and about 30% of cases of chorda tympani schwannoma have been described as bone erosion. In our case, preoperative CT only showed occupation of the tympanum, with no obvious bone destruction. However, we found that the head of the stapes was destroyed and missing during surgery. The bone destruction may be caused by tumor compression or factors secreted by the tumor; however, the underlying causes need to be further studied. Magnetic resonance imaging often demonstrates a circular, equal, or low signal intensity in T1WI, and high signal intensity in T2WI,4,7 in our present case. Although the specific manifestations of chorda tympani schwannoma on CT and MRI are helpful in the diagnosis and understanding of the lesion range and the surrounding anatomical relationship, which is of diagnostic relevance, it is still often necessary for the surgeon to determine the true source of schwannoma through surgery. The final diagnosis depends on the postoperative pathological analysis.
Surgery is currently recognized as a treatment for chorda tympani schwannoma. In almost all of the reported cases of chorda tympani schwannoma, successful tumor resections were performed. The conventional surgical method is the transmastoid operating microscope approach, although some surgeons use the transcanal endoscopic approach. There are 2 successful reported cases of endoscopic treatment of chorda tympani schwannoma via the external auditory canal,1,5 and our case provides further evidence that this treatment is feasible. Chorda tympani schwannoma occurs in the tympanic cavity, and rarely enters the tympanic antrum. Therefore, the endoscopic approach can be conveniently used for complete resection. Chorda tympani schwannoma is often localized and not associated with heavy bleeding, which makes endoscopic resection advantageous. In order to completely excise the tumor, the incus needs to be removed. Therefore, it is necessary to employ an artificial ossicle for hearing reconstruction after resection of the chorda tympani schwannoma, although it is also easily performed endoscopically. Notably, as shown from this report, the hearing outcome can be satisfactory. In addition to being minimally invasive, endoscopic resection is a better choice for chorda tympani schwannoma. This strategy can effectively shorten the operative time and reduce surgical complications. Thus chorda tympani schwannoma is ideal for endoscopic resection.
In summary, chorda tympani schwannoma is a very rare tumor. The primary symptom of chorda tympani schwannoma is hearing loss, which can be found on pure tone audiogram as conductive deafness. While CT and MRI scans can show a mass in the tympanic cavity. The symptoms are not unique to chorda tympani schwannoma, and therefore, it is difficult to diagnosis before surgery. Here, we described a rare case of chorda tympani schwannoma that was successfully managed with endoscopic resection without postoperative morbidity. We accordingly advocate the minimally invasive method of transcanal endoscopic resection to maximize intraoperative visualization and reduce postoperative morbidity for middle ear tumors.
Footnotes
Acknowledgments
The authors thank the ENT department of Shandong Provincial Hospital for their platform support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.