
Abstract
Lipomas, tumors of adipose tissue, are common and make up 16% of tumors of mesenchymal origin. Approximately 25% of lipomas occur in the head and neck region and are commonly found subcutaneously in places, such as the posterior neck. 1 The prevalence is higher among men than women, and often arise in the fifth or sixth decade of life. 2 Lipomas can further be categorized based on their histopathology into variants such as angiolipoma, chondrolipoma, spindle cell lipoma, or, in our case, osteolipoma. 1
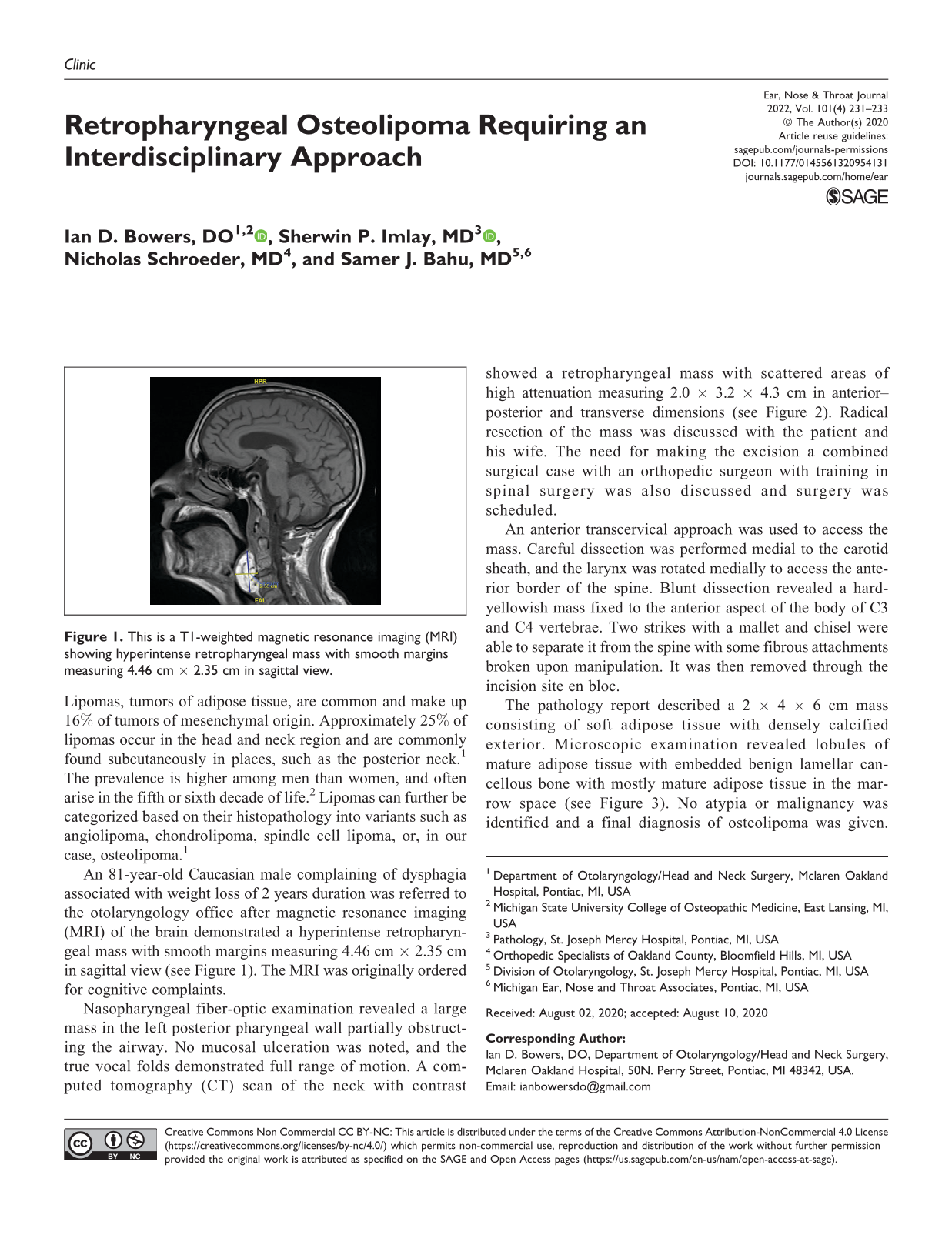
An 81-year-old Caucasian male complaining of dysphagia associated with weight loss of 2 years duration was referred to the otolaryngology office after magnetic resonance imaging (MRI) of the brain demonstrated a hyperintense retropharyngeal mass with smooth margins measuring 4.46 cm × 2.35 cm in sagittal view (see Figure 1). The MRI was originally ordered for cognitive complaints.
This is a T1-weighted magnetic resonance imaging (MRI) showing hyperintense retropharyngeal mass with smooth margins measuring 4.46 cm × 2.35 cm in sagittal view.
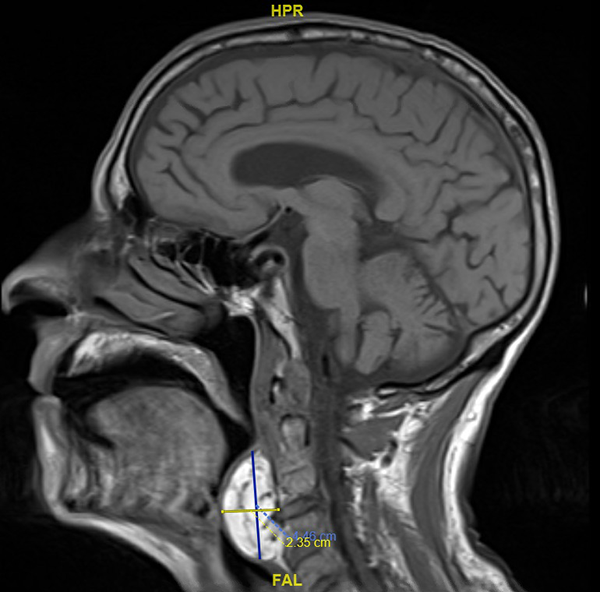
Nasopharyngeal fiber-optic examination revealed a large mass in the left posterior pharyngeal wall partially obstructing the airway. No mucosal ulceration was noted, and the true vocal folds demonstrated full range of motion. A computed tomography (CT) scan of the neck with contrast showed a retropharyngeal mass with scattered areas of high attenuation measuring 2.0 × 3.2 × 4.3 cm in anterior–posterior and transverse dimensions (see Figure 2). Radical resection of the mass was discussed with the patient and his wife. The need for making the excision a combined surgical case with an orthopedic surgeon with training in spinal surgery was also discussed and surgery was scheduled.
The above picture is a computed tomography (CT) bone window in coronal and axial views showing retropharyngeal mass with scattered areas of serpentine high attenuation representing calcification.
An anterior transcervical approach was used to access the mass. Careful dissection was performed medial to the carotid sheath, and the larynx was rotated medially to access the anterior border of the spine. Blunt dissection revealed a hard-yellowish mass fixed to the anterior aspect of the body of C3 and C4 vertebrae. Two strikes with a mallet and chisel were able to separate it from the spine with some fibrous attachments broken upon manipulation. It was then removed through the incision site en bloc.
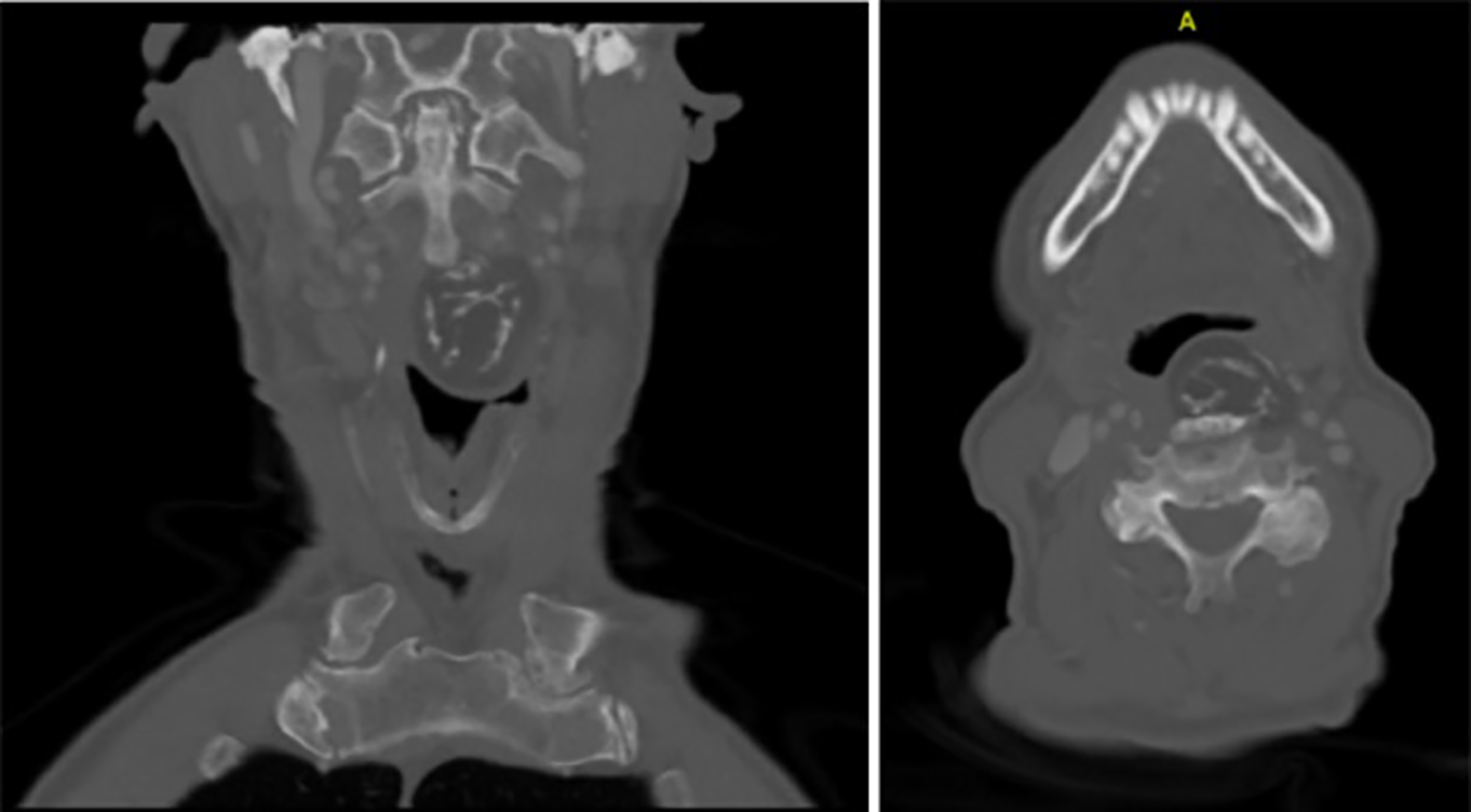
The pathology report described a 2 × 4 × 6 cm mass consisting of soft adipose tissue with densely calcified exterior. Microscopic examination revealed lobules of mature adipose tissue with embedded benign lamellar cancellous bone with mostly mature adipose tissue in the marrow space (see Figure 3). No atypia or malignancy was identified and a final diagnosis of osteolipoma was given. The patient was seen in the office on postoperative day 8 and again on day 29. His dysphagia symptoms greatly improved and the patient experienced positive weight gain. The patient’s wife, who is also his medical decision maker, provided written consent for the use of his medical information and images for this article.
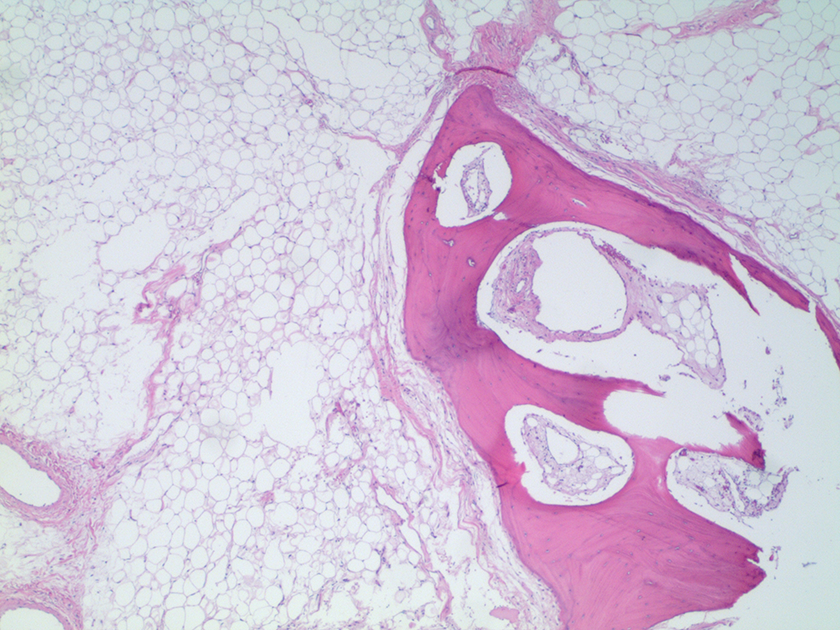
This is a microscopic histology slide (×2, hematoxylin-eosin stain) showing lobules of mature adipose tissue with embedded portions of benign cancellous bone of lamellar type with mature adipose tissue in the marrow space.
Osteolipomas are a rare variant of lipomas. They are described as benign tumors containing mature lamellar bone elements lacking hematopoietic cells within a larger tumor composed of mature adipose tissue. 3 Their clinical course is marked by slow progression with symptoms related to mass effect on the surrounding tissues. Approximately 20 cases have been reported in the scientific literature occurring in the extracranial head and neck region. 4 Of those 20, only one reported a case of an osteolipoma occurring in the retropharyngeal space. 3
The exact pathogenesis of osteolipomas is debated, with different theories appearing in the literature. One theory suggests that an existing lipoma undergoes bone formation that could be the result of repetitive trauma on the lipoma causing disruption of blood flow and subsequent ischemia and calcium deposition.5,6 The location of the lesion in the posterior oropharynx in our patient would leave it susceptible to continual microtrauma during the pharyngeal phase of deglutition.
There is no evidence in the literature of recurrence of osteolipomas after excision nor malignant transformation. They can be treated as a benign neoplasm and complete excision remains the treatment of choice.7,8 As was the case in the other previously described retropharyngeal osteolipoma, the mass was able to be removed completely and the patient reported significant improvement of his symptoms without complications. 3
Although we as otolaryngologists are comfortable working in the neck, the nature of the mass being firmly fixed to the anterior spine was concerning. Intraoperative input from a spinal surgeon proved vital as both the otolaryngologist and spinal surgeon added significant contributions during the surgery. This case demonstrates how an interdisciplinary approach can lead to positive patient outcomes in the operating room.
Footnotes
Authors’ Note
Samer J. Bahu is the senior author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.